Article Text

Abstract
Objective In heart failure populations without aortic stenosis (AS), the prognostic utility of multiple biomarkers in addition to clinical factors has been demonstrated. We aimed to determine whether multiple biomarkers of cardiovascular stress are associated with mortality in patients with AS undergoing aortic valve replacement (AVR) independent of clinical factors.
Methods From a prospective registry of patients with AS, 345 participants who were referred for and treated with AVR (transcatheter (n=183) or surgical (n=162)) were included. Eight biomarkers were measured on blood samples obtained prior to AVR: growth differentiation factor 15 (GDF15), soluble ST2 (sST2), amino-terminal pro-B-type natriuretic peptide (NTproBNP), galectin-3, high-sensitivity cardiac troponin T, myeloperoxidase, high-sensitivity C reactive protein and monocyte chemotactic protein-1. Biomarkers were evaluated based on median value (high vs low) in a Cox proportional hazards model for all-cause mortality and a parsimonious group of biomarkers selected. Mean follow-up was 1.9±1.2 years; 91 patients died.
Results Three biomarkers (GDF15, sST2 and NTproBNP) were retained in the model. One-year mortality was 5%, 12%, 18% and 33% for patients with 0 (n=79), 1 (n=96), 2 (n=87) and 3 (n=83) biomarkers elevated, respectively (p<0.001). After adjustment for the Society of Thoracic Surgeons (STS) risk score, a greater number of elevated biomarkers was associated with increased mortality (referent: 0 elevated): 1 elevated (HR 1.47, 95% CI 0.60 to 3.63, p=0.40), 2 elevated (HR 2.89, 95% CI 1.24 to 6.74, p=0.014) and 3 elevated (HR 4.59, 95% CI 1.97 to 10.71, p<0.001). Among patients at intermediate or high surgical risk (STS score ≥4), 1-year and 2-year mortality rates were 34% and 43% for patients with three biomarkers elevated versus 4% and 4% for patients with 0 biomarkers elevated. When added to the STS score, the number of biomarkers elevated provided a category-free net reclassification improvement of 64% at 1 year (p<0.001). The association between a greater number of elevated biomarkers and increased mortality after valve replacement was similar in the transcatheter and surgical AVR populations.
Conclusions These findings demonstrate the potential utility of multiple biomarkers to aid in risk stratification of patients with AS. Further studies are needed to evaluate their utility in clinical decision-making in specific AS populations.
Statistics from Altmetric.com
Introduction
With the increasing prevalence of calcific aortic stenosis (AS), decreasing operative mortality for aortic valve replacement (AVR) and the transformative innovation of transcatheter AVR (TAVR), risk stratification of patients with AS has become more challenging, complex and desirable.1 ,2 Biomarkers have not figured prominently in the risk stratification of patients with AS; most studies have examined the utility of natriuretic peptides, with some recent studies looking at high-sensitivity troponin and other assays.3 ,4 Improved risk stratification using biomarkers in patients with AS could aid clinical decisions about when, how and whether to perform valve replacement. In heart failure populations without AS, the prognostic utility of multiple biomarkers (evaluated in combination) in addition to clinical factors has been demonstrated; whether the same is true for patients with AS is unknown.5 To address this issue, we examined biomarkers of cardiovascular stress that have been shown to have prognostic utility in heart failure cohorts: growth differentiation factor 15 (GDF15) (fibrosis, inflammation), soluble ST2 (sST2) (myocyte stress), galectin-3 (Gal3) (fibrosis, inflammation), amino-terminal prohormone of B-type natriuretic peptide (NTproBNP) (neurohormonal activation), high-sensitivity cardiac troponin T (hs-cTnT) (myocyte injury), myeloperoxidase (MPO) (oxidative stress), high-sensitivity C reactive protein (hsCRP) (inflammation) and monocyte chemotactic protein-1 (MCP-1) (inflammation).6–9 We hypothesised that multiple biomarkers reflecting diverse biological pathways would improve risk stratification of patients with AS undergoing surgical AVR or TAVR in comparison to the Society of Thoracic Surgeons (STS) risk score, which is the existing standard.10
Methods
Study population and design
From an ongoing, prospective study of patients with AS in which clinical and echocardiographic data and biospecimens are collected, 345 participants recruited between August 2010 and April 2014 were included who were referred for and treated with AVR (transcatheter or surgical approach) at Barnes Jewish Hospital in St. Louis, Missouri. Patients seen in the cardiac surgery clinics or multidisciplinary high-risk valve clinic or those identified on the surgery schedule were potentially included. Patients had to be ≥18 years of age and have severe AS with an aortic valve area <1.0 cm2 or aortic valve area index ≤0.6 cm2/m2. Patients with prior valve replacement surgery, pulmonary fibrosis, cirrhosis, known active infection or cancer, or end-stage renal disease on dialysis were excluded.
Clinical variables were obtained through patient interview and chart abstraction. The STS risk score was calculated for each patient according to the STS definitions for each of the clinical characteristics using the publicly available website (V.2.73). Echocardiographic measurements were made as recommended by the European Society of Echocardiography and described previously and reflect an average of 3–5 values.11 ,12
Biomarker and LV tissue analyses
Venous blood was acquired in the clinic or hospital setting an average of 31 (14, first quartile; 57, third quartile) days prior to valve replacement, usually at a time when blood was drawn for clinical purposes. In a subset of patients (16%), blood was collected in the operating room 73±18 min after the patient was asleep. Blood samples were processed immediately and stored as aliquots of plasma or serum at −80°C until time of assay. GDF15, sST2, NTproBNP, MPO, Gal3, hs-cTnT, hsCRP and MCP-1 concentrations were measured from banked samples (1 freeze-thaw cycle). Assay details are provided in the online supplementary material. In a subgroup of patients, LV tissue was obtained from the basal septum of the heart at the time of surgical AVR. Detailed methods for the quantitative measurement of fibrosis and inflammatory cell number in the myocardium are provided in the online supplementary material.
Statistical analysis
Data are presented as frequencies, mean (SD) or median (25th, 75th percentiles). Determination of vital status was assessed by a combination of chart abstraction, in-person or telephone contact, and public record search (up to October 2014). A multivariable Cox proportional hazards model was built including all eight biomarkers; to make it more clinically meaningful, biomarkers were evaluated based on their median value (high vs low). A step-down variable selection technique was used to identify a parsimonious group of biomarkers; Akaike's information criteria was used to establish a stopping point.13 Biomarker levels, patient characteristics, medication usage and echocardiographic measurements were compared between groups determined by the elevated number of the selected biomarkers using analysis of variance and Fisher's exact test for continuous and categorical data, respectively. Non-normal and ordinal data were compared using the Kruskal–Wallis test. Each biomarker was evaluated using the median value as a cut-point for high versus low values and by log2 transformation standardised to a mean of 0 and SD of 1. The standardised log2 transformations were used to aid in comparison of individual biomarkers. The association between each biomarker and all-cause mortality was evaluated and described by the HR using Cox proportional hazards models. The HR of the standardised log2 transformation represents the increase/decrease in the likelihood of death for a 1 SD increase in the biomarker. In separate models, adjustment was made for (1) STS score and (2) clinical factors, including glomerular filtration rate, sex, diabetes mellitus, obstructive lung disease, New York Heart Association (NYHA) functional class (III/IV vs I/II) and aortic mean gradient. These six clinical factors were obtained from a Cox proportional hazards model for mortality that included 14 variables (age, body mass index, coronary disease, atrial arrhythmia, peripheral vascular disease, EF, mitral regurgitation severity and TAVR versus surgical aortic valve replacement (SAVR) in addition to the six variables already listed) and a backward selection method using p<0.20 set as the selection criteria.
Kaplan–Meier (KM) curves were created for groups of patients based on the number of the selected biomarkers that were elevated and the log-rank test used to evaluate the overall difference between the curves. KM estimates for 1-year and 2-year mortality were determined and reported based on the number of biomarkers elevated within different groups defined by the STS risk score (<4, 4–8 and >8). The probability of death at 1 year was derived from a Cox proportional hazards model having STS score and the number of elevated biomarkers as independent predictors and was used to visually examine the utility of evaluating biomarker elevations in addition to the STS score. Subgroup analyses were performed with separate models evaluating the interactions between the number of biomarkers elevated and several patient characteristics.
The integrated discrimination improvement (IDI) and the category-free net reclassification improvement (NRI) were determined to further describe the added utility of multiple biomarker measurements when added to the STS score.14 ,15 The IDI measures the new model's ability to improve integrated (average) sensitivity without sacrificing integrated (average) specificity.14 The NRI measures the correctness of patient reclassification based on the probability of death at selected time points.15 All analyses were conducted with SAS V.9.4 (SAS Institute, Cary, North Carolina, USA) except for the calculations of the survival-based c-statistic, IDI and NRI, which was conducted with the R software packages SurvC1 by Hajime Uno and Hmisc by Frank Harrell. A more complete list of references is found on the online supplementary material.
Results
Participants
Among the 345 patients included in the analysis, the average age was 78 years, 44% were women, mean aortic valve area was 0.74 cm2 and mean EF 58% (table 1). Most had heart failure symptoms: NYHA functional class was II in 19%, III in 56% and IV in 18%. Chest pain consistent with angina was present in 31% and syncope had occurred in 11%. The mean STS score was 7.5 (5.8); 107 (31%) had a lower risk STS score (<4), 112 (32%) had an intermediate risk STS score (4–8) and 126 (37%) had a high-risk STS score (>8). TAVR was performed in 183 patients (53%), including 77, 65 and 41 treated via transfemoral, transapical and transaortic approaches, respectively. Of the 162 patients treated with conventional surgery, 127 had isolated AVR and 35 underwent a concomitant procedure (29 coronary bypass, 4 MAZE, 2 ascending aorta repair). Among patients treated with TAVR, 86% (157/183) had coronary disease and 8% underwent a percutaneous coronary intervention between blood collection and the TAVR procedure. Baseline biomarker levels and clinical, medication and echocardiographic characteristics are shown for the whole population and according to the number of the selected biomarkers that were elevated (table 1).
Relationship Between Baseline Characteristics and the Number of Biomarkers Elevated
Individual biomarkers and mortality
All patients had each of the eight biomarkers measured in their banked plasma or serum. The correlations between each of the biomarkers are shown in online supplementary table S1. During a mean follow-up of 1.9 (1.2) years, 91 (26%) patients died, including 54 patients treated with TAVR and 37 patients treated with SAVR. The associations (unadjusted and adjusted) between each of the biomarkers and mortality are shown based on standardised log-transformed biomarker levels and median values (see online supplementary table S2). GDF15 had the strongest and most consistent relationship with mortality, followed by sST2 and NTproBNP.
Multiple biomarkers in combination
From among the eight biomarkers evaluated, a parsimonious group of biomarkers was identified that included GDF15, sST2 and NTproBNP (see online supplementary table S3). An elevation in each of these three biomarkers was treated equally. One-year mortality was 5%, 12%, 18% and 33% for patients with 0, 1, 2 and 3 biomarkers elevated, respectively. Increased mortality associated with an increased number of biomarkers elevated was observed in the whole population and the subgroups treated with TAVR and surgical AVR (p<0.001 for all) (figure 1A–C).

Multiple biomarkers and mortality after transcatheter or surgical aortic valve replacement. Kaplan–Meier curves are shown for number of biomarkers elevated (0, 1, 2 or 3) for patients treated with surgical (SAVR) or transcatheter aortic valve replacement (TAVR) (A), TAVR only (B) or SAVR only (C).
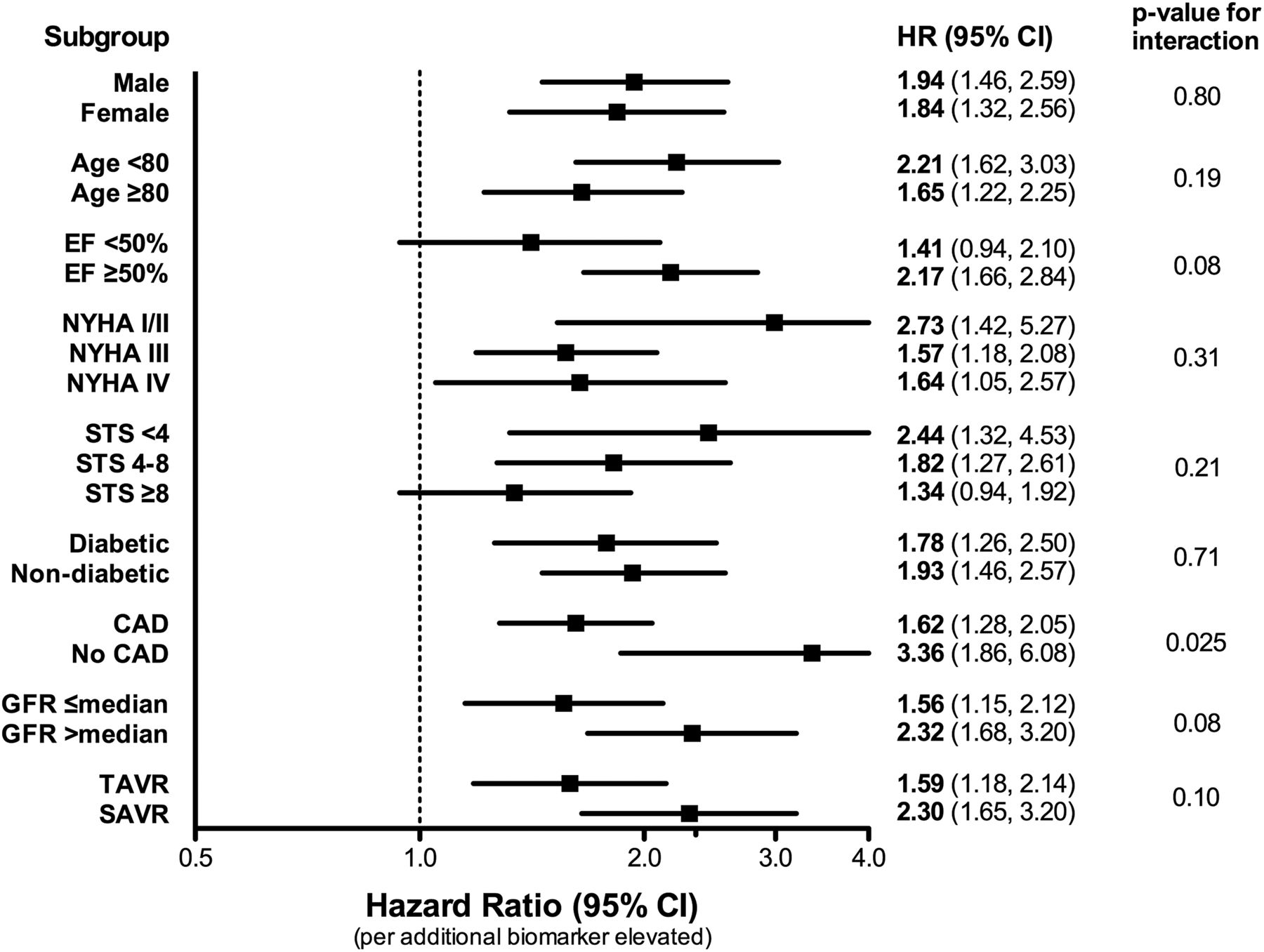
After adjustment for the STS score or other clinical factors, the increased hazard of death associated with each increased biomarker was 1.7 (p<0.001) (table 2). After the same adjustment and compared with patients with no biomarkers elevated, those with two biomarkers elevated had an almost threefold increased hazard of death and those with three biomarkers elevated had a greater than fourfold increased hazard of death (p<0.05 for all) (table 2). No increased hazard of death was found among patients having only one elevated biomarker. Across the spectrum of STS scores from low to high, mortality increased as the number of elevated biomarkers increased (figure 2). Among those at intermediate or high surgical risk with an STS score ≥4, those with three biomarkers elevated had 1-year and 2-year mortality rates of 34% and 43%, whereas those with no biomarkers elevated had 1-year and 2-year mortality rates of 4% and 4%. The relationship between an increased number of elevated biomarkers and increased mortality was consistent across subgroups, including the transcatheter and surgical AVR populations, albeit with an even stronger relationship among patients without coronary disease (figure 3).
Multivariable Models for Mortality

Society of Thoracic Surgeons (STS) score, biomarker elevations and mortality. Kaplan–Meier estimates for 1-year mortality are shown according to STS score and number of biomarkers elevated (0, 1, 2 or 3) for patients treated with surgical (surgical aortic valve replacement) or transcatheter aortic valve replacement separated by STS groups (<4, 4–8 and >8) (A) and combined into intermediate and high-risk patients with STS ≥4 (B). Based on a Cox proportional hazards model developed with STS score and the biomarkers, predicted 1-year estimates of mortality are shown for the spectrum of STS scores representing patients in our study according to the number of biomarkers elevated (C).
{kind=link}
{kind=link}
{kind=link}
Subgroup analyses for the biomarker elevations and mortality. The HR for mortality is shown for each additional biomarker elevated in various subgroups as well as the interaction p value. NYHA, New York Heart Association; STS, Society of Thoracic Surgeons; CAD, coronary artery disease; GFR, glomerular filtration rate; SAVR, surgical aortic valve replacement; TAVR, transcatheter aortic valve replacement.
Added prognostic utility of multiple biomarkers
The 1-year survival c-statistic for the STS score plus number of elevated biomarkers was 0.702 (95% CI 0.632 to 0.771) compared with the STS score alone (0.667, 97% CI 0.595 to 0.738) (p=0.16 for difference). Compared with the STS score alone, addition of the number of elevated biomarkers provided a 1-year category-free NRI of 64% (95% CI 41% to 87%, p<0.001), including improved reclassification of events (34%) and non-events (30%) (table 3). The IDI was also significant at 1 year (0.037, p<0.001). A similar improvement in net reclassification was observed for 2-year mortality (table 3). Similar results were obtained when evaluating reclassification from adding the number of elevated biomarkers to a clinical model (table 3).
Reclassification of Mortality Risk with Multiple Biomarkers
Biomarkers and tissue fibrosis and inflammation
The associations between each of the biomarkers and myocardial tissue fibrosis and inflammation are shown in online supplementary tables 4 and 5. Representative images are shown in online supplementary figure S1. Only hs-cTnT and the number of elevated biomarkers showed an association with percent collagen area (p<0.05), whereas GDF15, sST2, hs-cTnT, NTproBNP and MCP-1 all showed an association with the number of macrophages in the myocardium (p<0.05).
Discussion
In this prospective cohort of 345 patients with severe AS treated with surgical AVR or TAVR, we showed that multiple biomarkers of cardiovascular stress in combination provide an improved estimate of mortality compared with the STS score alone, which is the most commonly used risk score for patients with AS. After adjustment, an increased number of elevated biomarkers (GDF15, sST2 and NTproBNP) was associated with a higher hazard of mortality after valve replacement. Among patients at intermediate or high surgical risk with an STS score ≥4, those with elevations in all three biomarkers had a 10-fold higher 1-year and 2-year mortality than those with no elevated biomarkers. Importantly, the number of biomarkers elevated improved risk reclassification both by increasing the estimated mortality in those who died and decreasing the estimated mortality in those who survived and its prognostic utility was consistent across subgroups. Despite the differences in the transcatheter and surgical AVR populations, the association between an increased number of elevated biomarkers and increased mortality after valve replacement was consistently observed in both treatment populations. Collectively, these findings provide a proof-of-principle demonstration of the potential utility of multiple biomarkers to aid in risk stratification of patients with AS. Further studies are needed to evaluate their utility in clinical decision-making in specific AS populations.
As in other valvular heart diseases, biomarkers have not played a significant role in the evaluation and management of patients with AS.10 Natriuretic peptides are the only biomarkers that have been widely used in patients with AS, although their role in clinical management decisions is not clearly defined. The US guidelines on valve disease do not incorporate natriuretic peptide levels into clinical decision-making, whereas the European guidelines indicate that valve replacement may be considered (class IIB recommendation) in patients with asymptomatic severe AS with a ‘markedly elevated natriuretic peptide level’.10 ,16 There are emerging, but limited, data on the potential prognostic utility of other biomarkers, such as high-sensitivity troponin in patients with AS.4 Given the adverse prognosis associated with myocardial fibrosis in patients with AS, there has been interest in whether biomarkers that reflect myocardial fibrosis might aid in risk stratification.17 In this regard, the lack of a significant association between any of the circulating biomarkers and tissue fibrosis (except for hs-cTnT) suggests the association between ‘biomarkers of fibrosis’ and the presence of myocardial fibrosis may be weaker than anticipated. Perhaps some of these biomarkers of cardiovascular stress better reflect the degree of myocardial inflammation.
Given the complex cardiovascular and systemic pathophysiology that underlies AS and influences survival in patients with the disease, it is likely that multiple biomarkers reflecting diverse biological pathways (cardiac and systemic) will be more useful in the prediction of clinical outcomes than any one biomarker alone. Indeed, the prognostic utility of combining multiple biomarkers to predict incident heart failure and mortality in the general population and mortality in patients with non-valvular heart failure has been amply demonstrated.5 ,18
Our results demonstrate the potential utility of multiple biomarkers to improve risk stratification of patients with AS. Further studies are needed to evaluate how such biomarker panels might influence patient management and treatment decisions. In lower risk, perhaps asymptomatic, patients with severe AS, discerning the optimal timing of valve replacement surgery and identifying who might benefit from earlier surgical intervention as opposed to careful observation has been a management question that has generated considerable debate.2 ,10 ,16 Multiple biomarkers of cardiovascular stress may identify a group of patients who would benefit from earlier surgery despite the absence of symptoms to maintain long-term cardiac performance, optimal quality of life and freedom from heart failure.
At the other clinical extreme are patients, now often considered for TAVR, with advanced symptoms and numerous comorbidities. Even with TAVR, many of these patients either die soon after the procedure or do not experience an improvement in quality of life, raising questions about the potential benefit versus futility of treatment with TAVR.19 In these patients, using multiple biomarkers in combination with other clinical factors or risk scores may identify those unlikely to benefit from TAVR. Our observation of the effective stratification of mortality risk beyond the STS score suggests the potential utility of a multimarker approach (perhaps with more biomarkers that reflect disease in other organs) in combination with more accurate clinical risk scores to identify a subgroup of patients who have a dismal prognosis even with TAVR.
An additional group of patients with AS in whom a more refined risk stratification is needed are those at intermediate to high risk in whom treatment with TAVR or surgical AVR is feasible. With clinical trials showing similar outcomes after treatment with TAVR or surgical AVR, there will likely be an increasing tendency to treat these patients with the less-invasive approach.20 ,21 However, a subgroup of these patients—perhaps with coexistent significant non-aortic valve disease such as mitral or tricuspid regurgitation or multivessel coronary disease—may benefit from surgical AVR that allows for concomitant mitral or tricuspid valve repair or coronary bypass. A panel of multiple biomarkers that provides insight into anticipated survival may help guide the decision between a more complete surgical procedure (including correction of other valve abnormalities) versus a less-invasive approach with more selective treatment of AS via TAVR.
Limitations
Several limitations should be considered when interpreting these findings. While this cohort of patients was not exclusively comprised of those at higher surgical risk referred for consideration of TAVR, such patients were a large component of our study population as reflected in the older age, relatively high mean STS score and high prevalence of significant comorbidities. However, one-third of our cohort had an STS score <4 and we found no significant interactions for the relationship between the number of elevated biomarkers and mortality based on age or STS score. Additionally, we used the STS score for our analyses on the utility of the biomarkers in reclassifying risk. The STS score was designed to predict operative mortality and perioperative morbidity, not long-term mortality.22 However, the STS score performs reasonably well in predicting longer term mortality and is the most commonly used risk score to assess risk in patients with AS; a better alternative risk score does not currently exist.20 ,21 ,23 Moreover, the prognostic utility of the number of biomarker elevations was similar when adjusting for important clinical factors instead of the STS score. We lacked data on frailty, however, which could be prognostically useful in this patient population. Finally, the evaluation of the association between the biomarkers and ventricular fibrosis may have been influenced by sampling bias and our findings should be confirmed with cardiac MRI studies that measure diffuse fibrosis of the entire ventricle.
Conclusion
A multimarker approach including biomarkers from diverse biological pathways provided a net improvement in risk stratification for mortality in patients with severe AS undergoing valve replacement. Further studies are needed to evaluate the utility of this approach to influence clinical management decisions in distinct populations of patients with AS.
Key messages
What is already known on this subject?
While some studies have demonstrated the prognostic utility of natriuretic peptides, biomarkers have not figured prominently in the risk stratification of patients with aortic stenosis (AS). In heart failure populations without AS, the prognostic utility of multiple biomarkers (evaluated in combination) in addition to clinical factors has been demonstrated.
What might this study add?
We showed that multiple biomarkers of cardiovascular stress in combination provide an improved estimate of mortality in patients undergoing aortic valve replacement compared with the clinical factors or the Society of Thoracic Surgeons score, which is the most commonly used risk score for patients with AS. These findings provide a proof-of-principle demonstration of the potential utility of multiple biomarkers to aid in risk stratification of patients with AS.
How might this impact on clinical practice?
A multimarker approach including biomarkers from diverse biological pathways provided a net improvement in risk stratification for mortality in patients with severe AS undergoing valve replacement. Further studies are needed to evaluate the utility of this approach to influence clinical management decisions in distinct populations of patients with AS.
Acknowledgments
We thank Michael Hesseler, MD, for calculating STS scores, Li He, PhD, for assistance with tissue staining, Douglas L Mann, MD, and Michael W Rich, MD, for their feedback on the manuscript, and the Core Lab for Clinical Studies at Washington University in St. Louis for running the biomarker assays.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online supplement
Footnotes
Correction notice After the original online publication of this manuscript, we discovered that 3 (out of 348) specimens included in the original analysis were mis-labeled and, in fact, were not baseline samples for those 3 subjects. All other specimens were verified to be correctly labeled. When we excluded those 3 subjects, we were left with 345 subjects in the analysis cohort. We re-analyzed all of our results and provided updated Tables, Figures, and text to reflect the results when these 345 subjects were analysed. While there were numerous small changes resulting from the exclusion of these 3 subjects, there were no substantive changes that affected the main results or main messages of the paper. We apologise for the error and any confusion it may have caused.
Contributors All authors have made a substantial contribution to the conception or design of the work, or the acquisition, analysis or interpretation of the data. All authors have drafted the manuscript or revised it critically for important intellectual content. All authors have given final approval of the manuscript submitted. BRL provided overall leadership for the conception and design of the study as well as data acquisition, analysis and interpretation.
Funding This work was supported by NIH K23 HL116660 (BRL), KO8 HL09837305 (JDS), K08 HL114889 (CLH), 5T32HL007081-39 (MAS), American Heart Association grant 13CRP17080096 (BRL), the Gilead Sciences Research Scholars Program in CVD (BRL), Barnes-Jewish Hospital Foundation (BRL, EN), Washington University Mentors in Medicine Program (JGB), and the Washington University Institute of Clinical and Translational Sciences grant (UL1 TR000448, KL2 TR000450) from the National Center for Advancing Translational Sciences (NCATS) of the National Institutes of Health (NIH). Additional support was provided by a research grant from Roche Diagnostics.
Competing interests BRL is a site co-investigator for the PARTNER Trial, has consulted for Gerson Lehrman Group Research, received assay support from BG-Medicine and received a research grant and serves on the scientific advisory board for Roche Diagnostics. AZ has consulted for Edwards Lifesciences and is a member of the PARTNER Trial Steering Committee. HSM is a site investigator for the PARTNER Trial. RJD has consulted for and received grant support from AtriCure, and received grant support and speaking fees from Edwards Lifesciences. JML has consulted for Boston Scientific and Direct Flow Medical, received speaking fees from Boston Scientific and St. Jude, and received stock options from Direct Flow Medical.
Patient consent Obtained.
Ethics approval Institutional Review Board approval was obtained.
Provenance and peer review Not commissioned; externally peer reviewed.