Article Text

Abstract
Objective Surgery for aortic stenosis in patients with thoracic radiation therapy is associated with high morbi-mortality. Trans-catheter aortic valve implantation (TAVI) represents an alternative but has never been studied in this population. We aimed to compare outcomes in radiation and matched control patients undergoing TAVI and to identify predictive factors of survival.
Methods Between 2006 and 2011, 288 consecutive patients underwent TAVI in our institution, of whom 26 had previous chest radiation. They were matched 1:1 for age, sex and TAVI approach with controls.
Results In both groups, median age was 73 years, 50% of patients were male and 15% had a transapical approach. Procedural success was 88% in the radiation group versus 100% in controls (p<0.001) and 30-day survival was 92% in both groups. Five-year survival was 33%±10% in the radiation group and 42%±11% in controls (p=0.26). In radiation patients, the main cause of death was respiratory insufficiency in 40%. We identified four independent predictive factors of death in the radiation group: extracardiac arteriopathy (p=0.002) and the absence of β-blocker therapy (p=0.005) as preprocedural variables, and infectious complications (p=0.009) and a higher peak creatinine level (p=0.009) as postprocedural variables. In the radiation group, 89% of survivors were in New York Heart Association class I–II at last follow-up.
Conclusions Patients in the radiation group displayed high mortality rates although not significantly different from the controls. Respiratory failure was the main cause of death, emphasising the need for a careful pulmonary evaluation. Finally, we show a sustained improvement in functional results after TAVI in this population.
Statistics from Altmetric.com
Introduction
Cardiovascular diseases (CVDs) have become a leading cause of death among cancer survivors, partly because of therapy side effects.1 ,2 However, given the number of survivors, the long-term consequences of thoracic irradiation on the cardiovascular system have emerged.3 ,4 They include chronic constrictive pericarditis, coronary artery disease, cardiomyopathy, conduction disorders and valvular diseases such as aortic stenosis (AS).5 Radiation-induced AS usually appears two decades after the end of irradiation.6
Radiation exposure is also responsible for poor outcomes after cardiac surgery.7–9 In the largest published series, mortality was higher in patients with previous chest radiation, both at 30 days and long term.7 In the particular setting of severe AS, trans-catheter aortic valve implantation (TAVI) has emerged as an alternative to surgical aortic valve replacement (AVR) in high-risk patients. History of chest wall radiation is considered in the European and North American guidelines as a condition leading to favour TAVI over surgical AVR.10 ,11 However, although radiation patients are included in TAVI cohorts,12 no study has specifically reported the results of TAVI in this population.
The aims of this study were to (i) assess short-term and long-term (up to 5 years) outcomes after TAVI in patients with chest radiation therapy and severe symptomatic AS, and (ii) compare patients’ characteristics and outcome after TAVI to a matched control population.
Methods
Study population
Between October 2006 and April 2011, 26 consecutive patients with a history of chest radiation underwent TAVI in our institution for severe symptomatic AS, after evaluation by our multidisciplinary Heart Team. These 26 patients represent 9% of the 288 TAVI procedures performed during this period. This radiation group was matched 1:1 for age, sex and TAVI approach with a control population who underwent TAVI within the same timeline. Patients’ characteristics of the radiation group and the control group are detailed in table 1.
Comparison of the main characteristics of the radiation-exposed population and the matched controls
Index hospitalisation
Coronary angiogram was systematically performed before the index procedure. Extracardiac arteriopathy was defined according to the EuroSCORE II.13 To assess comorbidities, the aged-adjusted Charlson comorbidity index was used in addition to usual risk scores.14 Moreover, we used the France 2 score, which was specifically designed for TAVI.15 The variables of the France 2 predictive score are detailed in online supplementary table S1.
Supplementary table
France 2 score of individual risk assessment predictive of 30-day or in-hospital mortality after trans-catheter aortic valve implantation.
Both the Edwards SAPIEN and the Medtronic CoreValve System were used, as previously described.16 TAVI approach was selected according to the anatomy of iliofemoral arteries. Transfemoral access was favoured as the first approach.
Follow-up
Follow-up was conducted through clinical visits or phone calls to the referring cardiologist or to the patient. Data were prospectively entered in a computerised database.16 Follow-up was concluded in December 2014. Patients with last information before January 2014 were considered lost to follow-up. Quality of life (QoL) was assessed using the EuroQoL.17
The events taken into account were death, detailed as cardiac or non-cardiac according to the Valve Academic Research Consortium-2 (VARC-2) criteria,18 and New York Heart Association (NYHA) functional class III or IV at last follow-up.
Statistical analysis
Quantitative variables were expressed as median and (25th–75th) percentiles while qualitative variables were expressed as numbers and percentages. Comparisons between matched groups were made using Wilcoxon rank paired test for quantitative variables and a McNemar χ2 test for qualitative variables (to detect discordance between pairs with a high statistical power). Comparisons before and after the TAVI procedure in the same group of patients were performed using a Wilcoxon rank paired test. Survival curves were obtained with Kaplan–Meier estimates. Comparisons between survival curves were obtained using paired log-rank test. Univariate analysis of the predictive factors of death after TAVI was performed using a Cox model on the variables from table 1. Variables with p<0.10 were entered in a multivariate Cox model and selected by a backward procedure with a threshold of p=0.05. The variable ‘heart rate’ was not included in the multivariate model given a collinearity with the use of β-blockers. The results were considered significant when two-sided p values were <0.05. All analyses were performed using the SPSS statistical software (SPSS V.19, Chicago, Illinois, USA).
Results
Study population: radiation group versus control group
The main characteristics of the 26 patients who had a history of chest radiation and their matched controls are detailed in table 1. In both groups, median age was 73 years, 50% of patients were male and 15% had a transapical approach. Indications for thoracic radiation therapy were breast cancer in 11 patients and Hodgkin's disease in 11, while 2 patients had lung cancer, 1 a testicular seminoma and 1 a throat cancer. The median duration between TAVI and the last thoracic radiation therapy was 30 (14–40) years. Body mass index was significantly lower in the radiation group compared with controls (22 kg/m2 vs 28 kg/m2, respectively, p<0.002). Patients in the radiation group also presented with a higher heart rate at admission than controls (85 bpm vs 68 bpm, p<0.02) despite a trend for more frequent use of β-blocker therapy. The two groups did not differ according to their Charlson Index, common surgical risk scores and the France 2 risk score (table 1). Ten patients in the radiation group (38%) also had chemotherapy without significant difference in left ventricle ejection fraction compared with patients without chemotherapy (58 (35–60)% vs 60 (50–60)%, respectively, p=0.49).
Immediate results
Procedural success was achieved in 23 patients (88%) from the radiation group and 26 controls (100%) (p<0.001) according to VARC-2 criteria.18 In the radiation group, one implantation failed with migration of the prosthesis in the aorta and no implantation of a second prosthesis, one patient needed the implantation of a second prosthesis due to malposition of the first valve with good final results and one patient died during the procedure (from an annular rupture on heavily calcified bicuspid valve during balloon post-dilatation for aortic regurgitation (AR)≥3/4).
In the radiation group, median aortic valve gradient was 47 (41–57) mm Hg at baseline and 10 (7–12) mm Hg at day 7 (p<0.0001) and for control patients it was 52 (46–65) mm Hg at baseline and 11 (10–12) mm Hg at day 7 (p<0.0001) (figure 1). At day-7 echocardiography, there was no significant difference between the two groups regarding the aortic gradient and para-prosthetic AR was ≥2/4 in two patients (8%) of the radiation group and one (4%) in the controls (table 1).

Mean aortic gradient before and at day 7 after the trans-catheter aortic valve implantation (TAVI) procedure in patients from the radiation group (A) and the control group (B).
30-Day outcomes
The 30-day events are detailed in table 2 for both groups.
30-Day outcome of the 26 radiation-exposed patients and their matched controls
Thirty-day mortality was 8% (two patients) in both groups. In the radiation group, one patient died during the procedure due to annular rupture after post-dilatation on a bicuspid valve and one died the day following TAVI because of iliac rupture and severe bleeding. Heart failure and cardiogenic shock were the causes of the two deaths in the control group.
In each group, four patients experienced vascular complications treated using surgery or percutaneous treatment. In the radiation group, six patients (23%) suffered from congestive heart failure with haemodynamic complications versus three (12%) in the control group (p=0.001). This difference was not explained by arrhythmias or conduction disorders since less patients from the radiation group suffered from these problems (table 2).
Long-term outcomes
Survival
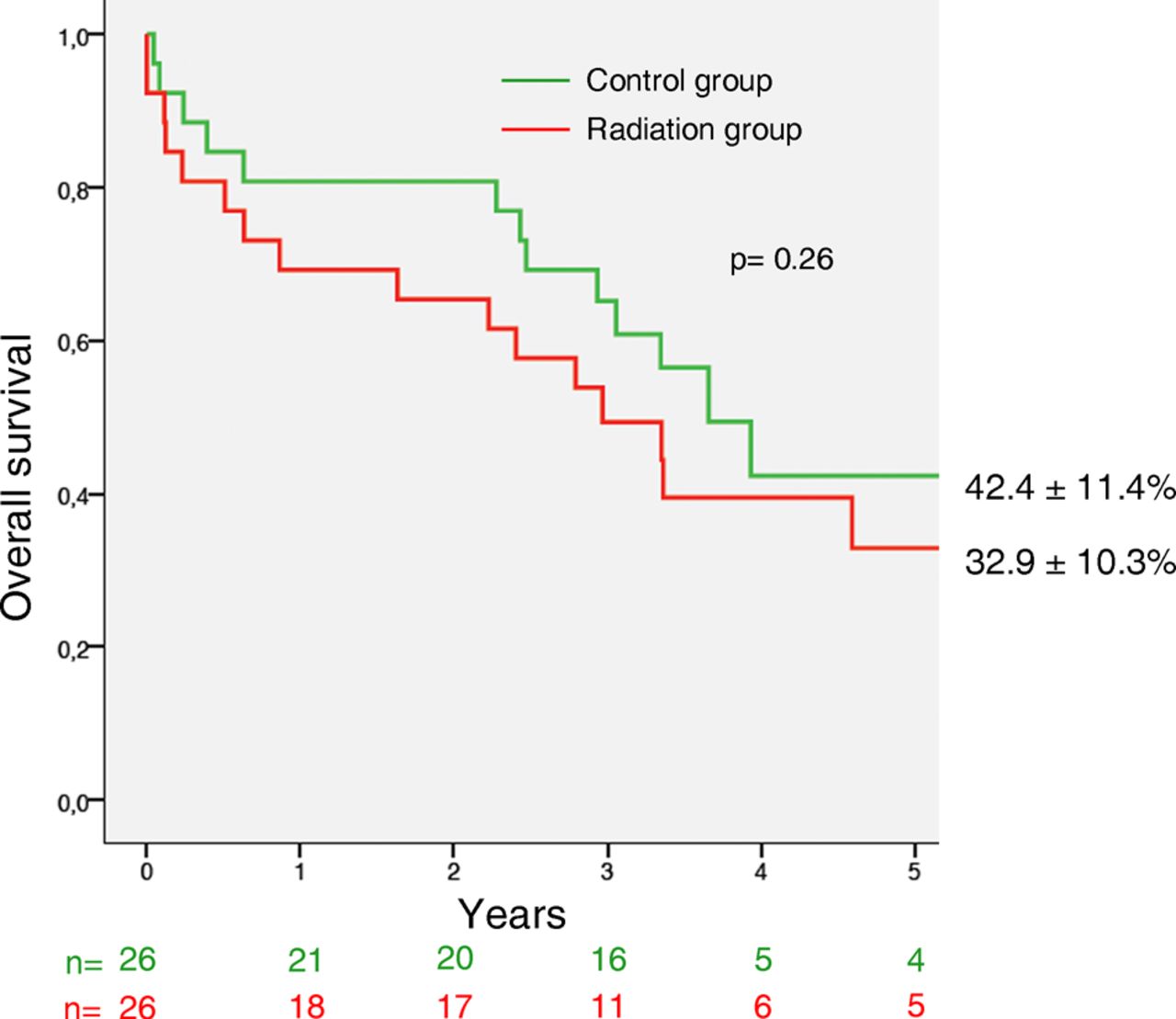
Follow-up was complete in all patients. In addition to the patients who died within the first 30 days, 15 patients died in the radiation group during a median follow-up of 3.0 (1.6–4.4) years and 11 in the control group during a median follow-up of 3.7 (2.8–4.6) years. The 5-year survival rates were 32.9%±10.3% and 42.4%±11.4% in the radiation and control groups, respectively (p=0.26) (figure 2).

Overall survival at 5-year follow-up after trans-catheter aortic valve implantation (TAVI) in the 26 patients with previous thoracic irradiation compared to age-matched, sex-matched and TAVI approach-matched controls.
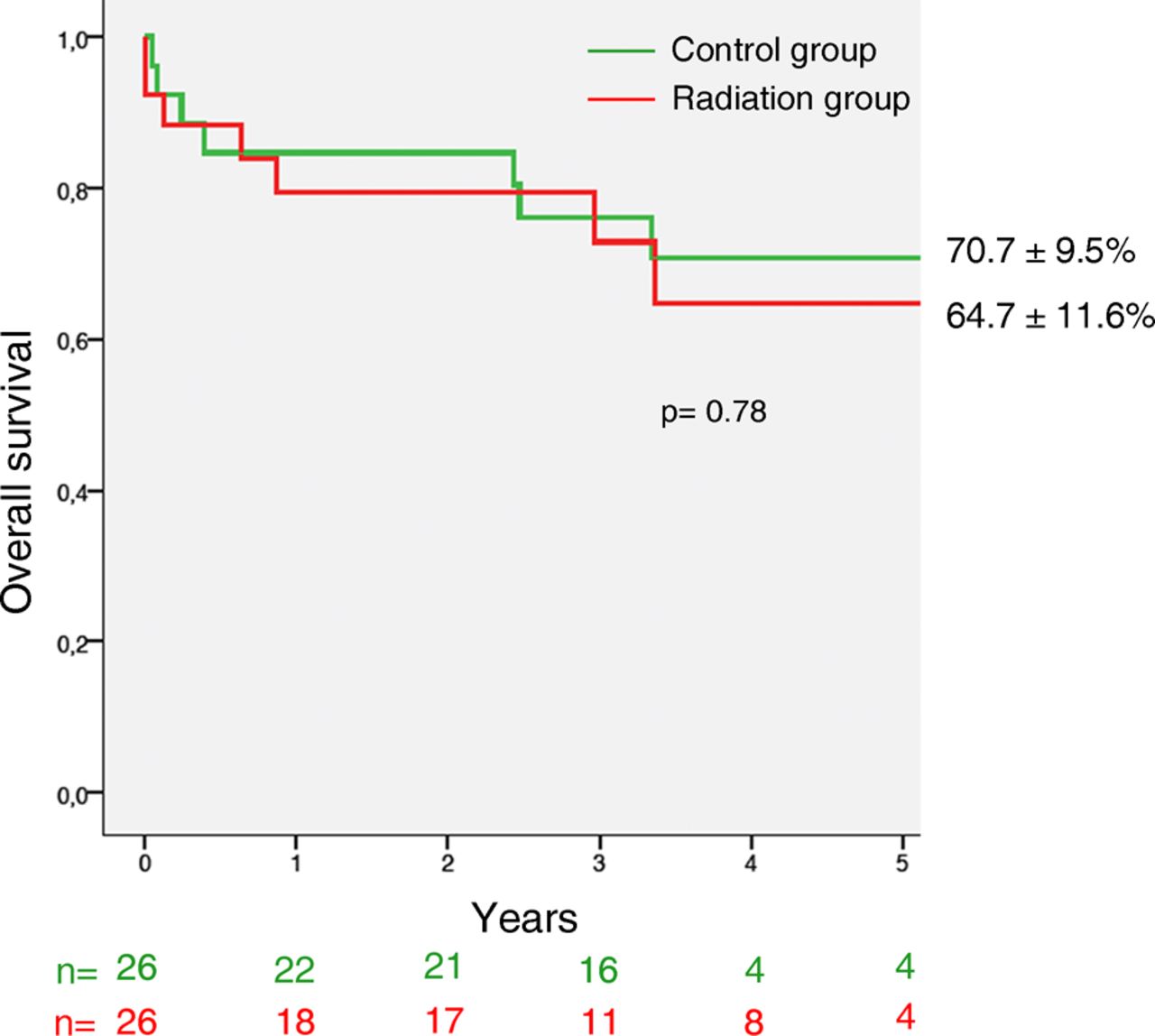
In the radiation group, only five patients (33.3%) died from cardiac cause after hospital discharge: acute pulmonary oedema in two, chronic left heart failure in one, sudden death in one and ventricular arrhythmias in one. The majority of deaths (66.7% of cases) were thus non-cardiac. The main cause of death in this population was respiratory failure secondary to radiation-induced fibrosis or sepsis in six patients (40%), non-pulmonary sepsis in two patients (13%), poor general condition with dementia in one and only one death due to relapse of neoplasm. This is illustrated by a survival rate without cardiovascular death of 64.7%±11.6% at 5 years (figure 3).

Cardiovascular survival at 5-year follow-up after trans-catheter aortic valve implantation (TAVI) in the 26 patients with previous thoracic irradiation (radiation group) compared to age-matched, sex-matched and TAVI approach-matched controls (control group).
In the control group, the majority of deaths were also non-cardiac in 7 out of 11 patients (64%) but only 1 patient died from respiratory failure. The other causes of death were metastatic cancer in two patients, sepsis in one, haemorrhage in one, renal insufficiency in one and following hip fracture in one. This is illustrated by a survival rate without cardiovascular death of 70.7%±9.5% at 5 years (figure 3). Survival rates without cardiovascular death were not different between radiation and control groups (p=0.78).
Predictive factors of mortality
Predictive factors of death for the radiation group are presented in table 3.
Predictive factors of overall survival in patients from the radiation group (univariate and multivariate analysis)
In multivariate analysis, we identified four predictive factors, two preprocedural variables: the presence of extracardiac arteriopathy (adjusted HR 43.21, 95% CI 3.79 to 492.97; p=0.002) and the absence of β-blocker therapy (adjusted HR 7.80, 95% CI 1.84 to 33.0; p=0.005), and two postprocedural variables: infectious complications (adjusted HR 8.93, 95% CI 1.74 to 45.77; p=0.009) and a higher peak creatinine level (adjusted HR 1.02, 95% CI 1.01 to 1.04 per µmol/L.; p=0.009).
Functional status
Among the nine survivors of the radiation group, eight patients (89%) were in NYHA class I or II at last follow-up. The improvement in NYHA class before and after the TAVI procedure among the survivors is illustrated in figure 4A.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
New York Heart Association (NYHA) class before and after the trans-catheter aortic valve implantation procedure among the survivors of the radiation group (A) and controls (B).
According to the EQoL-5D questionnaire, 44% of patients could walk easily, 78% had no problem with self-care, 78% had no difficulties in performing their usual activities, 56% were pain free and 67% were neither anxious nor depressed. According to the visual analogical scale of QoL, with the best imaginable state being 100 and the worst state being 0, the median score was 70 (53–78).
Only 54% of the 13 survivors in the control group were in NYHA class I or II at last follow-up (figure 4B). The EQ-5D questionnaire and the visual analogical scale of QoL could be assessed in 12 patients (92%) since 1 patient had advanced Alzheimer's disease. According to the questionnaire, 17% of patients could walk easily, 75% had no problem with self-care and 58% had no difficulties in performing their usual activities, were pain free and were neither anxious nor depressed. The median score of the visual analogical scale of QoL was 60 (43–70) in the control group (see online supplementary figure S1).
Supplementary figure
Discussion
Patients with previous chest radiation undergoing TAVI displayed a 5-year survival of 33%, not significantly different from the matched TAVI control population. In the radiation group, respiratory failure was the main cause of death and predictive factors of mortality were extracardiac arteriopathy, infectious complications and creatinine levels after TAVI, whereas β-blocker therapy before TAVI was a protective factor. Finally, despite high mortality rates at long-term follow-up after TAVI, the survivors experienced a substantial improvement in functional results.
Population
Radiation-induced valve dysfunction usually appears after the second decade following chest irradiation, which is consistent with the time delay reported in this study.5 ,9 The two main causes of radiation therapy in the present series were Hodgkin's lymphoma and breast cancer, in which most common non-malignant cause of death are CVD.1 ,5 ,19 ,20 Moreover, Hodgkin's survivors have a 9.2-fold higher risk of valve intervention.21
The population of the radiation group was younger than the patients usually undergoing TAVI (73 vs >80 years).16 ,22 ,23 However, they were older than the patients undergoing surgical management, aged from 51 to 63 years in cohorts of patients with prior radiation therapy.7 ,8 The differences between populations make the comparison of results difficult. This is, to the best of our knowledge, the first described radiation therapy cohort with severe AS treated by TAVI.
Early outcomes
The procedural success was 88% in the radiation group compared with 100% in controls (p<0.001), but this difference did not impact the 30-day mortality rate, which was comparable in both groups (8%) and consistent with previous studies on TAVI.16 ,22–24 Therefore, the presence of chest radiation did not seem to impact short-term mortality in TAVI, which differs from surgical series.7 Similarly, we did not observe more frequent atrial fibrillation or pacemaker implantation in the radiation group than in controls, in contrast with surgical management.7 The main in-hospital complication encountered in radiation patients was postprocedural congestive heart failure (23% vs 12% in controls, p=0.001). This is consistent with diastolic dysfunction, which is sevenfold more common in radiation patients compared with control subjects.5 ,8 ,25 This may be a reason for the trend to longer hospital stay in the radiation group compared with controls (16±20 days and 11±6 days, respectively, p=0.32), which is consistent with the findings after surgical management.7
Long-term survival
Radiation group 5-year survival was 33%, non-significantly different from the control group (42%, p=0.26), although probably underpowered because of the small number of patients. This 5-year rate was consistent with the results published so far in the general TAVI population (35–37%).24 ,25 However, as previously stated, our radiation patients were 10 years younger than usual TAVI patients, and these results thus emphasise the high risk of this particular population.
The main cause of death was respiratory failure, either chronic due to radiation-induced lung fibrosis or acute due to pulmonary infection. The importance of pulmonary condition has been well established for radiation patients undergoing open heart valve surgery, who showed a longer length of artificial ventilation, and a higher rate of tracheostomy or ventilation-induced pulmonary infections.7–9 In the setting of TAVI, pulmonary failure has also been reported as a major cause of non-cardiac death, accounting for about one quarter of deaths.22 ,26 In our population of radiation patients, 50% had respiratory insufficiency and pulmonary failure accounted for up to 40% of death causes. Radiation patients are exposed to the risk of pulmonary fibrosis and consequent restrictive respiratory insufficiency.27 We could not assess the impact of baseline respiratory function on outcome since only 58% of patients in the radiation group had pulmonary functional tests before TAVI. The burden of respiratory complications in late mortality highlights the need for a careful pre-TAVI assessment of respiratory function in patients with prior radiation therapy.
Predictive factors of mortality
The presence of extracardiac arteriopathy is consistent with previous findings in a general TAVI population.16 However, besides the negative impact of diffuse atherosclerosis, this factor may also reflect the importance of radiation-induced arteritis.28 It should be given particular attention during patient evaluation.
One of the key findings is the association between pre-TAVI β-blocker treatment and improved long-term survival. In a cohort of radiation patients undergoing valvular surgery, β-blocker therapy was also independently associated with decreased late mortality (HR 0.66 (0.47–0.93)).7 These results raise the question of whether β-blockers might be intrinsically protective before a TAVI procedure or if their absence could reflect a worse clinical condition, such as diastolic dysfunction. It is indeed noteworthy that a proportion of radiation patients cannot tolerate β-blockers, probably due to impaired myocardial compliance. Thus, the presence of β-blocker treatment might also be a marker of less altered myocardial damage after radiation exposure. Given consistent findings in surgically treated patients and our cohort on TAVI patients, it would be useful to evaluate prospectively the impact of β-blocker introduction before intervention.
Consistently with previous studies, one of the main causes of death in our radiation group was infectious complications, particularly pulmonary infections.8 Pneumococcal vaccine has been recommended by the Center for Disease Control for patients with generalised malignancy and/or iatrogenic immunosuppression including radiation therapy.29 Given the susceptibility of these patients to infections and the impact on late mortality, it is advised to check that their pneumococcal vaccine is efficient before TAVI. Radiation patients should be given particular attention regarding any signs of infection (biological testing) since they have an immunocompromised status with a possible debilitated clinical presentation.
The last predictive factor was a higher creatinine level after TAVI. Renal impairment is a frequent comorbidity and has been reported as a predictive factor of mortality both in TAVI and aortic valve surgery.30 Moreover, it may reflect haemodynamic status and a close monitoring seems mandatory in this radiation population given the high proportion of postprocedural heart failure and the impact of renal failure on late results.
Functional status
We found in this study a good functional status of radiation patients at last follow-up. We could have hypothesised that radiation patients’ quality of life would be less satisfactory than in controls given the numerous deleterious effects of radiation therapy. However, both the NYHA class assessment and the QoL questionnaire showed excellent sustained results in radiation patients, with a trend to be better than in control patients (89% of radiation patients in NYHA class I or II vs 54% in controls). These results are thus encouraging in this population, although they have to be interpreted with caution given the small sample size.
Study limitations
First, we report our early TAVI experience (from 2006) with first-generation catheters, which may negatively influence the results. Second, because of the single-centre nature of this study conducted in a large TAVI centre, referral bias cannot be excluded. Finally, the small number of patients precludes the observation of a significant statistical difference between the radiation group and controls and leads to consider the results of the multivariate analysis with caution since the number of events may lead to overfitting. However, to our knowledge, this is to date the only study reporting early and late outcome after TAVI in patients with previous chest radiation.
Conclusion
Patients with previous chest radiation display high mortality rates after TAVI although not significantly different from the control population. In patients with radiation valvular disease, the use of β-blockers is an independent predictor of late survival after TAVI, which deserves further consideration. The fact that respiratory failure is the main cause of death in this particular population emphasises the need for a careful pulmonary evaluation. Finally, patients show a sustained improvement in functional results after TAVI.
Key messages
What is already known on this subject?
Patients with a history of chest wall radiation exhibit a worse survival after cardiac surgery compared with controls, which has led to favour trans-catheter aortic valve implantation (TAVI) in these patients. However, there are so far no specific data on the results of TAVI in this population.
What might this study add?
This study reports for the first time a 5-year survival rate of 33% in patients with prior radiation therapy, not significantly different from controls (42%, p=0.26). It also includes predictive factors of mortality and late functional results in this particular population.
How might this impact on clinical practice?
The main cause of death in radiation patients is respiratory failure, which highlights the importance of careful pulmonary evaluation and follow-up in these patients. We identified post-TAVI infection as a predictive factor of late mortality, which emphasises the need for a particular awareness to sepsis signs in this population.
References
Footnotes
Contributors CB designed the study, analysed and interpreted the data and drafted the manuscript. MA participated in the interpretation of the data and drafted the manuscript. AT and BA participated to data collection and revised the manuscript. BI and DH participated in the analysis and interpretation of the data and revised the manuscript. EB was in charge of echocardiographic data collection, analysis and interpretation, and revised the manuscript. PO performed and analysed cardiac CT scan examinations and revised the manuscript. MU, WG, M-PD, PN and AVn, revised the manuscript.
Competing interests DH is a proctor for Edwards Lifesciences and Medtronic. PN is a consultant for Medtronic and a proctor for Edwards Lifesciences. AV is on the advisory board for Medtronic and receives speaker's fees from Edwards Lifesciences. BI has received speaker's fees from Edwards Lifesciences. All other authors have no relationships relevant to the contents of this paper to disclose.
Patient consent Obtained.
Ethics approval The local ethics committee.
Provenance and peer review Not commissioned; externally peer reviewed.