Article Text

Abstract
Objectives The goal of this study is to report the prevalence, aetiology and clinical outcome of pregnant women with heart failure.
Methods This is a retrospective community-based cohort study that included pregnant women in the Kaiser Permanente Health System between 2003 and 2014. Women with heart failure were identified using International Classification of Disease, Ninth Revision codes. Medical records were manually reviewed to confirm diagnosis and adjudicate outcomes.
Results In a cohort of 385 935 pregnancies, 488 (0.13%) had a diagnosis of heart failure, corresponding to 126 cases per 100 000 pregnancies. Peripartum cardiomyopathy was the most common cause of heart failure, accounting for 333 (68.2%) cases. Preterm birth and caesarean delivery were more common in patients with heart failure. Neonatal death rate was higher in the heart failure group (1.0% vs 0.4%, p=0.03). Infants delivered to women with heart failure had lower birth weights (3112.0±774.0 g vs 3331.9±575.5 g, p<0.001) and lower Apgar score at 1 min (7.9±1.5 vs 8.3±1.1, p<0.001). Median follow-up was 6.2 years (IQR 3.2–9.2). During follow-up, 7 (1.4%) in the heart failure group and 423 (0.11%) in the control group died. Heart failure was associated with a 7.7-fold increase risk of death (adjusted HR 7.7, 95% CI 3.6 to 16.4, p<0.001).
Conclusion Heart failure during pregnancy is associated with unfavourable fetal outcomes including prematurity and low birth weight. While the overall mortality rate was low, pregnant women with heart failure carried an excess risk of death compared with controls.
- pregnancy
- heart failure
Statistics from Altmetric.com
Introduction
Although heart failure is a relatively uncommon diagnosis among pregnant women,1 its incidence continued to rise over the past few decades.2 The US Centers for Disease Control and Prevention’s Pregnancy Mortality Surveillance System estimated heart failure and cardiomyopathy to account for about 11.8% of all pregnancy-related deaths in the USA.3
Pregnancy is associated with substantial haemodynamic changes to meet the increased metabolic demands of the mother and the fetus. These include a 30%–50% increase in cardiac output and plasma volume, partly through the activation of the renin–angiotensin–aldosterone system and sympathetic nervous system that cause increased salt and water retention. Women with heart failure are often unable to optimally respond to these hormonal and haemodynamic changes associated with pregnancy, especially during labour and delivery. In women with known cardiomyopathy, the increased volume load can lead to clinical decompensation because of impaired ventricular function and limited cardiac reserve.4
Heart failure in pregnant women can be due to pre-existing cardiac conditions such as dilated cardiomyopathy, hypertrophic cardiomyopathy, restrictive cardiomyopathy or ischaemic cardiomyopathy. Heart failure can also be related to peripartum cardiomyopathy, an acquired cardiomyopathy associated with pregnancy in women without known pre-existing heart disease.5 Management of heart failure in pregnant women can be challenging, because many standard therapeutic regimens for heart failure, such as ACE inhibitors or aldosterone antagonists, are contraindicated during pregnancy.6 Perhaps partly related to lack of effective therapy, studies have reported that women with cardiomyopathy may be at risk of having adverse maternal or fetal outcomes.7 8
Because heart failure in pregnancy is rare, there are limited data on the aetiology and associated short-term and long-term risks. Kaiser Permanente is a large integrated health maintenance organisation that provides medical care to more than 4 million members in Southern California. More than 20 000 deliveries occur at Kaiser Permanente hospitals in this region each year. Comprehensive medical records are maintained for all members and provide a good source of information for population studies. The goal of this study is to identify the prevalence, aetiology and clinical outcomes of heart failure in pregnant women using this population-based cohort.
Methods
Study population
This is a retrospective cohort study that included pregnant women in the Kaiser Permanente Southern California (KPSC) healthcare system between 1 January 2003 and 31 December 2014. Patients who were not Kaiser Permanente members or did not have continuous 1-year membership prior to date of delivery were excluded to allow adequate follow-up data. Women with a diagnosis of heart failure or cardiomyopathy prior to their deliveries, or within 6 months after their deliveries, were identified using International Classification of Disease, Ninth Revision (ICD-9) codes (425.x and 428.x). A detailed manual review of the medical records was performed by two physicians to confirm the diagnosis, identify aetiology of heart failure and adjudicate maternal and fetal outcomes. The Institutional Review Board granted a waiver of informed consent because of the observational nature of the study.
KPSC is a large group-model health maintenance organisation in California providing comprehensive medical care to more than 4 million members. Members reside in seven counties in Southern California (Orange County, Kern County, Los Angeles County, San Diego County, Ventura County, San Bernardino County and Riverside County), with broad representation of all ages and ethnicity. Health plan members have a demographic and socioeconomic profile similar to the overall Southern California population.9 Over 20 000 deliveries occur at Kaiser Permanente hospitals every year. Comprehensive medical records are maintained for all patients.
This study used computerised electronic health system databases, which include information on member enrolment, inpatient and outpatient diagnoses, pharmacy records and laboratory information. KPSC maintains a perinatal database that includes all births within the Kaiser Foundation hospitals with maternal and infant linkage using unique identifiers. The perinatal database includes maternal demographic characteristics, infant gender, gestational age at birth, birth weight, Apgar scores, delivery methods and pregnancy-associated complications.
Maternal comorbidities were identified by searching the KPSC Research Data Warehouse, which contains diagnoses from all ambulatory visits, emergency room visits and inpatient admissions, using ICD-9 Clinical Modification (ICD-9-CM) codes. The self-reported racial/ethnic data were obtained from California birth certificates. Aetiologies of heart failure were determined as documented by the treating clinician and confirmed by manual review of medical records.
Fetal birth weights were obtained from California birth certificates. Fetal medical conditions were identified by searching electronic medical records using ICD-9-CM codes. Small for gestational age was defined as having a birth weight below the 10th percentile for the corresponding gestational week. Low birth weight was defined as a birth weight of less than 2500 g (5 pounds 8 ounces). Very low birth weight was defined as birth weight less than 1500 g (3 pounds 5 ounces).
Statistical analysis
Descriptive statistics for categorical data were reported in absolute numbers and percentages. Continuous variables were analysed by calculating mean values and SD. Differences in categorical data between patient groups were compared by Fisher’s exact or χ2 tests. Differences in continuous data between patient groups were compared by Student’s t-tests (two tailed). P values <0.05 were considered statistically significant. Cox proportional hazard regression models were used to analyse between-group comparison of survival and estimate HRs with 95% CIs. Statistical analysis was performed using STATA IC V.14.
Results
Prevalence of heart failure
Among the cohort of 385 935 unique pregnancies in the study population, there were 488 cases of heart failure, corresponding to an overall prevalence of 126 cases per 100 000 pregnancies. The prevalence of heart failure varied by racial ethnic groups. The overall prevalence was 131 cases per 100 000 pregnancies in white women, 338 cases per 100 000 pregnancies in black women, 86 cases per 100 000 pregnancies in Hispanic women and 141 per 100 000 pregnancies in Asian women.
Aetiologies of heart failure
Among patients with heart failure, 333 (68.2%) had peripartum cardiomyopathy, 34 (6.9%) had non-ischaemic cardiomyopathy, 47 (9.6%) had congenital heart disease, 17 (3.5%) had valvular heart disease, 5 (1.0%) had ischaemic cardiomyopathy, 17 (3.5%) had hypertrophic cardiomyopathy and 35 (7.2%) had other aetiologies (table 1). Among the different ethnic groups, peripartum cardiomyopathy accounted for 89 out of 113 (79%) cases of heart failure in black mothers and 244 of 375 cases (65%) in non-black mothers. Diagnosis of heart failure was made prior to the index pregnancy in 161 cases (33%), during pregnancy in 61 cases (13%) and within 6 months postpartum in 266 cases (54%).
Baseline characteristics
Demographic and clinical characteristics
Table 1 shows the baseline maternal characteristics of the population. Compared with the control group of women with no heart failure, women with heart failure were older. Diagnoses including hypertension, hyperlipidaemia, obesity, diabetes, chronic kidney disease and coronary artery disease were more common in the heart failure group. Multigravida and multifetal pregnancies were more common in the heart failure group.
Obstetric events
Table 2 summarises the obstetric events. Pre-eclampsia and eclampsia were more common in the heart failure group: pre-eclampsia complicated 2.9% of pregnancies in the control group, whereas 9.2% of pregnancies in the heart failure group were complicated by pre-eclampsia. The rate of eclampsia was 0.08% in the control group and 0.6% in the heart failure group. Rates of gestational diabetes and postpartum haemorrhage were higher among women with heart failure.
Obstetric events
Gestational age at delivery was lower in the heart failure group (37.6±2.8 weeks in the heart failure group vs 38.8±2.0 weeks in the control group). Premature birth, defined as gestational age at delivery <37 weeks, was more common in the heart failure group (26% in the heart failure group vs 8.8% in the control group). A significantly higher proportion of heart failure patients underwent caesarean delivery (58.2% vs 28.9%, p<0.001).
Fetal outcomes
Fetal outcomes were summarised in table 3. Rates of neonatal deaths (including intrauterine fetal death or infant death within 28 days of delivery) were slightly higher in the heart failure group. There were 5 (1.0%) neonatal deaths in the heart failure group versus 1536 (0.4%) neonatal deaths in the control group. Infant birth weight was lower in the heart failure group (3112±774 g in the heart failure group vs 3332±576 g in the control group). Prevalence of infants with low birth weight (<2500 g) and very low birth weight (<1500 g) were higher in the heart failure group. Even after correcting for gestational age, a higher proportion of infants born to mothers with heart failure were small for their gestational age (table 3). Apgar scores of infants born to mothers with heart failure were lower. The proportion of infants with Apgar scores lower than 7 at 1 min, 5 min, and 10 min of birth were higher in the heart failure group compared with controls.
Fetal outcomes
Maternal mortality
The median follow-up period was 6.2 years (IQR 3.2–9.2 years). During the follow-up period, 7 (1.4%) in the heart failure group died and 423 (0.11%) of patients in the control group died. Figure 1 shows the Kaplan-Meier survival estimates for pregnant women with or without heart failure. Having heart failure during pregnancy was associated with a 7.7-fold increase risk of death (adjusted HR 7.7, 95% CI 3.6 to 16.4, p<0.001) (figure 2).
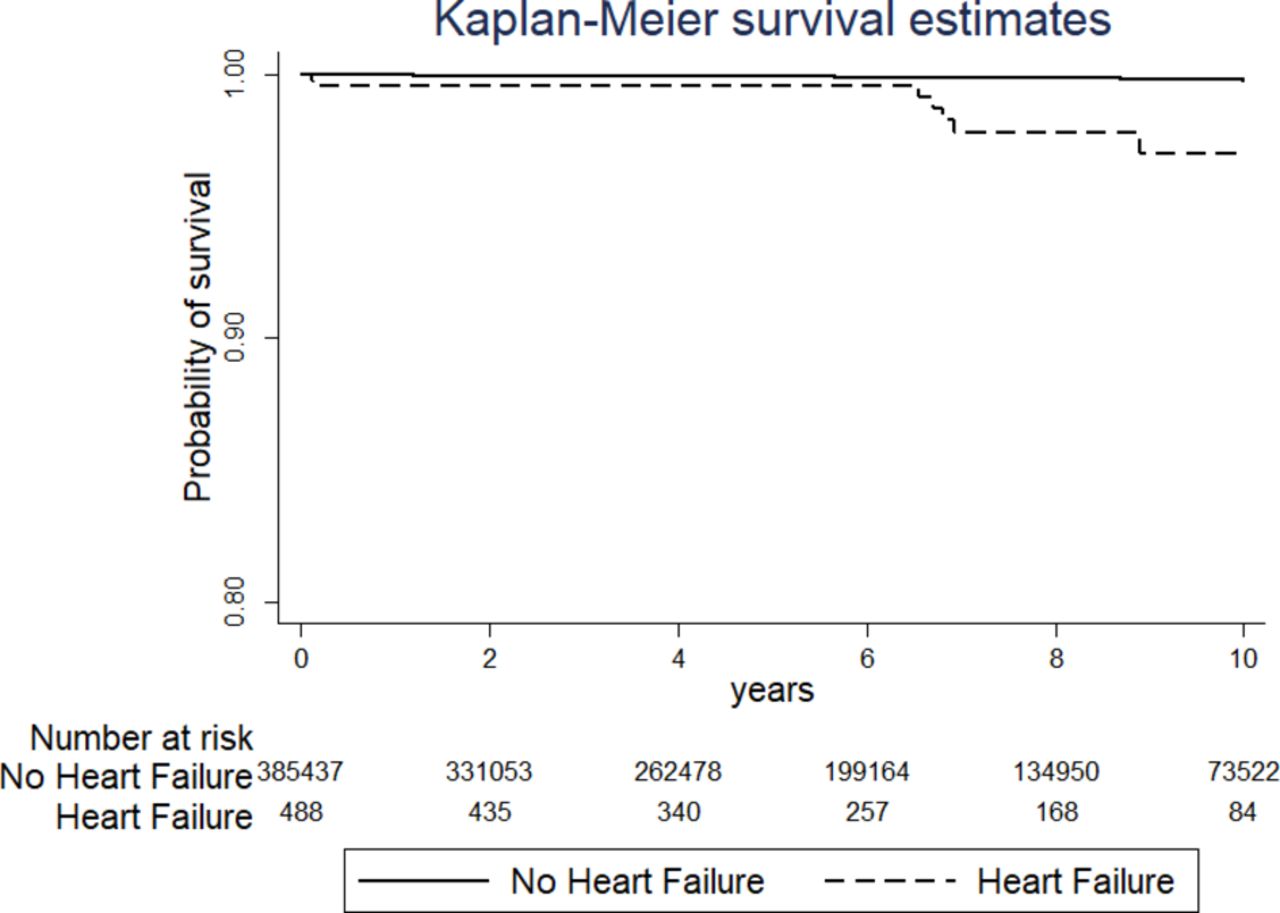
Kaplan-Meier survival estimates illustrating overall survival of pregnant women with or without a diagnosis of heart failure.

{kind=link}
{kind=link}
Risk of all-cause mortality associated with heart failure.
Discussion
In this population-based cohort study of pregnant women in Southern California with diverse racial ethnic background, we identified 488 cases of heart failure, corresponding to a prevalence of 126 cases per 100 000 pregnancies. Our estimate of prevalence is similar to those of other recent studies from the USA.10 The prevalence of heart failure was highest among black women (338 cases/100 000) and was lowest among Hispanic women (86 cases/100 000). The higher prevalence of heart failure among black women corresponded with increased prevalence of peripartum cardiomyopathy in this subgroup. A population study in North Carolina reported that peripartum cardiomyopathy was four times more common in black women than that of white women.11 Worldwide, higher incidences of peripartum cardiomyopathy were found in countries with a predominant black population such as Haiti and Nigeria compared with European countries with a predominant Caucasian population such as Denmark and Sweden.5 12 13 A combination of genetics and environmental risk factors may explain some of these differences. Given that patients in our study all resided in Southern California and are likely to have been exposed to a similar environment, the contribution of genetics to peripartum cardiomyopathy is probably much more significant in this cohort. Rare truncating variants in eight genes, including TTN (which encodes the protein titin) have been found to be prevalent in women with peripartum cardiomyopathy.14 Many of these truncating variants were found in women of African descent and may partially contribute to the increased predisposition to peripartum cardiomyopathy in this group.
In our cohort, peripartum cardiomyopathy was the most common cause of heart failure, accounting for 68% of all cases. Women with heart failure were more likely to have comorbidities such as hypertension, diabetes and renal insufficiency. Pregnancy-related conditions such as pre-eclampsia and gestational diabetes were also more common. The association with pre-eclampsia has also been seen in other studies10 and may be related to shared pathophysiological mechanisms. The failure to adapt to pregnancy-associated haemodynamic changes, along with activation of the renin–angiotensin–aldosterone system and sympathetic nervous system, predispose development of both hypertension and heart failure. Soluble Fms-like tyrosine kinase 1 (sFlt1) is another possible link between the two conditions. There is elevation in pre-eclampsia of placental sFlt1, a hormone that suppresses the vascular endothelial growth factor pathway and may trigger cardiomyopathy due to its vasculotoxic effects.2 15 Women with peripartum cardiomyopathy have elevated plasma sFlt1 level.16 In an animal model, sFlt1 administration has been shown to cause cardiomyopathy. These findings provide support for close monitoring of blood pressure and evidence for pre-eclampsia in women with heart failure.
In our cohort, premature birth was seen in 26% of the cases. The majority (58%) of patients with heart failure were delivered via caesarean delivery, significantly higher than in the control population. Neonatal death rate was higher in the heart failure group. A significantly higher proportion of infants were of low birth weight and very low birth weight. The Apgar scores of infants born to mothers with heart failure were lower. Despite significant progress made in the diagnostic evaluation and management of patients with heart failure, complications resulting in unfavourable fetal outcomes remain of concern. These observations underscore the importance of optimal management of maternal health, which is important to the health of the mother and to the health of the newborn.
The maternal mortality from heart failure in this study is lower than reported in some other studies that evaluated patients with cardiomyopathies and peripartum cardiomyopathy.17–19 One possible reason for the discrepant findings is that previous studies primarily enrolled patients referred to tertiary referral centres and likely included women with more advanced diseases. Patients from our study are drawn from the community and comprise the entire spectrum of heart failure disease severity and may have an overall better prognosis. More important is that all patients in our cohort have access to health insurance. The availability of medical care, especially having access to close follow-up care after delivery, may have led to improved survival. Lack of access to affordable, quality healthcare, especially during the postpartum period, has been suggested as a factor that might have partially contributed to the rising maternal mortality in the USA.20 The importance of early diagnosis and appropriate management of heart failure in pregnancy cannot be overemphasised.
Despite the overall low mortality rate compared with other studies, having heart failure during pregnancy was still associated with a 7.7-fold increase risk of death. While prepregnancy counselling and close monitoring are needed, future studies that focus on developing therapies for pregnant women with heart failure and improving systems of care delivery are particularly important.
Several limitations of this study should be acknowledged. This is a retrospective analysis, and as such the diagnosis and management decisions were likely to be not uniform in the study population as these were at the discretion of the treating clinicians. Cases were initially identified using ICD-9 codes, and it is possible that these codes did not capture all the cases. However, among cases identified, manual chart review was performed for all cases to allow for improved case ascertainment. Lastly, as our study drew its data from an insured population, there is an element of selection bias towards patients who have improved access to healthcare, and as such the findings may not be generalisable to patients in the USA who lack insurance or patients from developing countries with limited access to care.
Despite these limitations, this is a study of a geographically defined, racially diverse population, with a large number of pregnant women with heart failure managed according to contemporary clinical guidelines. Since heart failure in pregnancy is rare, findings from this large population-based dataset are invaluable in providing information on the prevalence, aetiology, complications and prognosis of this condition.
Key messages
What is already known on this subject?
Heart failure is an uncommon diagnosis among pregnant women, but its incidence is rising.
What might this study add?
We reported the prevalence, aetiology and clinical outcome of pregnant women with heart failure in a large contemporary community-based cohort. The prevalence of heart failure was 126 per 100 000 pregnancies. Peripartum cardiomyopathy was the most commonly cause of heart failure, accounting for 68.2% of cases. Infants delivered to women with heart failure had lower birth weights and higher neonatal death rates. Heart failure was associated with a 7.7-fold increase risk of death in the mother.
How might this impact on clinical practice?
Our findings underscore the importance of early diagnosis and treatment of heart failure in pregnancy, which is important to the health of the mother and to the health of the newborn.
References
Footnotes
Contributors Study concept and design: AT-YN and M-SL. Acquisition, analysis or interpretation of data: AT-YN, LD, TW and M-SL. Drafting of the manuscript: AT-YN, HTS and M-SL. Critical revision of the manuscript for important intellectual content: AT-YN, LD, HTS and M-SL. Statistical analysis: LD and M-SL. Administrative, technical or material support: AT-YN, LD and TW. Study supervision: M-SL. All authors have access to the data and share responsibility for the published material.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Not required.
Ethics approval The research protocol used in this study was reviewed and approved by the Kaiser Permanente Institutional Review Board.
Provenance and peer review Commissioned; externally peer reviewed.