Article Text

Abstract
Despite an overall reduction in cardiovascular disease (CVD) mortality in the USA, the rate of coronary heart disease and CVD mortality is on the rise in younger women aged 35 to 54 years. This has been attributed to an increasing prevalence of CVD risk factors, which can portend disparate outcomes in women versus men. Women with diabetes and those who smoke have an excess relative risk of CVD when compared with their male counterparts. In addition to these discrepancies in traditional risk factors, a number of clinical conditions unique to women have been shown to increase CVD risks such as pre-eclampsia, gestational diabetes, polycystic ovary syndrome, early menopause and autoimmune diseases. The majority of these sex-specific risk factors can be identified at an early age, allowing for aggressive risk factor modification through lifestyle changes and, in certain patients, medications. The recently published 2018 American College of Cardiology and American Heart Association (ACC/AHA) hypercholesterolaemia and 2019 ACC/AHA primary prevention guidelines reflect this, citing pre-eclampsia, early menopause and autoimmune diseases as ‘risk enhancers’ that if present may favour initiation of statin therapy in borderline or intermediate risk patients. This comprehensive review addresses both traditional and unique risk factors of CVD in women, as well as sex-specific risk stratification and management options.
- cardiac risk factors and prevention
- pregnancy
- heart disease
Statistics from Altmetric.com
Introduction
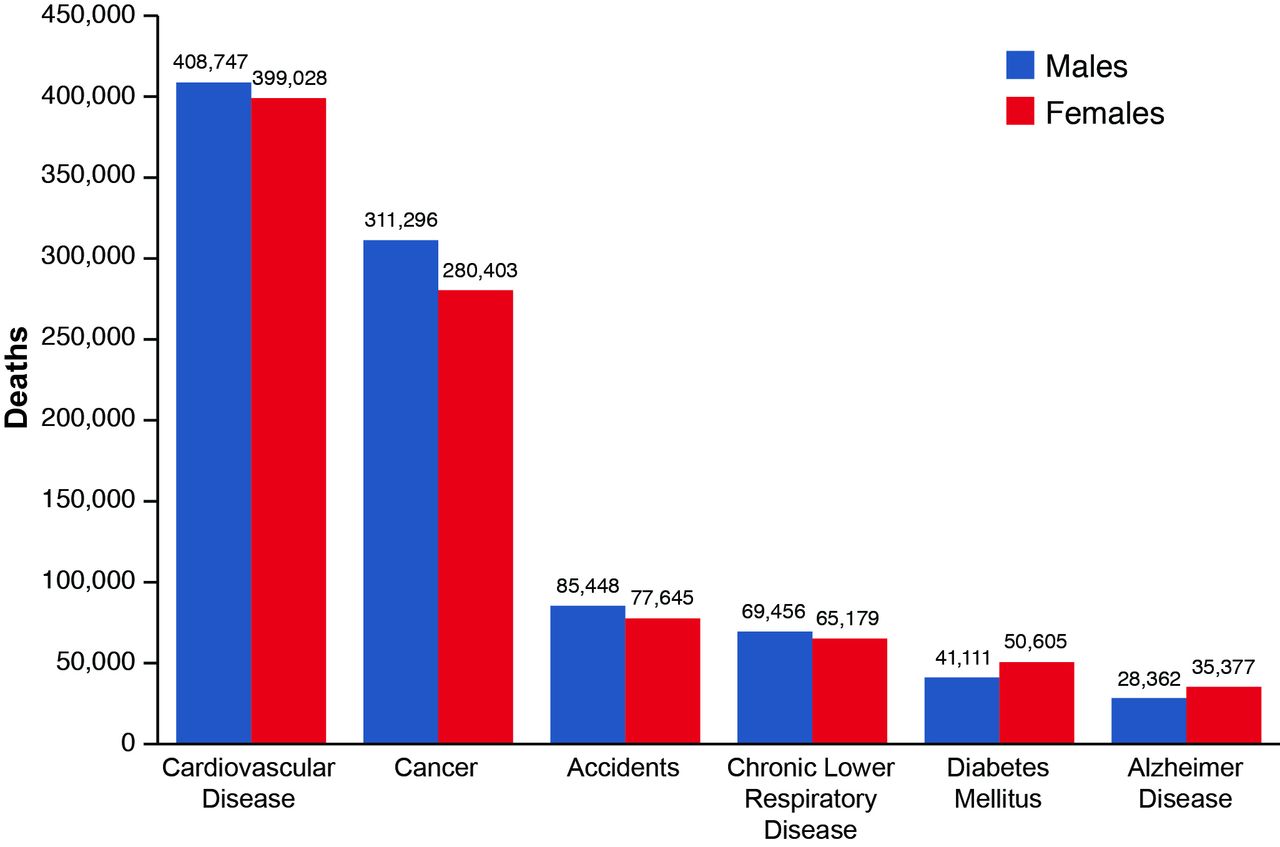
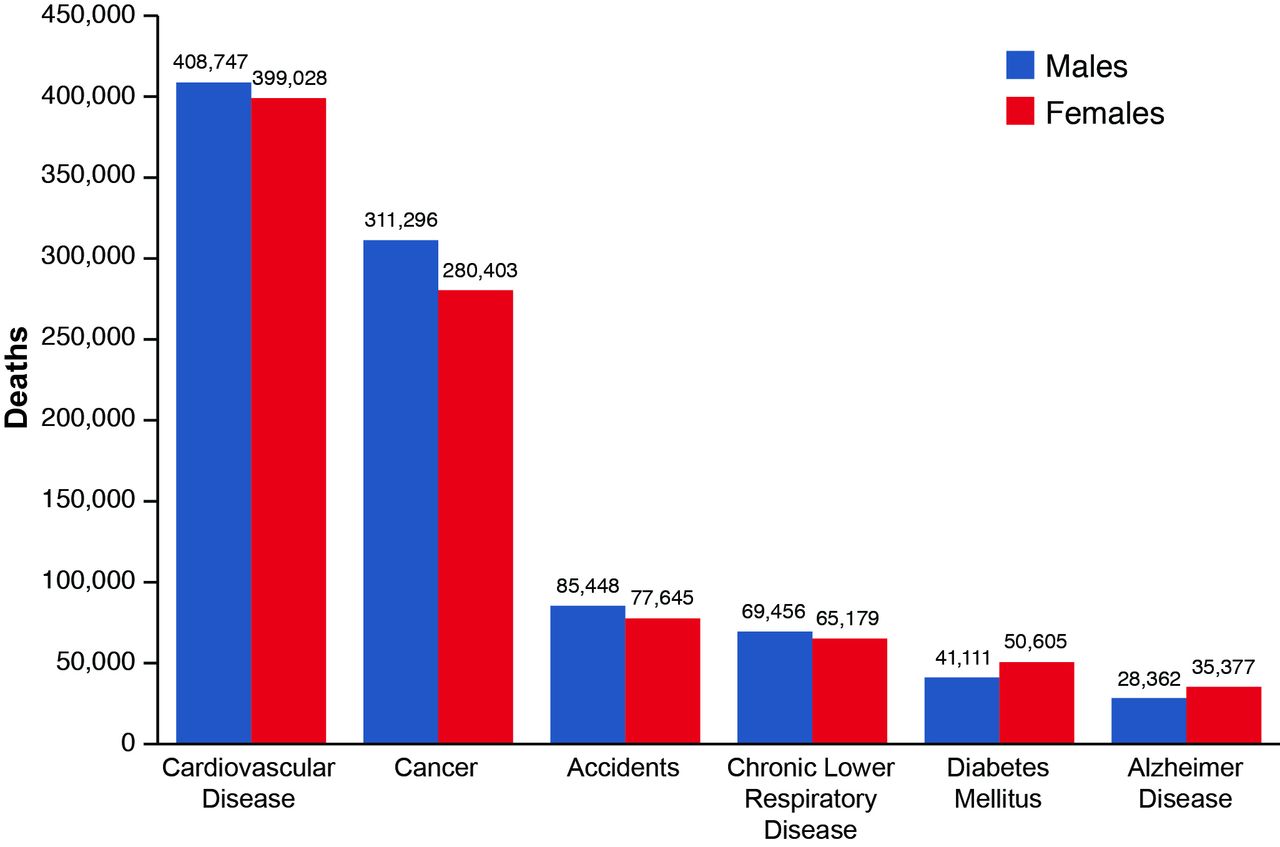
Stringent risk factor modification and early recognition of cardiovascular disease (CVD) for aggressive secondary prevention have led to a significant reduction in overall CVD mortality over the past few decades. However, despite these remarkable achievements, CVD remains the leading cause of death worldwide in both men and women. (figure 1)1 More alarmingly, the CVD mortality and acute myocardial infarction (MI) incidence rates are rising in younger women (35–54 years), likely a reflection of the Western obesity epidemic and increasing prevalence of associated CVD risk factors.2
{kind=link}
Comparison of major causes of death for all males and females in the USA: 2014. Adapted from 2017 Heart Disease and Stroke Statistics.1
Although recent efforts have significantly improved awareness of CVD among women, it is important to recognise that women are not an inherently homogeneous population. CVD rates remain significantly higher for African American women compared with their Caucasian counterparts and may be a reflection of the lower overall awareness of what CVD entails among black versus white women.3 There is a socioeconomic disparity within CVD as well, with low-income and middle-income regions accounting for over 80% of cardiovascular deaths.4
Although overall CVD mortality may be steadily decreasing, morbidity from CVD remains high as evidenced by substantial Disability-Adjusted Life-Year lost, largely attributed to an increasing burden of stroke and ischaemic heart disease.1 As such, there is now a concerted effort towards primary prevention of CVD. This review article serves to outline the unique differences in CVD risk factors for women and how these contribute to preventive strategies.
Traditional risk factors
In the early 1990s, there was concern regarding the applicability of traditional risk factors in women, as the vast majority of studies were predominated by a male population. Over the past couple of decades, increased awareness has allowed for sex-specific subgroup analysis, which has shown that traditional CVD risk factors are relevant to both sexes. However, although traditional risk factors for CVD can be defined the same in women and men, there are notable differences in the potency of risk factors that must be recognised to allow for sex-specific approaches to CVD prevention.
The SHEEP study, a case–control study in Sweden, demonstrated that women with diabetes mellitus (DM) had up to a sevenfold increased CVD risk compared with up to only threefold elevated risk in men with DM.5 Importantly, this increased risk portends not only the development of CVD in women but an increased mortality risk as well.6 These findings were confirmed in a collaborative meta-analysis of 68 prospective studies, where women with DM had a threefold increased risk of CV mortality versus double the risk in men with DM.7 The cause of this relative excess risk in women with DM remains unclear.
Increased awareness and advertising of the adverse effects of tobacco use have led to a marked decline in the prevalence of smoking in the USA, which has largely contributed to the notable fall in CVD mortality during this same time period. However, 13.7% of American women remain current smokers.1 8 Although women account for a smaller proportion of current smokers than men, tobacco use has been shown to be a more potent risk factor in women. A 2011 meta-analysis including ~2.4 million individuals showed that female smokers have a 25% greater risk of coronary heart disease (CHD) compared with their male counterparts (RR 1.25; 95% CI 1.12 to 1.39).9 Tobacco use is ultimately associated with half of all CV events in women and triples the risk of MI.10 Smoking cessation is the most cost-effective intervention in primary prevention of CVD and cessation therapies, both behavioural and pharmacological, should be offered to all tobacco users at each healthcare encounter.11
Gender differences
Although biological differences are those of each sex, gender differences are those related to sociocultural exposures and not typically reproducible in animal models. Depression and psychosocial factors have been shown to be a significant risk factor in both genders, but women have a notably higher prevalence of depression and greater attributable contribution to CHD.12 13 Women are more likely to be physically inactive than men, correlating with the higher prevalence of obesity in women compared with men.14 Lower socioeconomic status and education level in women have been associated with an excess risk of CHD compared with men.15
Risk factors unique to women
On average, women are affected by CVD 7–10 years later than men, which has been largely attributed to the protective effects of oestrogen during reproductive years. There are several cardioprotective mechanisms of oestrogen including antioxidant properties, increased angiogenesis and vasodilatation, reduced fibroblast proliferation and antiapoptotic properties.16 However, the marked reduction in oestrogen levels associated with menopause may account for the delayed clinical onset of CVD in women compared with men. However, there are a number of clinical conditions unique to women that have been identified to be associated with increased, and sometimes early onset, CVD risk Table 1undefined.
Comparison of current leading US cardiovascular risk calculators for women
Pre-eclampsia
Pre-eclampsia affects 3%–5% of all pregnancies and based on the updated 2013 American College of Obstetrics and Gynecology guidelines is defined as either new-onset hypertension with proteinuria or hypertension and significant end-organ dysfunction (with or without proteinuria) after 20 weeks’ gestation.17 The exact pathophysiology as to why pre-eclampsia increases CVD risk remains unclear. An early hypothesis was that pregnancy resembles a physiological stress test and may therefore simply unmask traditional risk factors of CVD, which may be more commonly associated with pre-eclampsia. A more recent study showed that compared with women with healthy pregnancies, women with pre-eclampsia are more likely to have abnormal lipid deposition within the spiral artery, which supplies temporary blood supply to the endometrium.18 The pathophysiology is thought to be due to impaired vascular remodelling, essentially resembling an accelerated atherosclerotic process and perhaps portends a predisposition to atherosclerotic CVD (ASCVD). Another hypothesis is that the resultant oxidative stress and inflammatory response caused by luminal narrowing of the spiral arteries may persist beyond the pregnancy, contributing to ongoing vascular dysfunction.18 Further research into the exact pathophysiology is necessary to confirm these hypotheses.
A meta-analysis by McDonald et al in 2008 examined CVD risk in 116 175 women with pre-eclampsia or eclampsia compared with women with uncomplicated pregnancies.19 They found that a prior diagnosis of pre-eclampsia was associated with almost a twofold increase in the risk of both CVD and CV mortality. They also notably identified a correlative relationship between severity of the patient’s pre-eclampsia and risk of CVD, with mild cases having a RR of 2 (95% CI 1.83 to 2.19) versus severe cases with a RR of 5.36 (95% CI 3.96 to 7.27; p<0.001).
These findings were confirmed by Wu et al, who performed a meta-analysis including 258 275 women with pre-eclampsia from 22 individual studies.20 They demonstrated a clear association between pre-eclampsia and future incidents of CVD and CVD mortality. This risk persisted even when adjusted for traditional risk factors including age, BMI and DM with an adjusted risk ratio of 1.8–2.5 except in heart failure, where there was a fourfold increased risk in those with pre-eclampsia.
Gestational diabetes
DM is a well-established traditional risk factor for the development of CVD, and so it should not come as a surprise that women with GD are at higher risk of CVD as well. This was recently confirmed in prospective cohort analysis of the Nurse’s Health Study (NHS) II, which included nearly 90 000 US women.21 GD was associated with a 43% increased risk of CVD (MI or stroke) compared with those without a history of GD at a median of 25.7 years of follow-up.
A more recent cohort analysis included over 1 million women and similarly showed increased CVD risk among those with a history of GD, with a 1.7-fold increased risk of hospitalisation for CVD up to 25 years post partum and most strongly associated with CHD.22 This held true when adjusted for baseline age, parity, time period, socioeconomic deprivation and pre-eclampsia, with a 2.14-fold increased risk of MI (95% CI 1.95 to 2.39). The incidence of cardiovascular hospitalisation for these women notably peaked at 8–15 years post partum, suggesting that primary prevention of CVD should be employed early in the post-partum period.
Although a large contributing factor in the mechanism of CVD development related to gestational diabetes (GD) is likely the increased risk for subsequent development of type 2 DM (in NHS II, 19% in women with GD subsequently developed DM vs 4.8% in controls),21 other mechanisms have been postulated. Early endothelial changes have been shown in women with GD, related to associated glucose intolerance. These effects can last beyond the pregnancy itself and several studies have demonstrated that women with a history of GD have higher rates of reduced coronary flow reserve, early atherosclerosis, and endothelial dysfunction when compared with controls.23 These findings again reiterate the importance of early and aggressive risk factor modification post partum, regardless of whether their glucose intolerance resolves, as prior vascular changes may persist post partum.
Polycystic ovary syndrome
Polycystic ovary syndrome (PCOS) is a heterogeneous syndrome characterised by a combination of polycystic ovaries, oligomenorrhoea and hyperandrogenism, with an estimated prevalence of 4%–8% in women of reproductive age.24 Although insulin resistance is not part of the diagnostic criteria, it is prevalent in 50%–70% of PCOS cases and is found to be independent of obesity.25 The resultant chronic hyperglycaemia has been hypothesised to have detrimental effects on the CV system, ultimately leading to increased CVD risk. However, individual studies on the association between PCOS and CVD have had controversial results.26 This is likely due to the fact that women with PCOS have a threefold to fivefold increased risk of developing DM, making it difficult to tease out the effect of PCOS from that of DM.
Zhao et al performed a meta-analysis including 104 392 women from 10 studies in an attempt to better ascertain whether there is an association between PCOS and CVD risk.26 They found that patients with PCOS were 1.3 times more likely to develop CVD than those without PCOS (95% CI 1.09 to 1.56), with a significantly increased risk of CHD (OR 1.44, 95% CI 1.13 to 1.84).27
A recent registry-based cohort study in Denmark compared women with PCOS and no prior diagnosis of CVD, hypertension or dyslipidaemia to age-matched controls.28 A total of 18 112 women with PCOS were identified with a median age of 29 years at diagnosis and followed for a median of 11.1 years. The incidence rate of CVD was significantly higher in women with PCOS (22/1000 person-years (PY) vs 13.2/1000 PY in controls, p<0.001), even when hypertension and dyslipidaemia were excluded as CVD diagnoses (6.4/1000 PY in PCOS vs. 4.5/1000 PY in controls, p<0.001).
Within a subgroup where clinical and biochemical data were available, women with PCOS who subsequently developed CVD were found to be significantly older with higher BMI, higher blood pressure (BP), more adverse lipid profile and less controlled DM. Notably, testosterone levels and sex-binding hormone globulin levels were comparable between the two groups.28 These findings suggest that increased CVD risk in patients with PCOS may be related to a metabolic syndrome picture, although further research is needed to fully understand the mechanism.
Early menopause
Up to 10% of women will experience early natural menopause, as defined by 45 years of age. The early loss of oestrogen has been postulated to result in chronic activation of the renin–angiotensin–aldosterone system, ultimately resulting in endothelial dysfunction and inflammation.29
In 2016, Muka et al published a meta-analysis including over 310 000 women to determine the effect of age at onset of menopause on CVD risk.30 Early menopause was considered to occur at <45 years of age, including both natural and surgical menopause; these women were found to have a 1.5-fold risk of CHD (95% CI 1.28 to 1.76) and importantly, a 1.19-fold increase in CVD mortality (95% CI 1.08 to 1.31).
More recently, Dam et al published a case–cohort study comparing incident CHD event rates between 5486 premenopausal women to 9916 postmenopausal women from 10 European countries.31 They found no significant difference in CHD risk between postmenopausal and premenopausal women once adjusted for confounders (HR 1.08, 95% CI 0.93 to 1.26, p=0.29). However, among postmenopausal women, there was a linear inverse relationship between earlier menopause and CHD risk whereby each 1-year decrease in age at menopause portended a 2% increased risk of CHD. Women with surgical menopause were at even higher risk than those who underwent natural menopause (HR 1.25, 95% CI 1.1 to 1.42, p<0.001).
With these findings in mind, early hypotheses suggested that hormonal therapy (HT) could help to ameliorate the risk of CVD in postmenopausal women. The Women’s Health Initiative randomised controlled trial included 16 608 postmenopausal women who were randomised to HT versus placebo for primary prevention of CHD.32 The trial was ended prematurely at a mean follow-up of 5.2 years due to trends towards CVD harm in those randomised to HT. There was a signal of increased CVD risk in women on the combined estrogen–progestin pill compared with placebo, whereas those on oestrogen alone had an increased risk of stroke compared with the placebo arm. Furthermore, there was an excessive risk of invasive breast cancer in the cohort of women taking estrogen–progestin HT. As such, current AHA/ACC guidelines recommend against HT for primary or secondary prevention of CVD.3
Autoimmune disease
Although autoimmune diseases are not unique to a specific sex, they almost universally disproportionately affect women. Although the incidence of the autoimmune disease usually lies within a younger cohort than CVD, the majority of deaths within these patients are related to CVD.33 The chronic inflammatory effects of autoimmune diseases have been shown to lead to accelerated atherosclerosis and endothelial dysfunction, clinically manifesting as premature CHD.34 Chronic steroid therapy can additionally lead to worsening hyperglycaemia and hypercholesterolaemia, exacerbating traditional risk factors of CVD within these patients.35 Early screening for and high clinical suspicion of CVD within this cohort are key in the aggressive reduction of morbidity and mortality.
Baena-Díez et al recently published a cohort study involving 39 057 individuals with the autoimmune disease but no known history of CVD.36 Overall, a diagnosis of an autoimmune disease was associated with an increased risk of CVD and all-cause mortality. Individuals with systemic connective tissue disorders or rheumatoid arthritis were found to have the highest risk of all study endpoints, including incident MI or stroke and all-cause mortality.
Risk stratification in women
The Framingham Risk Score (FRS) was first developed in 1987 based on a sample population from the northeastern USA. Last updated in 2008, its most recent version takes into account seven clinical factors: age, gender, smoking status, total cholesterol, high-density lipoprotein (HDL), BP and DM.37 Although the pioneer risk calculator only addressed risk of CHD events, additional CVD outcomes were included in subsequent versions. The current version comprises CVD mortality, MI and angina, heart failure, stroke and peripheral arterial disease as predicted outcomes.
However, external validation studies showed that using the FRS alone classifies up to 90% of asymptomatic women as low risk, grossly underestimating the true incidence of CVD.38 It was felt that relying on traditional risk factors alone to risk stratify women was misleading, as up to 20% of all coronary events occur in the absence of any traditional risk factors in women.39 In recognition of this, Ridker et al sought to develop a risk stratification tool that incorporated both traditional and novel risk factors, assessing 35 factors in a cohort of 24 558 healthy women who were then followed-up for a median of 10.2 years.40 On internal validation, the Reynolds Risk Score was shown to reclassify up to 50% of women from intermediate risk to either low or higher risk categories. External validation confirmed improved discrimination of the Reynolds score when compared with FRS and importantly, demonstrated reproducibility within non-Caucasian women.41 The clinical implication of the Reynolds score lies mainly within the appropriate use of statins for primary CVD prevention within this cohort of otherwise healthy, middle-aged women.
In 2013, the updated ACC/AHA guidelines for CV risk assessment included a novel risk calculator, the ASCVD Pooled Cohort Equations (PCEs).42 It included nearly 25 000 individuals aged 40–79 years old from five unique prospective cohorts and thereby was felt to provide a broader representation of the US population by allowing for four individual equations for African American and Caucasian men and women. Clinical risk factors similar to those used in FRS and Reynold’s risk score were used for the PCEs, though importantly with the inclusion of race (Table 1).
Although there have been some studies demonstrating reasonable calibration of ASCVD risk using PCEs,43–45 others have raised concern that PCEs overestimate risk in the general US population.46 Importantly, the emphasis within the 2013 guidelines was that the PCEs, as with any other risk stratification tool, should be used as a starting point for a shared decision-making conversation between the clinician and each individual patient as opposed to a tool for definitive treatment planning.
Conclusion and future directions
The first evidence-based, sex-specific guidelines for CVD prevention in women were first published by ACC/AHA in 2004 and since updated in 2007 and 2011. These guidelines succinctly outline the benefit of early risk factor identification within women and the potential for aggressive risk factor modification, which can begin simply at the recognition of pregnancy-related CVD risk factors or increased postmenopausal CVD risk. The 2018 ACC/AHA cholesterol guidelines reiterate these points, identifying early menopause and a number of pregnancy-associated conditions as risk enhancers for ASCVD (Box 1).47 Early identification and then aggressive risk factor modification with diet and exercise and in certain patients, drug treatment is key to lowering life-time risk of CVD.
Unfortunately, data have shown that this increased awareness of CVD risk in women has not yet translated into changes in standard clinical care. Studies have shown that women still receive less cholesterol screening, less lipid-lowering therapies, less cardiac rehabilitation referrals, and are less often prescribed antiplatelet therapy and beta-blockers for secondary prevention.48–50 Further outreach is necessary to ensure that primary care providers and cardiologists alike are attuned to the sex and gender disparities in the management of CVD risk.
Risk-enhancing factors for intermediate risk primary prevention treatment strategy
Family history of early ASCVD (<55 years in male FDR; <65 years in female FDR).
Primary hypercholesterolaemia (LDL-C 160–189 mg/dL, non-HDL 190–219 mg/dL).
Metabolic syndrome (>3 of the following):
Increased waist circumference (thresholds based on ethnicity).
Non-fasting TG >150 mg/dL and/or low HDL-C (<50 mg/dL in women).
Elevated BP and/or glucose.
CKD stage III-V, not treated with dialysis or renal transplantation.
Chronic inflammatory conditions (HIV/AIDS, SLE, RA, psoriasis).
History of premature menopause or history of pregnancy-associated conditions that increase ASCVD risk.
High-risk race/ethnicity (eg, South Asian).
Biomarkers
TG >175 mg/dL, non-fasting—persistently elevated.
Elevated high-sensitivity C reactive protein (>2.0 mg/L).
Elevated Lp(a) (>50 mg/dL).
Elevated apoB (>130 mg/dL).
Ankle-brachial index <0.9.
In patients with borderline (5%–7.5%) or intermediate (7.5%–19.9%) 10-year ASCVD risk, risk-enhancing factors may help individualise the shared decision-making conversation for a patient.
Adapted from 2019 ACC/AHA primary prevention guidelines.47
apoB, apolipoprotein B; ASCVD, atherosclerotic cardiovascular disease; CKD, chronic kidney disease; FDR, first degree relative; LDL-C, low-density lipoprotein, Lp (a),lipoprotein a; non-HDL, non-high-density lipoprotein, RA, rheumatoid arthritis; SLE, systemic lupus erythematosus; TG, triglyceride.
Five risk factors unique to or more prevalent in women
References
Footnotes
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Commissioned; externally peer reviewed.
Patient consent for publication Not required.