Article Text

Abstract
Objective To establish the benefits of an early, tailored and low-cost exercise intervention in older patients hospitalised for acute coronary syndrome (ACS).
Methods The study was a multicentre, randomised assessment of an exercise intervention in patients with ACS ≥70 years with reduced physical performance (as defined by the short physical performance battery (SPPB), value 4–9). The exercise intervention included four supervised sessions (1, 2, 3, 4 months after discharge) and home-based exercises. The control group attended a health education programme only. The outcomes were the 6-month and 1-year effects on physical performance, daily activities, anxiety/depression and quality of life. Finally, 1-year occurrence of adverse events was recorded.
Results Overall, 235 patients with ACS (median age 76 (73–81) years) were randomised 1 month after ACS. Exercise and control groups were well balanced. Exercise intervention improved 6-month and 1-year grip strength and gait speed. Exercise intervention was associated with a better quality of life (as measured by EuroQol-visual analogue scale at 6 months 80 (70–90) vs 70 (50–80) points, p<0.001 and at 1 year 75 (70–87) vs 65 (50–80) points, p<0.001) and with a reduced perception of anxiety and/or depression (6 months: 21% vs 42%, p=0.001; 1 year 32% vs 47%, p=0.03). The occurrence of cardiac death and hospitalisation for cardiac cause was lower in the intervention group (7.5% vs 17%, p=0.04).
Conclusions The proposed early, tailored, low-cost exercise intervention improves mobility, daily activities, quality of life and outcomes in older patients with ACS. Larger studies are needed to confirm the clinical benefit.
Trial registration number NCT03021044.
- acute coronary syndromes
- quality and outcomes of care
- cardiac rehabilitation
Statistics from Altmetric.com
Introduction
The benefits of regular physical activity are well-recognised in the secondary prevention of cardiovascular disease.1 However, the use of exercise as part of regular treatment in healthcare vary largely.1 In recent years, the average age of patients admitted to the hospital for acute coronary syndromes (ACS) has significantly increased.2 Older patients with ACS show the highest risk of mobility limitation, sedentary behaviour and physical inactivity, further worsening short-term and mid-term prognosis.2 3 Previous studies showed that traditional centre-based cardiac rehabilitation programmes effectively improve physical performance and outcomes after ACS. However, in most cases older patients with ACS are less likely to be referred to or to participate in such programmes. Therefore, the implementation and maintenance of physical activity in this high-risk subgroup of patients is still an unmet clinical need.4 To fill this gap, we designed the Physical Activity Intervention for Elderly Patients with Reduced Physical Performance after ACS (HULK) trial.5 In this study, an early, individualised and progressive, low-cost exercise intervention including few supervised sessions and home-based exercises was assessed and compared with a health education strategy.5 We found that the proposed exercise intervention was associated with a high attendance rate and with significant increase in the time engaged in PA and the values of short physical performance battery (SPPB).6
The purpose of the present analysis from the HULK study was to assess additional differences in terms of physical performance, activities of daily living, anxiety, depression, quality of life and adverse events in the study groups.
Methods
Study design
The HULK study was a multicentre, investigator-driven, randomised clinical trial conducted at three sites across the Emilia-Romagna region (Italy).5 A detailed study outline, a list of the criteria used for inclusion or exclusion in the study and definitions of end points have been previously published.5
Study population
The main inclusion criteria were: i) age ≥70 years; ii) hospital admission for ACS and iii) SPPB score from 4 to 9 at the inclusion visit (30±5 days after hospital discharge). In agreement with previous studies, we excluded patients with values ≥10 because they were considered to have exceptional functional capacity, and those with an SPPB value ≤3 because of the limited possibility to recover.7 8 Main exclusion criteria were: multivessel disease with indication for surgical revascularisation or staged percutaneous coronary intervention, inability to be discharged to home, congestive heart failure (HF), left ventricular ejection fraction <30%, severe valvular disease.6 ACS diagnosis and patient management was according to current guidelines and internal protocols. ST-segment elevation myocardial infarction (MI), non ST-segment elevation MI and unstable angina diagnoses were based on the integration of symptoms, ECG changes and high-sensitivity cardiac troponin values and variations.
Randomisation
Screening of eligible patients, as well as baseline data collection, was performed during index hospitalisation for ACS, before hospital discharge.5 One-month later (inclusion visit), after re-assessment of inclusion/exclusion criteria and eligibility, patients were randomised either to health education (control group) or exercise intervention (experimental group).5 Randomisation was stratified using the following variables: sex (male vs female), clinical presentation (presence or absence of ST-segment elevation), SPPB value (4–6 vs 7–9 points).5 The procedures of study arms are summarised in the online supplementary tables 1 and 2.
Supplemental material
Health education group
The control group received a 20 min session with one of the study physicians.5 Both the patient and relatives attended these sessions. The study physician stressed the major issues related to a heart-healthy lifestyle and explained the importance of physical activity as a powerful and independent factor to improve cardiovascular health and minimise cardiovascular risk. A detailed brochure explaining the benefits of physical activity was provided to all patients (online supplementary file).5
Supplemental material
Exercise intervention group
The exercise intervention consisted of four supervised sessions (1, 2, 3 and 4 months after hospital discharge) combined with an individualised home-based exercise programme.5 Centre-based sessions were supervised by a sports physician and a nurse, and took approximately 30–40 min, including a moderate standardised treadmill-walk, and strength and balance exercises (detailed description is available in the online supplementary file).5 The programme has been previously shown to be useful in the estimation of cardiorespiratory fitness and the prediction of survival and hospitalisation.9 Based on the practice sessions, patients received a walking programme to perform at home, unsupervised. The exercise programmes were individualised, and consistent with current international recommendations. A selection of calisthenic exercises designed based on the Otago Exercise Programme was prescribed (online supplementary file).10 Participants were encouraged to perform the exercises three times per week (approximately 20 min).5 Adjustment of the type and intensity of the home-based exercise was made at each visit.5 At the end of the 4-month supervised session, a long-term home-based exercise programme was designed by the sports physician. The exercise programme was extensively described to the patient and family members. The next session was planned at 1 year (after the cardiological visit) and then repeated yearly. The patient and/or family member were free to contact the Sport Medicine Centre in case of doubts or request of additional information and/or clarification.
Study measurements
Patient demographic data, clinical diagnoses, laboratory data and treatments were recorded. The physical performance was assessed with the SPPB scale, gait speed and grip strength.5 SSPB values have been previously reported.6 Gait speed was measured using a 10 m distance and was expressed in metres per second (m/s).11 Grip strength was performed with the dominant hand and the elbow flexed 90°; three measurements were performed, and the highest value was considered.12 Quality of life and emotional health was assessed with the questionnaires EuroQol-visual analogue scale (VAS) and EuroQol-5 domains (5D).13 Functional capacity and social activities were evaluated using the advanced activities of daily living (aADL) developed by Rosow et al and Reuben et al.14 15 All scales and questionnaires were recorded at inclusion, 6-month visit and 1-year visit.
Study end points
After randomisation, patients returned for study visits at 6 and 12 months and then yearly. The results of the primary outcome (6-month value of SPPB) and of the 1-year SPPB values have been previously reported.6 A brief summary of these findings is reported in the ‘Results’ section. The end points of the present analysis were 6-month and 1-year values of grip strength, gait speed, Euro-Qol VAS, Euro-Qol-5D and aADL. In addition, laboratory data, medical treatments and the cumulative occurrence of death or adverse events requiring hospitalisation at 1 year were reported. The assessment staff was blinded to the intervention. Participants were asked not to disclose their assigned group and not to talk about their interventions during the assessment. All events were centrally adjudicated by the clinical events committee whose members were unaware of patient randomisation assignment.5 This research was done without patient involvement.
Sample size calculation and statistical analysis
A detailed description of sample size calculation and statistical plan has been previously reported.5 Briefly, we expected to find in the intervention arm an increase of at least one point in the 6-month SPPB score (SD of 2.5 points), compared with control group. In order to obtain statistical power ≥80% (alpha 5%), an overall sample size of 226 patients was needed.5 Continuous data were tested for normal distribution with the Kolmogorov-Smirnov test. Normally distributed values were presented as mean±SD, otherwise median value and IQR were used. Categorical variables were summarised in terms of counts and percentages. At each timepoint (baseline, 6 months, 1 year), comparison between groups was performed with t-test for normally distributed variables, with Mann-Whitney U test for those without normal distribution and with two-sided Pearson’s χ2 test for categorical variables. To assess the changes overtime (from baseline to 1 year timepoints, through 6-month timepoint) of grip strength, 10 m gait speed and EuroQol-VAS in study groups, the repeated measures analysis of variance was applied. All tests were two sided, and the statistical significance was defined as p<0.05. All analyses were intention-to-treat and were performed with Stata V.13 (StataCorp, College Station, Texas, USA).
Results
From January 2017 to April 2018, 479 older adults admitted to hospital for ACS were assessed for eligibility (figure 1). The final population consisted of 235 patients (figure 1 and table 1). The median age was 76 (73–81) years. Overall, 117 patients were randomised to control group whereas 118 patients to experimental group (figure 1). There were no substantial differences in the baseline demographics and clinical characteristics of the two groups (table 1).

Study flow chart. LVEF, left ventricle ejection fraction; NYHA, New York Heart Association; PCI, percutaneous coronary intervention; SPMSQ, Short Portable Mental Status Questionnaire; SPPB, short physical performance battery.
Baseline characteristics
Assessment of physical performance
Patients randomised to exercise intervention showed a significant and progressive increase in the time engaged in physical activity, as assessed by 7-day physical activity recall questionnaire and accelerometery.6 This was associated with an improvement of SPPB values in the experimental group (baseline 76–8 vs 6 month 98–11 vs 1 year 9,8–11 p for trend <0.001). On the contrary, SPPB values did not change in the control group (baseline 76–9 vs 6 month 75–8 vs 1 year 7,6–8 p for trend 0.7).6 Similar findings were found regarding grip strength and 10 m gait speed (table 2). After 6 months, grip strength was respectively 16% higher in the exercise intervention group than the control group and the improvement was maintained until 1-year visit (figure 2). In the intervention group, 10 m gait speed improved along the follow-up (baseline 0.59±0.2 vs 6 months 0.81±0.3 vs 1 year 0.85±0.5, p for trend <0.001). The changes were not significant in the control group (baseline 0.60±0.2 vs 6 months 0.63±0.3 vs 1 year 0.65±0.5, p for trend <0.6).
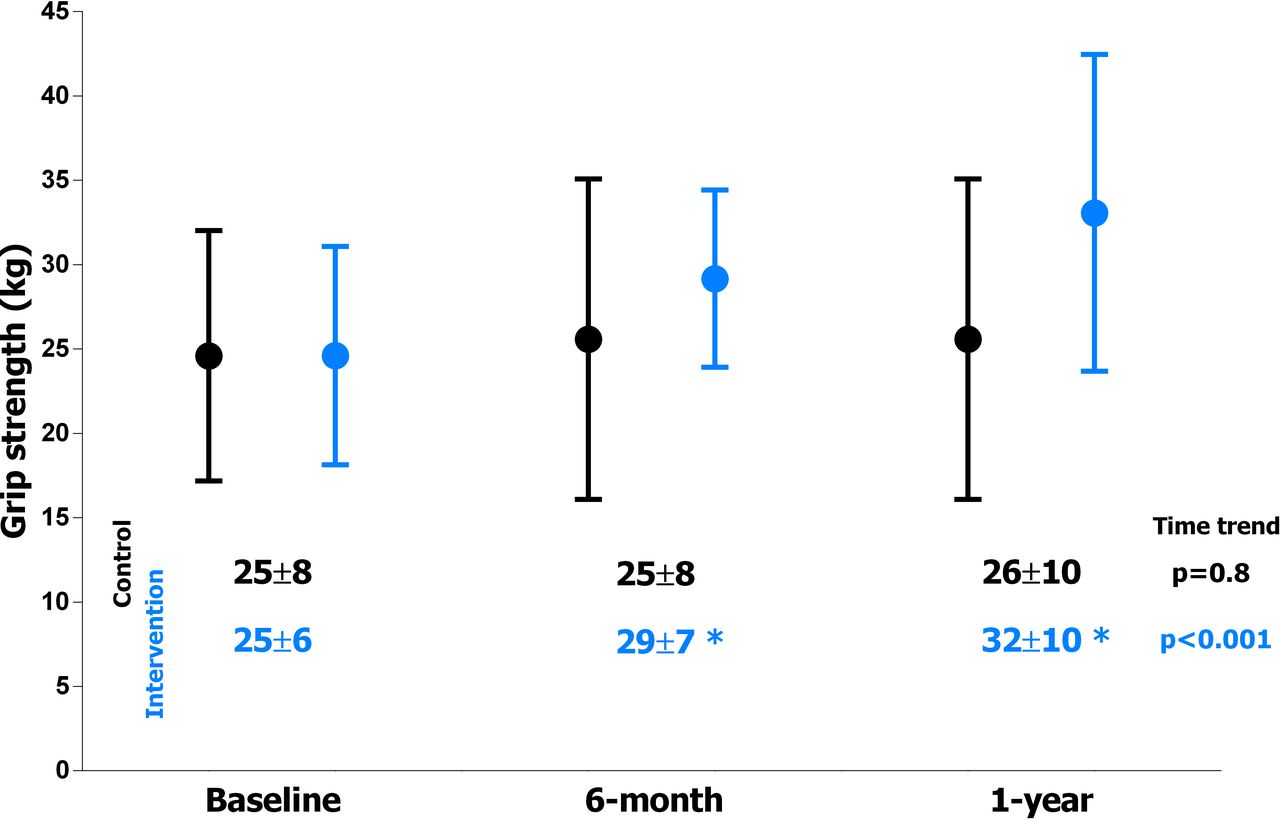
Grip strength in the study groups. Black: control group. Blue: intervention group. The circle represents the mean value, the line is the SD. *P<0.05 for the comparison vs control group in the single timepoint.
Outcome measures
Assessment of quality of life and emotional status
Quality of life as expressed by EQol-VAS significantly varied along the follow-up in the intervention group, but not in the control one (figure 3). At 6-month and 1-year visits, quality of life was better in the intervention group (table 2). Similar findings were obtained with the analysis of the EQol-5 domains questionnaire. The percentage of patients of the experimental group referring lack of pain or no problems in mobility and usual activities was higher in the intervention group (table 2). Anxiety/depression was significantly lower at follow-up visits in the intervention group (table 2 and figure 4).

Quality of life in the study groups, as assessed by EuroQol-visual analogue scale (VAS). White box: control group. Blue box: intervention group. The box represents the IQR, the line is the median and the whiskers are 5%–95% range. *P<0.001 for the comparison vs control group in the single timepoint.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Anxiety/Depression in the study groups, as assessed by EuroQol- 5 domains. *P<0.05 for the comparison vs control group in the single timepoint.
Assessment of functional capacity and social activities
The items of the aADL confirmed the benefits associated with the exercise intervention (table 2). Of note, self-reported ability to walk half of a mile was significantly higher in the intervention group than the control group (85% vs 55%, p<0.001) (table 2).
One-year clinical outcome
Table 3 summarises the main findings of 1-year visit. Low-density lipoprotein values were lower in the experimental group (table 3). Compliance to dual antiplatelet therapy tended to be higher in the intervention group (table 3). There were 4 (2%) deaths, all for cardiac cause, and 33 (14%) rehospitalisations, 25 of which for cardiovascular cause (table 3 and online supplementary table 3). The occurrence of rehospitalisation tended to be higher in the control group (18% vs 10%, p=0.09) and the main cause of admission was HF (table 3). The cumulative occurrence of cardiac death and hospitalisation for cardiovascular cause was 17% (n=20) in the control group vs 7.5% (n=9) in the experimental group (p=0.04).
Laboratory data, medical therapy and adverse events at 1 year
Discussion
The HULK study investigated the effects of a novel, early, tailored, combined centre-based and home-based exercise intervention compared with usual care among older adults (≥70 years) after a recent (1 month) ACS. The proposed exercise intervention was feasible, associated with high attendance rate and effective in improving time engaged in physical activity.6 This was associated with a significant improvement in the SPPB values at 6 and 12 months.6 The current analysis confirmed and expanded previous observation with several scales investigating physical performance, mobility, emotional status, daily activities and quality of life.
Grip strength and gait speed have been consistently found to be inversely associated with mobility, disability, hospitalisation and all-cause mortality in older adults.11 12 In a population of patients with cardiac disease, difference of 5 kg in grip strength was associated with a significant reduction in the risk of cardiac death, all-cause death and hospital admission for HF.12 The proposed exercise intervention was able to guarantee an increase of around 10 kg in grip strength both at 6-month and 1-year follow-up. Changes of 0.10 m/s for 10 m gait speed were generally accepted as clinically significant.16 In the current study, mean increments of 10 m gait speed were 0.18 m/s in the intervention arm, whereas they did not change in the control arm. The improvement in objective measures of physical function was paralleled by increase in the likelihood of being able to walk a half of a mile, a more relevant clinical outcome in everyday patient’s life.17 Due to the inclusion of patients with ACS (the occurrence of cardiac event is unpredictable), an objective measurement of the physical performance status immediately before hospitalisation is missing. Thus, it is unclear whether exercise intervention is associated with a true improvement (compared with physical performance before ACS) or whether it slows and/or stops the natural downward trajectory triggered by cardiac event. However, our findings show that immediately after an acute cardiac event, older patients are more prone to modify their lifestyle. In addition, we found that these lifestyle changes tend to be maintained over time. Indeed, despite the lack of supervised sessions between 6 and 12 months, the achievements in terms of physical performance and quality of life were largely confirmed at 1-year visit.
Recovering from cardiovascular disease and adjusting to subsequent life changes is a challenge for the patients. The study found a significant improvement in quality of life indices, including anxiety/depression profiles and improved functional/social activities in the intervention group. This is particularly notable given that no psychological intervention was included. Consistent with previous literature, the results of this study further suggest that a home-based approach may provide more psychological support than usual care.18
The major strength of the HULK study is the focus on the highly prevalent and increasing population of functionally impaired older patients after ACS. This subgroup of patients is at higher risk of lack of adherence to secondary prevention strategies, including compliance to cardioprotective drugs, and its cumulative occurrence of death and hospital readmissions is still impressive.19 Participation in exercise intervention might contribute to improve prognosis reducing adverse events. Although our study population is too small to draw any conclusion, we observed a trend supporting this hypothesis. Laboratory values (ie, low-density lipoprotein), compliance to 1-year dual antiplatelet regimen and adverse events tended to be better in the experimental group. Especially, we noted a consistent effect on hospital readmissions for HF. These data are not surprising and previous experiences showed the benefit of cardiac rehabilitation and exercise intervention in patients with HF.18 20 Exercise intervention improves functional capacity and cardiorespiratory fitness represented by VO2 peak.9 These parameters demonstrated to be related to a better prognosis, first in terms of HF hospitalisation.21
Limitations
The present study has several limitations. First, the exercise intervention was relatively short. Although the validity of the programme for a longer period must be demonstrated, we found that many favourable changes remain up to 1-year postevent. Second, selection bias due to the exclusion of patients with cognitive decline or disability and for those with severe left ventricular dysfunction might limit generalisability of the findings to older adults with more debilitated clinical conditions. Third, in the control group we applied a health education programme and not a traditional centre-based cardiac rehabilitation programme. This decision should be considered in the light of the study population inclusion criteria. We focused our attention in older patients with ACS with reduced physical performance at hospital discharge. No previous studies on cardiac rehabilitation selected a such frail and complex population. We can argue that a more engaging control programme could determine different results. However, it should not be forgotten that this vulnerable population receives the most frequent strategy of secondary prevention as the only health education.22 The aim of our study was to assess a first demonstration of safety, compliance and effectiveness of a novel programme of exercise intervention. Obviously, in future studies the equivalence of the proposed intervention as compared with standard cardiac rehabilitation should be investigated. Fourth, the open-label nature of the trial should be considered a further limitation. We minimised any potential bias dividing the teams performing exercise intervention and visits and applying validated tools performed according to validation rules. Finally, it remains to be proven whether the observed improvements in functional capacity also are associated with clinically relevant health outcomes.
Conclusions
The findings from the present prospective, multicentre, randomised trial of functionally impaired patients older than 70 years after ACS support the effectiveness of a novel, simple, individualised exercise intervention starting soon after discharge and continuing in the community. The largely home-based exercise intervention reduced anxiety and depression and improved quality of life. The benefits were maintained over time and up to the first year of follow-up. These findings may help to mitigate the challenges related to limited healthcare resources devoted to rehabilitation, including the paucity of rehabilitation facilities, particularly given that home-based interventions are cost-effective and the preferred choice of many patients.
Key messages
What is already known on this subject?
In older patients admitted to hospital for acute coronary syndrome, the presence of reduced physical performance is frequent and associated with a heightened risk of death and hospital readmission.
Traditional centre-based programmes improve physical performance and outcome, but older patients are less likely to be referred to or to participate in such programmes.
What might this study add?
The current investigation shows that an early, tailored, mainly home-based exercise intervention effectively improves several parameters of physical performance, daily activities and quality of life.
How might this impact on clinical practice?
The application of the proposed exercise intervention may improve quality of life and reduce the risk of recurrent adverse events in a large portion of vulnerable population, namely older adults admitted to hospital for myocardial infarction.
References
Footnotes
Twitter @RobertaCampan13
Contributors Conceived and designed the research: GC, ET, SB, SV, GG, GM, GC. Acquired the data: GB, MS, RR, FV, AR, SC, RC, GV, GS. Performed statistical analysis: GC, EM, SV. Handled funding and supervision: RP. Drafted the manuscript: GC, SB, EM, ET, RP, GG. Made critical revision of the manuscript for key intellectual content: JM.
Funding The study was an investigator-driven clinical trial conducted by the University of Ferrara.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, conduct, reporting or dissemination plans of this research.
Patient consent for publication Not required.
Ethics approval The study was approved by the ethical review boards at the participating hospitals. The study was conducted in accordance with the ethical principles of the Declaration of Helsinki.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available on reasonable request to corresponding author.