Article Text

Abstract
Objective Spontaneous coronary artery dissection (SCAD) is a rare and potentially lethal cause of myocardial infarction (MI). The purpose of our study was to estimate the prevalence and maternal outcomes of pregnancies complicated by SCAD.
Materials and methods A population-based cohort study on all births identified in the Healthcare Cost and Utilization Project from 2008 to 2012. Disease prevalence was calculated and logistic regression was used to estimate the adjusted odds ratio (aOR) for risk factors and different maternal complications.
Results A total of 4 363 343 pregnancy-related discharges were evaluated. 79 cases of SCAD were identified resulting in a prevalence of 1.81 per 100 000 pregnancies. The mean maternal age at the time of diagnosis was 33.4 years (±5.2). Chronic hypertension (aOR, 2.67; 95% CI 1.18 to 6.03), lipid profile abnormalities (aOR, 48.22; 95% CI 24.25 to 95.90), chronic depression (aOR, 3.56; 95% CI 1.43 to 8.83) and history of migraine (aOR, 3.93; 95% CI 1.52 to 10.17) were associated with an elevated risk for SCAD. MI was diagnosed in 66 (85.5%) cases of SCAD with anterior and subendocardial territories being the most common locations. Thirty one patients (40%) with SCAD underwent angioplasty with the majority receiving stents, which was associated with a longer hospital stay than those treated conservatively or with bypass.
Conclusions SCAD is a rare aetiology of MI; risk factors and outcomes are illustrated in the current study. The puerperium is an important period for the development of pregnancy-related SCAD. Careful evaluation of pregnant and postpartum women with chest pain is warranted, especially if these risk factors are identified.
Statistics from Altmetric.com
Introduction
Spontaneous coronary artery dissection (SCAD) has been defined as a non-traumatic and non-iatrogenic separation of the layers of the coronary arterial wall by which a false lumen is formed. SCAD is a rare, devastating and potentially lethal cause of myocardial infarction (MI). The prevalence of SCAD is not well established as it is often underdiagnosed, having varied presentations from mild chest pain to sudden cardiac arrest and death.1 ,2 SCAD has been reported to account for 3–4% of patients presenting with acute coronary syndrome (ACS)3 as diagnosed by optical coherence tomography.1 ,4 It is recognised to be more prevalent in women and possibly most prevalent in young women.1 ,2 ,5
Presenting symptoms are typical of an ACS, including chest pain, dyspnoea, diaphoresis and/or nausea. Clinical findings that can lead to the diagnosis of SCAD include abnormal electrocardiographic findings, elevated cardiac biomarkers and regional wall motion abnormalities on echocardiography.6 As the typical patient is often young and healthy with no identified cardiovascular risk factors, SCAD may not be considered in the preliminary differential diagnosis.6 A higher index of suspicion and knowledge about this condition are prerequisites to an earlier and appropriate diagnosis of SCAD. Pregnancy is associated with significant changes in cardiovascular haemodynamics and cardiac disease often manifests during pregnancy and the postpartum period. The prevalence of SCAD in pregnancy has not been established, with most of the reported literature representing case reports and small case series or reviews,7 despite it being appreciated that pregnancy and the puerperium are major risk factors for the development of SCAD.1 ,7 ,8
Yip and Saw1 and Saw et al9 recognised different risk factors for the development of SCAD and described a possible new association with fibromuscular dysplasia (FMD). These risk factors included FMD, pregnancy, connective tissue disorders, systemic inflammation (eg, systemic lupus erythematosus) and stressful events. Clinically, SCAD is associated with the development of ST-elevation myocardial infarction (STEMI), non-ST-elevation myocardial infarction (NSTEMI), ventricular arrhythmias, cardiac arrest and death.10
Here, we describe a review of a national database to analyse possible risk factors, maternal outcomes and different interventions of patients diagnosed with SCAD during pregnancy and the puerperium.
Materials and methods
The Nationwide Inpatient Sample (NIS) from the Healthcare Cost and Utilization Project (HCUP) of the Agency for Healthcare Research and Quality (AHRQ) was queried for all pregnancy-related discharge codes for the years 2008–2012. The NIS is the largest all-payer inpatient healthcare database, containing all discharge data from more than 1000 hospitals, corresponding to a 20% stratified sample of US community hospitals. With more than 100 clinical and non-clinical data elements for each hospital stay, the NIS can be used to assess healthcare use and access, quality of care and outcome.11 ,12 These data include primary and secondary diagnoses, primary and secondary procedures, admission and discharge status, demographic information such as gender, age, race and median income for ZIP code, expected payment source, total charges, length of stay and hospital characteristics. The reliability of using such data has been examined on many occasions by different investigators to examine different pregnancy outcomes of rare diseases and their outcomes.13
Pregnancy-related discharges were identified using the International Classification of Diseases, 9th Revision (ICD-9) and were classified as antenatal, delivery and postpartum admission and discharges. To identify any pregnancy-related admission, we identified all pregnancy-related ICD-9 codes (ICD-9 codes 630–648) or delivery codes (ICD-9 codes 74 for caesarean delivery and 72, 73, 75, v27 or 650–659 for vaginal delivery). Postpartum admission consisted of discharge records that included a postpartum diagnosis (ICD-9 codes 670–677) and that did not also include a delivery code. For antenatal (predelivery) admissions, we excluded cases with delivery from the pregnancy-related group, dividing this group into those that delivered during the same admission record and those that did not. For our main exposure (SCAD), we used the ICD-9 code (414.12). For comorbidities and outcomes, both the ICD-9 code for a particular condition in pregnancy and the general ICD-9 code for that condition were used (see online supplementary table S1. ICD-9 codes were used). Once all targeted codes were identified, we constructed a historical cohort of pregnancies from 2008 to 2012. This cohort was used to perform a historical population-based study to identify different associated medical conditions and maternal complications in pregnancy-related SCAD. The Research Institute of the McGill University Health Centre approved the utilisation of this data set.
supplementary table 1
The ICD-9 codes used in identifying medical diagnoses and procedures.
Statistical analysis
To calculate odds ratios (ORs), we used logistic regression with CI of 95% for maternal age, race, maternal complications and obstetrical outcomes. The first logistic regression model was used to calculate the significance of different demographics (table 1). We constructed a single model for each of the demographic. Significant findings from this model were included in other models for adjustment. The second model was constructed to study different possible associations between different medical conditions and the occurrence of SCAD (figure 1 and see online supplementary table S1). For this model, we used a screening threshold for significance of p value of 0.25.14 All variables of significance were included in this logistic regression model.
Demographics
{kind=link}
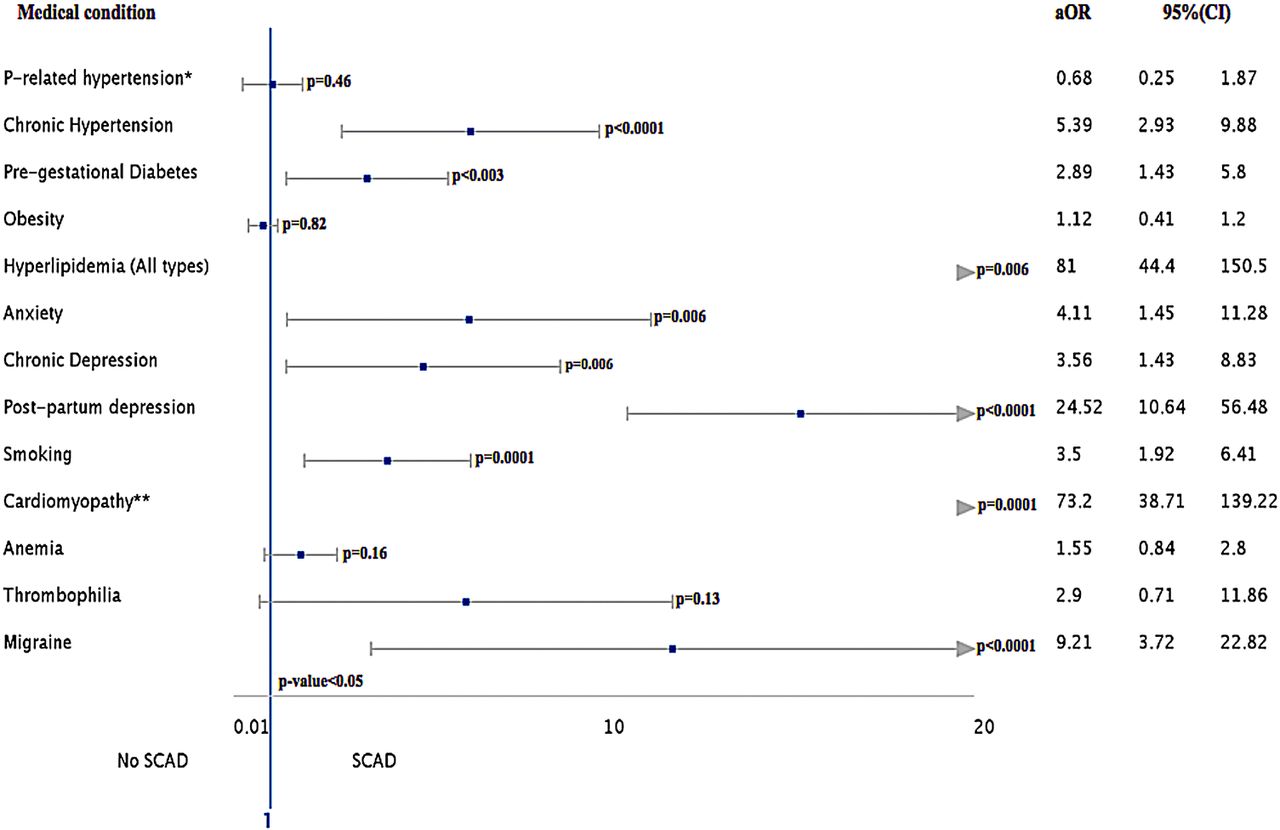
Adjusted odds ratios (aORs) for relevant medical conditions and their association with spontaneous coronary artery dissection (SCAD) in pregnancy and the puerperium. (*Pregnancy-related hypertension; **Prior or current cardiomyopathy; aOR, adjusted OR for maternal age, race and income; Crude OR are presented in online supplementary table S2).
supplementary table 2
Multivariable analysis of medical conditions suspected to be associated with spontaneous coronary artery dissection in pregnancy
To examine the maternal complications related to SCAD of all pregnancies, we used descriptive analysis using χ2 and Fisher exact tests when appropriate (table 2). Further subanalysis was performed on the cases of SCAD which were complicated by MI using multiple logistic regression for each of the maternal complications.
Maternal complications in pregnancy-related spontaneous coronary artery dissection (SCAD)
Adjustments for maternal age (in years as a continuous variable) and race were incorporated in the model for the logistic regression analysis. A p value <0.05 was considered significant. The results are presented as adjusted odds ratios (aORs). Statistical analysis was performed using SPSS© (V.23.0, IBM, Armonk, New York, USA).
Results
By analysing the data from 2008 to 2012, we extracted 4 363 343 pregnancy-related discharges. Of these, 281 200 (6.4%), 4 012 396 (92%) and 69 747 (1.6%) were antenatal, delivery and postpartum discharge diagnoses, respectively. A total of 79 cases of SCAD were identified resulting in a prevalence of 1.81 per 100 000 pregnancies. SCAD was diagnosed during the same admission as the delivery in only four cases (5.0%). Fifty-five (69.6%) and twenty (25.4%) cases of SCAD were diagnosed in the postpartum and antenatal periods, respectively. The mean maternal age at the time of SCAD diagnosis was 33.4 years (±5.2) compared with a mean of 27.6 years (±6.1) for mothers without SCAD. There was a progressively significant increase in the association between maternal age and SCAD, commencing with the 30–34 years age group (table 1). Black race was significantly associated with the development of SCAD (OR, 2.19; 95% CI 1.24 to 3.89). Different medical conditions were analysed using multivariable logistic regression to examine possible associations with SCAD (figure 1 and see online supplementary table S2). Gestational hypertension and pre-eclampsia do not appear to be associated with the development of SCAD; however, chronic hypertension is associated with an increased risk (aOR, 5.39; 95% CI 2.93 to 9.88). Lipid profile abnormalities were strongly related to SCAD (aOR, 81.00; 95% CI 44.40 to 150.50). An association was found between postpartum depression and an elevated risk for SCAD (aOR, 24.52; 95% CI 10.6 to 56.4); chronic depression also carries an increased risk (aOR, 3.56; 95% CI 1.43 to 8.83). Thyroid disease did not appear to be correlated, while there was an apparent association between migraine and the risk for SCAD (aOR, 9.21; 95% CI 3.72 to 22.82).
We also examined maternal outcomes that might be related to SCAD (table 2). MI was diagnosed in 66 (83.5%) cases of SCAD. The different locations of MI in SCAD and of MI without SCAD are illustrated in table 3. Pregnant and postpartum women with SCAD are more likely to develop STEMI rather than NSTEMI (aOR, 3.50; 95% CI 2.02 to 6.07). The site of MI in SCAD was most often anterior followed by anterolateral (table 3). Cardiac arrest occurred in 13.6% of patients with SCAD and ventricular fibrillation was more frequent (aOR, 4.53; 95% CI 1.70 to 12.05). There were three maternal deaths in this cohort representing a case fatality rate of 3.8% for SCAD in pregnancy and the puerperium and a 4.5% case fatality rate for SCAD complicated by MI. Case fatality rate for MI in pregnancy in general was reported at 5.1% in a previous study.13 Our analysis yielded an overall case fatality rate of 6% for MI in pregnancy. All deaths occurred in the postpartum period.
Maternal complications in patients with myocardial infarction (MI) with and without pregnancy-related spontaneous coronary artery dissection (SCAD)
Haemorrhage more frequently complicated cardiac procedures in the SCAD cases; however, the transfusion rate was not increased. Coronary artery stent insertion was performed in 32.9% of cases. Twenty-nine per cent (29.1%) of patients with SCAD required coronary artery bypass graft (CABG) with 5% of the cases undergoing angioplasty during the same admission. No CABG was performed after a stent insertion. There were 402 cases of MI diagnosed in this cohort. Overall, 16.4% were associated with SCAD. The differences in the procedures performed consequent to MI in pregnancy are presented in table 4. Cardiac catheterisation, angioplasty, coronary artery stenting and CABG were all performed more frequently in cases with MI complicated by SCAD compared with MI without SCAD (table 4). Of the three deaths in this database, two patients underwent cardiac catheterisation and CABG during the same admission. The third had a coronary stent and placement of a pacemaker. All three deaths were associated with acute subendocardial infarcts.
Procedures performed in cases of myocardial infarction in pregnancy
There does not appear to be an association between multiple gestation or grand-multiparity and SCAD as no such cases were found in the study cohort. Inherited collagen disorders (eg, Marfan's and Ehler–Danlos syndrome) and immune connective tissue disease were sought, but no cases were identified (see online supplementary table S1 provides a list of all diseases investigated). No specific coding was identified for FMD; therefore, this previously suggested association could not be evaluated. Fetal outcomes do not appear to be affected, as no cases of fetal death, growth restriction or prematurity were observed in this cohort; however, detailed neonatal outcomes cannot be evaluated using these data.
Discussion
Here, we present a cohort of SCAD evaluated in pregnancy and the puerperium. There are some limitations to the use of such population-based data sets. We acknowledge that these databases represent the discharge diagnoses and therefore do not allow the sequence or timing of events to be studied in a chronological fashion. However, these data do permit the evaluation of clinical outcomes and the identification of potential risk factors. Furthermore, some pertinent descriptors of disease and patient characteristics are not available within the data set, for example, the type of dissection or the specific coronary vessels involved. Another potential limitation is the risk of case duplication for patients who were transferred from one institution to another with included discharge data for each admission. By analysing different variables available in the data set, we identified two cases that may have represented interhospital transfers; however, we believe that in such cases it is more likely that the diagnosis of SCAD would be made in the receiving institution than in the referring hospital. We had two cases with a history of previous MI (2.5%), but the use of de-identified patient data does not allow such cases to be tracked. Additionally, cases diagnosed more than 6 weeks after delivery would not be included in the ICD-9 coding for the puerperium. In the study by Higgins et al,7 the mean time for postpartum presentation was 22.9±26.1 days (range, 3–90 days) and therefore late presenting pregnancy-related cases might have been missed. In cases with SCAD, eight cases (10.1%) had no invasive intervention performed and no invasive or non-invasive test could be extracted from the data set. There are non-invasive modalities that can be used to diagnose SCAD such as cardiac magnetic resonance, which might explain these cases; however, such examinations are not coded in the data set. Deaths occurring outside of a hospital would not have been captured in these data and might potentially have underestimated the case fatality rate.
Hormonal changes during pregnancy are thought to change normal elastic fibres, impair collagen synthesis and alter mucopolysaccharide content, causing weakening of the tunica media.1 Progesterone is thought to be the principal hormonal contributor, although in addition to this oestrogen contributes to pregnancy-associated hypercoagulability. The weakened coronary arterial walls together with the prothrombotic state of pregnancy increase the risk of dissection, the creation of a false lumen and of thrombosis.1 The prevalence of SCAD in this study population was 1.81 per 100 000 pregnancies. As SCAD has often been missed or underdiagnosed,1 this perhaps underestimates the true prevalence. The prevalence of SCAD in a general population presenting with ACS is estimated to be in the range of 3–4%,1 ,4 ,10 compared with 15.6% in our population. These data invite the question whether pregnancy and the postpartum period might be associated with an increased risk for the development of SCAD. An MI complicated by SCAD has a more complicated course and poorer outcomes (table 3). However, the presence of SCAD does not appear to alter the mortality rate of MI in pregnancy.
The classically recognised risk factors for coronary artery disease appear to be associated with the development of SCAD in our study. Hyperlipidaemia was significantly associated with the development of SCAD (aOR, 81.00; 95% CI 44.40 to 150.50). Acknowledging that the diagnosis of hyperlipidaemia in pregnancy can be challenging giving the physiological changes in the lipid profile associated with pregnancy, this finding should be interpreted with caution.15 Smoking and chronic hypertension also showed an association, but prepregnancy diabetes mellitus did not. Migraine has been reported previously as a risk factor for MI13 and we also observed an association with SCAD. It has been proposed by several authors that stressful events and depression might be associated with the development of SCAD1 ,6 ,16 and our study affirms this finding (figure 1).
The different procedures performed for patients with a diagnosis of SCAD are summarised in table 5.
Cardiac procedures performed in patients with spontaneous coronary artery dissection (SCAD) in pregnancy with mean length of stay (MLOS) in hospital
The management of SCAD is controversial and there are no management guidelines available. A conservative approach is reportedly preferred in patients who are stable, remote from the ischaemic event and who have a limited dissection demonstrated by angiography, as most dissections exhibit spontaneous vascular healing and do not require stenting.17 ,18 However, in the setting of ongoing ischaemia or injury risk to a significant myocardial territory, such as with a proximal left anterior descending artery dissection, percutaneous coronary intervention (PCI) is the treatment of choice17 and has been discussed and reviewed in previous reports.17–19
It is noted, however, that the rate of successfully managing an acute dissection with PCI is much less than that of an ACS due to atherosclerosis and patients with SCAD may experience less-than ideal outcomes.20 The coronary arteries are more friable due to the increased levels of progesterone in pregnancy and may exhibit ongoing dissection provoked by a PCI. Given the small sample size in this study and the inability to establish the chronology of events from the data set, it was not possible to evaluate procedure-related outcomes though no obvious correlations were observed.
The results show that patients with SCAD complicated by MI are at higher risk for CABG compared with patients with MI in the absence of SCAD (table 4); however, the results from these data cannot determine the optimal method of management given the small number of cases and the inability to analyse other factors that might have influenced decisions regarding interventions.
Conclusion
The significance of chest pain in pregnancy can be underestimated given the many confounding physical changes that arise in pregnancy such as gastro-oesophageal reflux and factors increasing the frequency of musculoskeletal pain. Although SCAD is a rare condition, it appears that it is more prevalent during pregnancy and in the puerperium, especially in patient presenting with ACS. Increased awareness of the importance of investigating a pregnant woman presenting with typical or atypical chest pain is vital. As women have been increasingly delaying childbirth21 and age is correlated with SCAD, advancing maternal age presents an increasing risk for the development of both MI and SCAD. Awareness of these risk factors might permit better identification of women at increased risk. However, further research is required to determine the clinical utility of evaluating older mothers for cardiovascular risk factors such as hyperlipidaemia and whether this knowledge would allow for monitoring or intervention strategies that might alter the natural history of this condition.
Key messages
What is already known on this subject?
Spontaneous coronary artery dissection (SCAD) is recognised to be more prevalent in women and possibly most prevalent in young women. Pregnancy and the puerperium represent a period of increased risk for the development of SCAD.
What does this study add?
This study establishes a prevalence of 1.81 per 100 000 pregnancies for SCAD in pregnancy. Most cases of SCAD appear to occur in the postpartum period (69.6%). This study demonstrates associations between SCAD and specific risk factors.
How might this impact on clinical practice?
Black race, chronic hypertension, hyperlipidaemia and migraine are factors demonstrating an association with SCAD in pregnancy and the puerperium. Clinical vigilance when evaluating pregnant and postpartum women presenting with chest pain and these characteristics is warranted.
References
Footnotes
Twitter Follow Majed Faden at @majfad
Contributors MSF contributed greatly to the analysis, organisation of the data and writing the manuscript. AB's effort in reviewing the manuscript, initiating the project and her valued input and participation were of pertinent importance in completing this project. NB input and evaluation from the cardiologist point of view was a cornerstone in this project. RNB provided a great valued input with providing the data and was an integral part of the team to write and review the manuscript.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.