Article Text

Abstract
Objective Plasma level of N-terminal–pro-brain natriuretic peptide (NT-proBNP) is a reliable prognostic factor in patients with heart failure (HF). However, it is unclear how differently the biomarker predicts adverse outcomes in HF with preserved EF (HFpEF) versus HF with reduced EF (HFrEF).
Methods From the Korean Heart Failure registry, a prospective multicentre cohort for consecutive patients who were hospitalised for acute HF syndrome, those with available NT-proBNP and LVEF measurements were extracted. Patients with LVEF ≥50% were categorised as the HFpEF group (N=528) and those with ≤40% as the HFrEF group (N=1142).
Results Patients with HFpEF had significantly lower NT-proBNP level than those with HFrEF (median 2723 vs 5644 ng/L, p<0.001). Event-free survival did not differ between the two groups either in terms of death from any cause (88.4% vs 86.9%; p=0.471) or the composite of death or HF readmission at 1 year (73.8% vs 70.6%; p=0.225). High levels of NT-proBNP were significantly associated with poor outcomes. However, the relationship was not different among the HFpEF and HFrEF groups (interaction p=0.956 for all-cause death; p=0.351 for the composite of all-cause death or HF hospitalisation).
Conclusions Plasma level of NT-proBNP is the most powerful prognostic factor in both HFpEF and HFrEF. Although patients with HFpEF have lower NT-proBNP levels, the prognosis of a patient with HFpEF expected from a given NT-proBNP level is similar with his/her counterpart with HFrEF.
Statistics from Altmetric.com
Introduction
Neurohumoral pathways play a crucial role in the development and progression of heart failure (HF).1 ,2 Plasma levels of N-terminal–pro-brain natriuretic peptide (NT-proBNP) or B-type natriuretic peptide (BNP) are well-known markers for neurohumoral activity in patients with HF and can be reliably used for the diagnosis and the risk stratification.3–6
Among patients with clinical syndrome of HF, approximately half have normal or near normal LVEF, known as HF with preserved EF (HFpEF).7 ,8 HFpEF is one of the major growing public health problems as its prevalence has been steadily increasing while its survival did not improve.7 ,8 Patients with HFpEF and HF with reduced EF (HFrEF) have a different degree of neurohumoral activity;9 ,10 nonetheless, the diagnostic and prognostic values of plasma BNP or NT-proBNP levels have been well established in both types of HF.11–14 Although patients with HFpEF and HFrEF show very similar survival,7 ,8 interestingly HFpEF have typically lower natriuretic peptide values than in patients with HFrEF,15 suggesting the prognostic value of the natriuretic peptide may be dependent on the type of HF.
In this study, we sought to evaluate how differently NT-proBNP predicts adverse outcomes in patients with acute HF according to the types of HF.
Methods
Patients
The Korean Heart Failure (KorHF) registry is a prospective multicentre cohort study designed to reflect ‘real world’ clinical data of Korean patients admitted for acute HF. The design and primary results of the registry have been described elsewhere.16 Between June 2004 and April 2009, the data on the clinical status and in-hospital outcomes of consecutive patients who were hospitalised with an episode of acute HF were prospectively collected from 24 well-qualified tertiary hospitals in Korea. Acute HF was defined as new-onset (de novo) HF without a prior history or the acute worsening decompensation of chronic HF with a previous diagnosis. HF was diagnosed at admission according to the Framingham criteria,17 which was confirmed at the time of the patient's discharge. We obtained information on patient survival and hospital readmission for HF by medical records review and/or telephone contact, and all patients were recommended to be followed up for at least 1 year. Data were collected at each site by a trained study coordinator using a standardised case report form and entered into the KorHF registry database via a Web-based electronic data capture system. Data collection and audition were performed by the KorHF Registry Steering Committee at the Korean Society of Heart Failure.
Study variables and definitions
Patients with HF were categorised into the HFpEF (LVEF≥50%) or HFrEF (LVEF≤40%) groups.18 ,19 Variables including demographic and baseline characteristics, medical history, clinical presentation, laboratory tests, hospital course and clinical outcomes during admission and at discharge were obtained. Plasma NT-proBNP levels were measured at admission for the acute HF. The initial echocardiographic measurements performed during the index admission were collected. Blood sampling and tests were conducted as routine practice by laboratories at each centre certified by the Korean Association of Quality Assurance for Clinical Laboratories. Measurement of NT-proBNP was performed with the electro-chemiluminescence immunoassay method using an Elecsys 2010 analyser (Roche Diagnostics) or NT-proBNP assay for Dimension platform, Siemens Medical Solutions Diagnostics. The primary endpoint of this study was all-cause death at 12 months. The secondary endpoint was defined as a composite of all-cause death or HF readmission at 12 months after the index hospitalisation.
Statistical analysis
Data were presented as frequencies or mean±SD. Restricted cubic splines were used to allow for non-linearity in the relationship between continuous NT-proBNP level and relative hazards with the use of the ‘Hmisc’ packages in R program. Linear and quadratic Cox regression models were constructed, and the nested models were compared using the likelihood ratio test. Interactions of the type of HF with continuous NT-proBNP level were illustrated by plotting the log relative hazards and compared with the use of the likelihood ratio test. Proportionality of hazards of the Cox models were tested using the Schoenfeld residuals (see online supplementary figures S2–S5). The Kaplan–Meier curves were plotted and compared with the log-rank test.
For multivariable analysis, missing values were imputed by multiple imputation method using the ‘mi’ packages in R program. Variables used for the multiple imputation model included age, gender, body mass index, diabetes, hypertension, chronic kidney disease, previous myocardial infarction, peripheral artery disease, valvular heart disease, previous history of stroke, chronic lung disease, smoking status, atrial fibrillation, systolic and diastolic blood pressure, heart rate, serum sodium, haemoglobin and New York Heart Association (NYHA) class. The proportion of missing values was <5% in 13 out of 19 variables, and 5–10% in the rest 6 variables. We assumed that missing data were missing at random, such that the observed data can be used to explain the missing data. We generated and combined multiple (n=5) imputed datasets that included within-imputation and between-imputation error estimates. Time-dependent receiver operating characteristic (ROC) curves were constructed and areas under the curves were compared using the ‘timeROC’ packages in R program. Statistical analyses were performed using R programming V.3.1.0 (The R Foundation for Statistical Computing, Vienna, Austria, http://www.R-project.org). A two-sided p value<0.05 was considered significant.
Results
Patient characteristics
Among a total of 3200 patients registered in the KorHF registry, plasma NT-proBNP level was available in 2169 (67.8%) and LVEF in 2843 (88.8%) patients (demographics compared in online supplementary table S1). After excluding HF with borderline EF (LVEF 41–49%), 1670 patients were included in this study: 528 (31.6%) with HFpEF and 1142 (68.4%) with HFrEF. The median age of study population was 70 years, and 48.9% of patients were male. Consistent with previous reports, patients with HFpEF were older, had higher body mass index and were more frequently associated with female sex, hypertension and atrial fibrillation, but less frequently associated with ischaemic aetiology.
Plasma level of NT-proBNP ranged from 8 to >35 000 ng/L with a median of 4508 ng/L. Patients with HFpEF had significantly lower NT-proBNP level than those with HFrEF (median 2723 vs 5644 ng/L, p<0.001) (figure 1). Table 1 shows patient characteristics according to the quartiles of NT-proBNP levels stratified by the type of HF. Patients with higher NT-proBNP level were more likely to be older and female, and more likely to have comorbidities including hypertension, diabetes and chronic kidney disease. In addition, these patients had more advanced NYHA class and higher blood pressure, heart rate and serum creatinine, but lower level of serum sodium and haemoglobin.
Patient characteristics according to NT-proBNP

Violin plots showing the distribution of N-terminal–pro-brain natriuretic peptide (NT-proBNP) levels in heart failure with preserved and reduced EF. The density trace of violin plots shows the distribution of NT-proBNP levels, while the box plots inside represent the summary statistics. The box plot shows the median (diamond in centre), the first through the third IQRs (thick, solid, vertical band), and notches (thin, vertical line) of NT-proBNP levels. The Y-axis represents log10-transformed plasma NT-proBNP levels. HFpEF, heart failure with preserved EF; HFrEF, heart failure with reduced EF.
Clinical outcomes
One-year follow-up was complete in 1237 among 1670 subjects (74.2%). Event rates did not differ between the HFpEF and HFrEF groups either in terms of death from any cause (11.6% vs 13.1%; HR with 95% CIs 0.90 (0.67 to 1.21); p=0.471) or the composite of death or HF readmission at 1 year (26.2% vs 29.4%; HR 0.89 (95% CI 0.73 to 1.08); p=0.225) (see online supplementary figure S1). Figure 2 shows the relationship between the rates of adverse clinical events and the plasma NT-proBNP level at admission. The risk of all-cause death increased linearly with increasing level of log10-transformed NT-proBNP, which had no significant interaction with the type of HF, that is, HFpEF vs HFrEF (interaction p=0.878 for linear model). In other words, a 10-fold increase in NT-proBNP was associated with three times higher risk for mortality in both HFpEF and HFrEF. The occurrence of the secondary endpoint, the composite of death or HF readmission, in relation with log10-transformed NT-proBNP level was best explained by a quadratic model; the event rate was lowest at 1000 ng/L of NT-proBNP and rose up with either lower or higher levels. The relationship of NT-proBNP level with the secondary endpoint did not significantly differ between the HFpEF and HFrEF groups (interaction p=0.680 for quadratic model; 0.712 for linear model). Kaplan–Meier survival curves according to the quartiles of plasma NT-proBNP are shown in figure 3. In the HFpEF group, while patients in the first to third NT-proBNP quartiles had similar outcomes, only patients in the highest quartile had higher 1-year mortality (23.8% vs 14.9% vs 8.1% vs 7.7%; p<0.001). In contrary, in the HFrEF group, patients in the first quartile had the lowest (4.6%), whereas those in the fourth quartile the highest 12-month mortality (21.3%).

N-terminal–pro-brain natriuretic peptide (NT-proBNP) levels and (A) death from any cause or (B) the composite of death or heart failure (HF) readmission in HF with preserved versus reduced EF (HFpEF). The X-axis represents log10-transformed plasma NT-proBNP levels, while the Y-axis event rates. Interaction p values are based on log10-transformed NT-proBNP levels. Bold lines represent expected event rates, and dotted lines 95% confidence limits. HFrEF, HF with reduced EF.
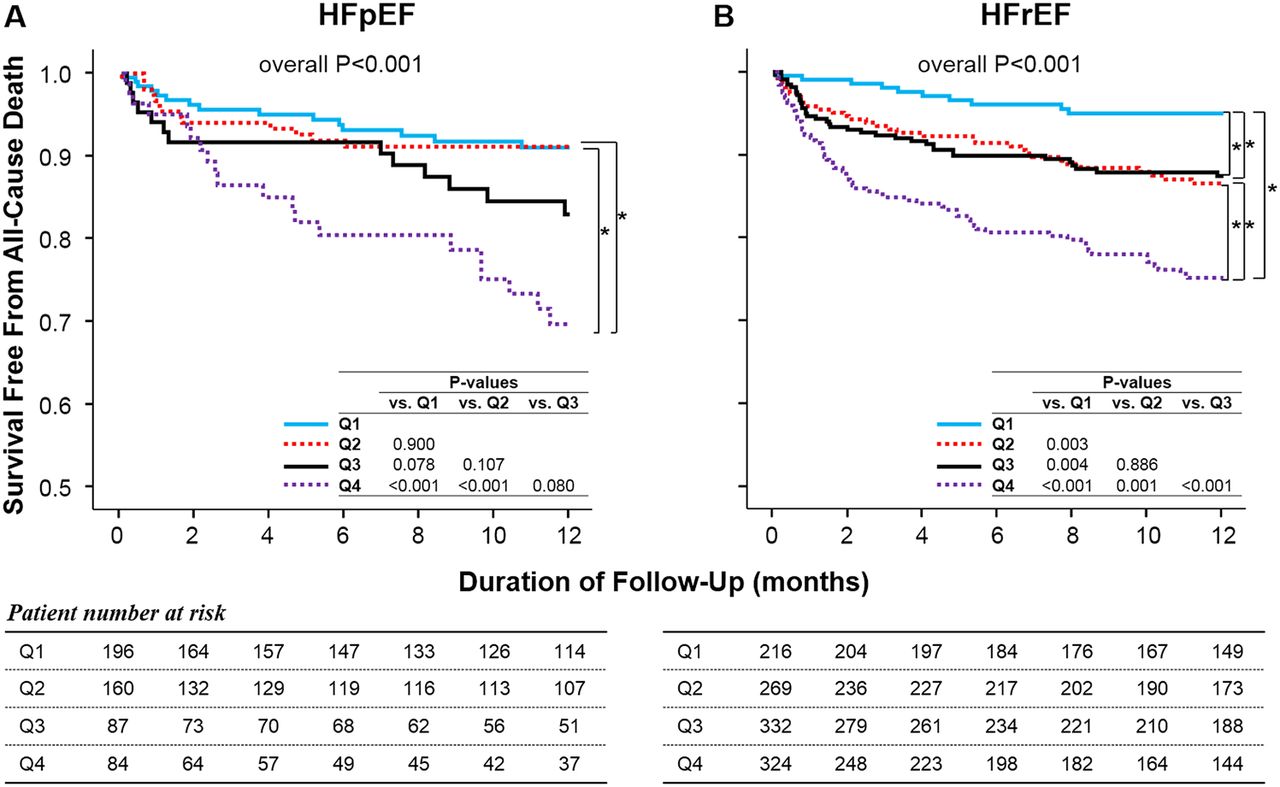
Kaplan–Meier survival curves free from all-cause death in patients with (A) heart failure with preserved EF (HFpEF) and in patients with (B) heart failure with reduced EF (HFrEF). p Values are described for each pairwise comparison.
Multivariable and subgroup analyses
The Cox regression model with a forward selection method using Wald statistic was used to find the independent predictors for all-cause death (table 2). Plasma level of NT-proBNP among baseline factors was the most powerful predictor for the primary endpoint regardless of HF types. After adjustment for major risk factors, every 1000 ng/L increment in NT-proBNP was shown to be associated with a 3–5% increase in the risk of mortality.
Independent predictors for death from any cause at 1 year
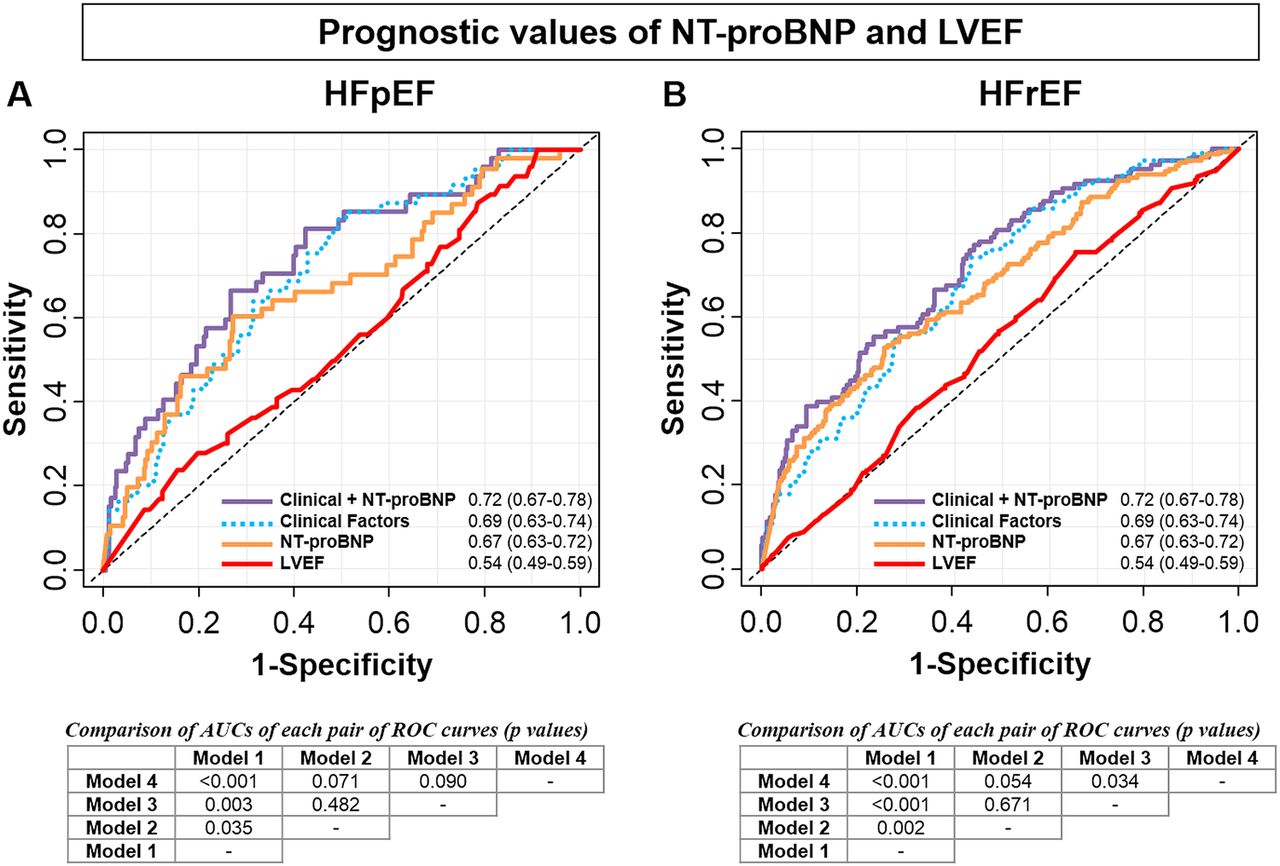
Of note, the prognostic value of LVEF was not statistically significant in this study population. Figure 4 shows the time-dependent ROC curves analysis for LVEF, NT-proBNP and other clinical factors. A combination of NT-proBNP and clinical factors had the highest area under the curve in both HFpEF and HFrEF groups, while the model with LVEF alone did not predict adverse outcomes with statistical significance. The primary and secondary endpoints stratified by NT-proBNP quartiles and LVEF are depicted in online supplementary figure S6, which shows LVEF provides no additional prognostic information over NT-proBNP. We could not find any significant interactions in subgroup analyses according to patients’ age, sex, serum sodium levels, creatinine levels or functional class.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Receiver operating characteristic curve analysis for death from any cause for (A) the heart failure with preserved EF (HFpEF) group and (B) the heart failure with reduced EF (HFrEF) group. Four models were constructed and compared: (1) model 1 with LVEF; (2) model 2 with the plasma levels of N-terminal–pro-brain natriuretic peptide (NT-proBNP); (3) model 3 with clinical factors including age, serum sodium, diastolic blood pressure, obesity and previous myocardial infarction; and (4) model 4 with clinical factors combined with NT-proBNP levels. AUC, area under the curve; ROC, receiver operating characteristic.
Discussion
In this study, we showed that plasma level of NT-proBNP was a powerful prognostic factor in both HFpEF and HFrEF groups. We also showed that patients with HFpEF had lower NT-proBNP levels than those with HFrEF and the overall mortality rate did not differ between the groups. Interestingly, we could not observe a significant interaction between the NT-proBNP level and the HF type. However, NT-proBNP was able to identify a low-risk group only in patients with HFrEF with the lowest NT-proBNP quartile. LVEF had no significant impact on mortality in this study population.
HFpEF, defined as symptomatic HF with normal to near normal LVEF, accounts for about one-half of patients hospitalised due to acute HF.7 ,8 ,20 The pathophysiology includes LV diastolic dysfunction as well as multiple non-diastolic abnormalities such as systolic dysfunction, ventricular–arterial coupling, vascular dysfunction, chronotropic incompetence and impaired cardiovascular reserve.21 ,22 Anatomically, patients with HFpEF have a concentric remodelling with increased relative wall thickness and relatively preserved LV diameter, resulting in a high ratio of mass to volume, whereas patients with HFrEF have an enlarged LV cavity, but relatively normal LV wall thickness.23 According to the law of Laplace, the wall tension correlates directly with wall pressure and LV diameter, but inversely with LV wall thickness. BNP is a cardiac neurohormone that is mainly secreted from the ventricles in response to an increase in wall tension.1 Recently, Maeder and colleagues showed that the release of BNP from myocardium was determined largely by end-systolic wall stress, and that the effects of diastolic load were only weak.24 Patients with HFpEF who have lower wall tension thus have lower natriuretic peptide levels than those with HFrEF.9
This study was provoked by the finding that patients with HFpEF and HFrEF have similar prognosis,7 ,8 ,20 while patients with HFrEF have a twofold higher NT-proBNP level than those with HFpEF. Thus, it was hypothesised that the plasma NT-proBNP levels may have a differential prognostic function dependent on the type of HF. Contrary to the expectation, we found in this study that for a given NT-proBNP level the expected mortality rate is similar in patients with HFpEF and HFrEF.
However, we found a difference in risk stratification pattern especially in patients with low NT-proBNP levels. In general, patients with low BNP level usually have better prognosis and those with high BNP level have worse prognosis. In this study, the Kaplan–Meier survival curves (figure 3) display that NT-proBNP quartiles show different patterns of discrimination between HFpEF and HFrEF; whereas in the HFrEF group the lowest quartile had significantly lower event rates than the second and third quartiles, in the HFpEF group the first three quartiles had similar event rates. Consequently, low NT-proBNP level identifies a low-risk group only among the patients with HFrEF, not among the patients with HFpEF, whereas high NT-proBNP level is associated with worse outcomes in both types of HF.
Finally, we found that NT-proBNP was the strongest prognostic factor, while LVEF had little value in predicting adverse events. In previous studies, BNP or NT-proBNP levels have been shown to be an important prognostic factor in both HFpEF12–14 or HFrEF.5 ,6 The independent predictors in our multivariable analysis were in line with previous studies. It also holds true for the lack of significant association between LVEF and clinical outcomes.25 ,26 Recently, van Veldhuisen and colleagues performed a study with 615 patients with mild to moderate HF to show that BNP was a strong predictor of outcome, but that LVEF was not.27 With subjects of different ethnicity and much larger sample size, we confirmed that LVEF has only limited prognostic value. What this study adds to the current knowledge is that NT-proBNP can be regarded as the most powerful predictor for the prognosis of a patient with HF irrespective of his/her LV systolic function.
This study provides important insight into the treatment of patients with HFpEF. Studies have shown patients with HFrEF benefit from natriuretic peptide-guided treatment.28 However, data on the biomarker-guided strategy in HFpEF are scarce until now. The only randomised trial, which enrolled elderly patients (≥60 years), showed no beneficial effects of natriuretic peptide-guided therapy in patients with HFpEF. In fact, there was a tendency towards potential harm in association with natriuretic peptide-guided therapy.29 However, the study was limited by the small sample size. It was powered only for the HFrEF arm, and the patient number of the HFpEF arm was even less than expected. In addition, although natriuretic peptides have a prognostic value in older patients with HFrEF, natriuretic peptide-guided management has not been shown helpful in these patients. Future studies are needed to investigate the role of NT-proBNP in the treatment of patients with HFpEF.
Study limitations
First, since we applied the Framingham criteria for diagnosis of HF, we cannot exclude that patients without HF may be included in this study, although all patients underwent either echocardiography or natriuretic peptide measurement. Furthermore, the diagnosis of HFpEF is sometimes not straightforward, and there are chances that patients with dyspnoea that is not in fact due to cardiac origin are falsely diagnosed to have HFpEF. However, the risk of bias is commonly present in HFpEF studies, and the characteristics of this study population are similar to those of others. Second is sampling bias. In this study, patients with measurements of both LVEF and NT-proBNP were analysed, who accounted for 61% of the total cohort. As shown in online supplementary table S1, there were significant differences between patients with and without NT-proBNP measurements. Third, the definition of HFpEF varies across studies. However, the definition of LVEF≥50% and 40% for HFpEF and HFrEF, respectively, is generally recommended by current guidelines.18 ,19 Fourth, the assumption of proportional hazards was not handled during the stepwise Cox regression, although it was tested for the final Cox models.
Conclusions
Plasma level of NT-proBNP is a powerful prognostic factor in both HFpEF and HFrEF. Although patients with HFpEF have lower NT-proBNP levels, the prognosis of a patient with HFpEF expected from a given NT-proBNP level is similar to his/her counterpart with HFrEF. This study implies NT-proBNP may be useful in risk-stratifying patients with HF irrespective of the types of HF.
Key messages
What is already known on this subject?
Patients with heart failure with preserved EF (HFpEF) and heart failure with reduced EF (HFrEF) show very similar prognosis. However, natriuretic peptide values are significantly higher in HFrEF than in HFpEF.
What might this study add?
Higher levels of N-terminal–pro-brain natriuretic peptide (NT-proBNP) were significantly associated with worse outcomes. The relationship between increasing NT-proBNP levels and prognosis did not differ between the HFpEF and HFrEF groups.
How might this impact on clinical practice?
NT-proBNP level can be used for risk stratification in both HFpEF and HFrEF.
Acknowledgments
The KorHF Registry was conducted from 24 medical centres: Catholic University Seoul St. Mary's Hospital, Chungnam National University Hospital, Chungbuk National University Hospital, Chonnam National University Hospital, Ewha Woman's University Hospital, Eulji University Daejeon Hospital, Gacheon University Gil Hospital, Hallym University Sacred Heart Hospital, Hanyang University Guri Hospital, Jeju National University Hospital, Konkuk University Medical Centre, Keimyung University Hospital, Korea University Guro Hospital, Kyungpook National University Hospital, Sungkyunkwan University Samsung Medical Centre, Seoul National University Bundang Hospital, Seoul National University Hospital, Ulsan University Asan Medical Centre, Wonkwang University Hospital, Yonsei University Wonju Christian Hospital, Yeungnam University Hospital, Yonsei University Severance Hospital, Dongguk University Ilsan Hospital, Soonchunhyang University Cheonan Hospital and Inje University Busan Paik Hospital.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online supplement
Footnotes
Contributors S-HK and JJP contributed equally to this article. All authors fulfil the authorship requirements and have approved of the final version of the manuscript. Study hypothesis and design was developed by S-HK, JJP and D-JC. Data preparation was conducted by S-HK, C-HY and I-YO, and analyses by S-HK and JJP. S-HK wrote the first draft of the manuscript to which all authors made significant and subsequent intellectual contributions.
Funding This work was supported by a grant from the Korean Society of Heart Failure, and the Korean Society of Cardiology and by Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Education, Science and Technology (2012M3A9C7050140 and 2012R1A2A2A02012821).
Competing interests None declared.
Patient consent Obtained.
Ethics approval The institutional review board or ethics committee at each participating hospital approved the study protocol.
Provenance and peer review Not commissioned; externally peer reviewed.