Article Text

Abstract
Background In Africa, screening for asymptomatic rheumatic heart disease (RHD) has been conducted in single communities using non-standardised echocardiographic criteria. The use of different diagnostic criteria has led to widely variable estimates of the prevalence of RHD in the same communities.
Methods Randomly selected school pupils, from 4 to 24 years of age in Bonteheuwel and Langa communities of Cape Town, South Africa, and Jimma, Ethiopia, respectively, were screened for RHD according to standardised evidence-based echocardiographic diagnostic criteria of the World Heart Federation (WHF).
Results We screened 4720 scholars. In South Africa (n=2720), 1604 (58.9%) were female and the mean age was 12.2±4.2 years. In Ethiopia (n=2000), 1012 (50.6%) were female and the mean age was 10.7±2.5 years. Echocardiographic screening revealed 55 cases of definite and borderline RHD by WHF criteria in South Africa and 61 cases in Ethiopia, corresponding to a prevalence of 20.2 cases per 1000 (95% CI 15.3 to 26.2) and 31 cases per 1000 (95% CI 23.4 to 39.0), respectively. The odds of detecting a scholar with RHD in Ethiopia were 1.5 times higher than in South Africa (OR 1.5; 95% CI 1.04 to 2.2, p=0.02). The prevalence of RHD was 27 cases per 1000 (95% CI 19.3 to 36.8) in Langa, and 12.5 cases per 1000 (95% CI 7.1 to 20.2) in Bonteheuwel. The odds of detecting a schoolchild with RHD in Langa compared with Bonteheuwel were 2.2 (OR 2.2; 95% CI 1.2 to 4.2, p=0.0071).
Interpretation There were significant differences in detecting asymptomatic RHD in school pupils of different countries and in different communities within a country in sub-Saharan Africa. The variation in the prevalence of RHD between countries and communities has important implications for the modelling of the global burden of RHD.
Statistics from Altmetric.com
Introduction
Chronic health conditions in children are a growing concern globally.1 The WHO recognises that children can die from preventable and treatable non-communicable diseases (NCDs), such as rheumatic heart disease (RHD), if health promotion, disease prevention and comprehensive care are not provided.2 However, while the importance of NCDs in adults has gained increasing attention, the focus on children still lags behind.3–5 There is little work on the burden of chronic NCDs in poor regions of the world, such as sub-Saharan Africa, where infectious diseases are still predominant.
RHD accounts for the greatest cardiovascular related loss of disability-adjusted life years among 10 to 14-year-olds and continues to represent a major public health challenge in sub-Saharan Africa and other low-income and middle-income countries.6 The prospect of detecting the earliest changes of RHD in endemic populations followed by institution of secondary prophylaxis to retard progress to overt disease has triggered an increasing number of echocardiographic screening studies for RHD over the past 15 years.7 These studies have not only revealed a large burden of subclinical disease in individuals without a history of rheumatic fever, but also demonstrated the superiority of echocardiography over auscultation in detecting early rheumatic structural and functional changes of the mitral and aortic valves.8 However, the lack of standardised criteria for the echocardiographic diagnosis of subclinical RHD has produced widely varying estimates of the prevalence of RHD in the same data set.9 The reliable evaluation of the prevalence of RHD is relevant for the estimation of the burden of disease and for planning the response of the health service.
A standardised evidence-based guideline for the diagnosis of subclinical RHD has been developed by the World Heart Federation (WHF) to improve the reliability, comparability and reproducibility of echocardiographic screening studies.10 We have conducted a study among school pupils in rural Ethiopia and urban South Africa using the WHF criteria. This study provides an opportunity to compare the prevalence of subclinical RHD in communities of different socioeconomic status living in an endemic region and to consider the implications for addressing and managing subclinical conditions such as RHD through a school-health service.11
Methods
Setting and survey methods
We conducted two studies of the prevalence of RHD in South Africa and Ethiopia using the same protocol under the auspices of the Stop RHD A.S.A.P. Programme of the Pan-African Society of Cardiology (PASCAR).12
The first study was conducted in two regions of Cape Town, South Africa, between January 2008 and March 2012 after approval by the Human Research Ethics Committee of the University of Cape Town, and the Departments of Health and Education of the Western Cape Government. The study was conducted in adjacent residential areas of Bonteheuwel and Langa with a total population of 55 707 and 49 667, respectively.13 The majority of the population of Bonteheuwel is of mixed ancestry, whereas the predominant population of Langa is black African. The population of Langa has noticeably poorer socioeconomic indicators compared with Bonteheuwel based on proportion of households with an income <US$200 per month (71.5% vs 36.1%; p<0.05), households with piped water inside the dwelling (35.4% vs 84.1%; p<0.05) and number of non-brick dwellings (49.7% vs 11.5%; p<0.05).14
The site investigators approached the principals of all schools who agreed to participate, rendering a sampling frame of 16 771 students (Bonteheuwel, n=8737, and Langa, n=8034). We used an adaptation of cluster sampling with probability proportional to size with classrooms as the sampling frame.15 The sampling process was conducted in three stages: stratification by residential area (ie, Bonteheuwel and Langa), then by school grade, and then, simple random selection of classrooms. All learners in a selected classroom were invited to participate, and the parents/guardians were asked to sign a consent form. The participants and their parents/guardians were asked to provide information pertaining to past medical history of acute rheumatic fever, RHD and heart disease, in general. Echocardiographic scanning was conducted by a trained echocardiographer using a portable echocardiography machine in a mobile clinic. Images were stored for later review by a paediatric cardiologist who was experienced in diagnosing RHD (LZ).
The second study was carried out in Jimma, Ethiopia, between November 2010 and October 2013 after approval by the ethics committee of the College of Public Health and Medical Sciences of Jimma University. The study was conducted in the community at Gilgel-Gibe Field Research Center (GGFRC) near Jimma City using the same sampling methods as in the first study. One of the authors (AH) was the paediatric cardiologist responsible for scoring the echocardiograms at this site. The GGFRC has eight rural and two urban wards (or ‘kebele’) with a total population of 50 000; 12 427 of whom were school pupils (2010–2011).16
The scholars were interviewed by a research assistant (WD) to determine general health and past history and symptoms of acute rheumatic fever, RHD and other forms of heart disease.
Echocardiographic definitions
Echocardiographic studies were performed by experienced echocardiographers (CEL and MvdW, South Africa; and WD, Ethiopia) in the left lateral decubitus position, using a Vivid I machine, equipped with a 3S probe and tissue Doppler technology, a Philips CX50 with an S5-1 phased-array transducer probe and a Sonosite M-Turbo with the P10 probe. Simultaneous electrocardiography was used for timing of electrical events with mechanical events during cardiac scanning. Standard approaches to transthoracic echocardiography were adopted together with the technical recommendations of the WHF criteria, in particular relating to morphological parameters.17 Three echocardiographers were trained by a paediatric cardiologist in Cape Town (LZ) in the application of the WHF criteria using a training set of echocardiograms, and they followed a standardised protocol for the acquisition of images. All echocardiograms were reviewed by a paediatric cardiologist blinded to the echocardiographer's preliminary diagnosis, and scored according to the WHF criteria for echocardiographic diagnosis of RHD (LZ in Cape Town and AH in Ethiopia).10 A subset of 30 randomly selected echocardiograms from each site were independently reviewed by each cardiologist to measure pairwise agreement. Weighted pairwise kappa testing showed good agreement between the two readers (agreement 91.7%; χ=0.5; SE=0.11, p<0.0001). Furthermore, all normal and abnormal echocardiograms from Ethiopia were independently reviewed by two readers in South Africa, and scored according to the WHF criteria. Any discrepancies were resolved by consensus between three readers (AH, CEL and LZ). Participants with confirmed definite or borderline RHD were referred for consideration for secondary antibiotic prophylaxis and entered into a local registry for continued follow-up.
Statistical analysis
A sample size of 2875 subjects was calculated for each site, anticipating a prevalence of 3% of RHD.18 This sample size assumed a non-participation rate of 5%. With this sample, we would be able to estimate the prevalence of RHD within 0.7 percentage points of precision with 95% CI. Participants were selected by cluster sampling, using the classroom as the unit of randomisation; to account for design effect (i.e. similarity of respondents within a classroom), the sample size was increased by 20% over the 2396 that would have been needed had all participants been independent of each other.
All data were managed in the Department of Medicine at the University of Cape Town with Epi-Info software, and Stata V.11.2 (Cary, North Carolina, USA) was used for the analysis. Descriptive data are presented as means±SD; sample means were compared using the Student's t test. A two-sided p value of less than 0.05 was considered to indicate statistical significance. Comparisons between sites were performed using χ2 or Fisher’s exact test, ORs are presented with CIs as calculated using Stata.
Role of the funding source
The funders had no role in the conception, design, execution, analysis, write-up and decision to publish this study.
Results
South Africa
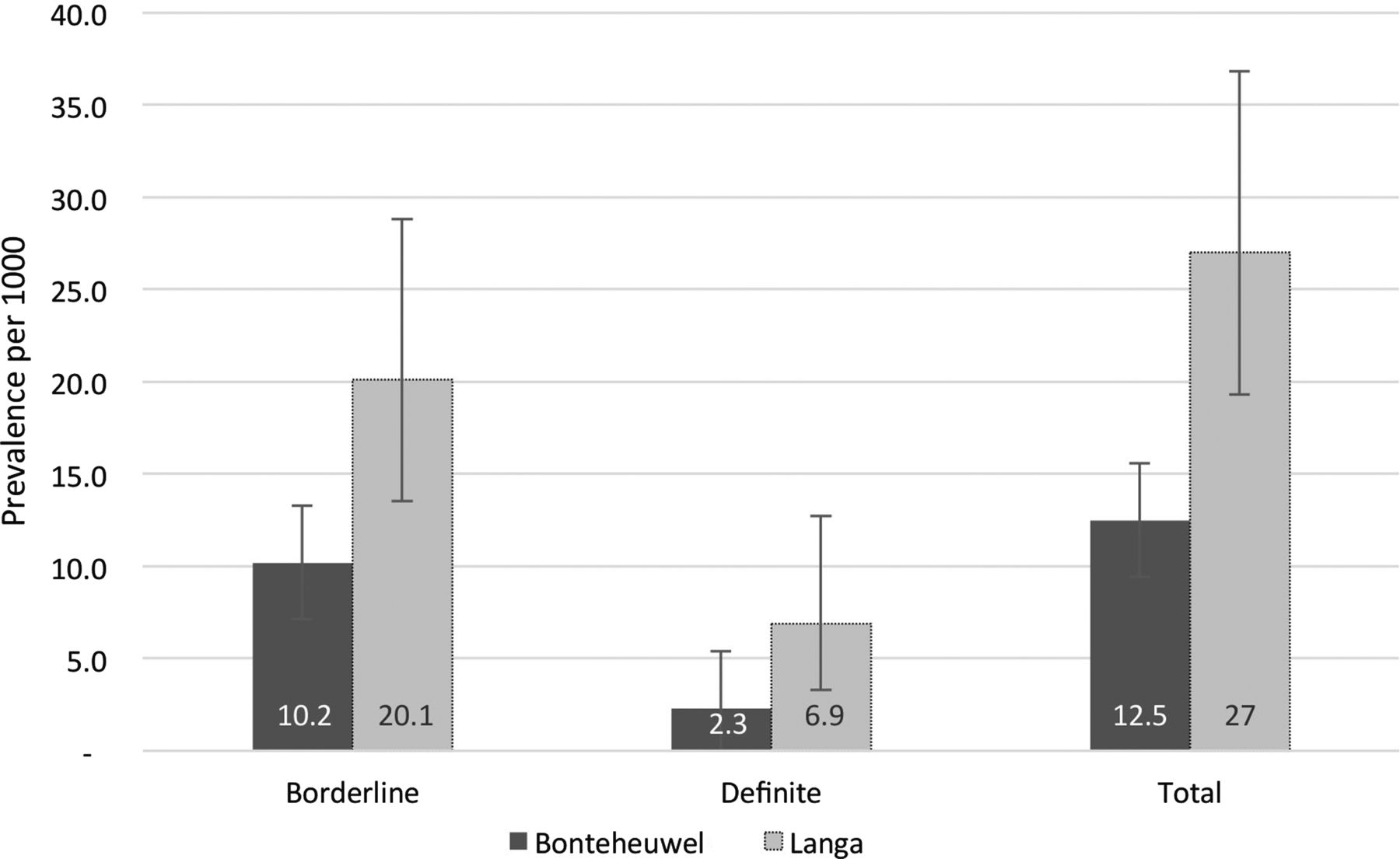
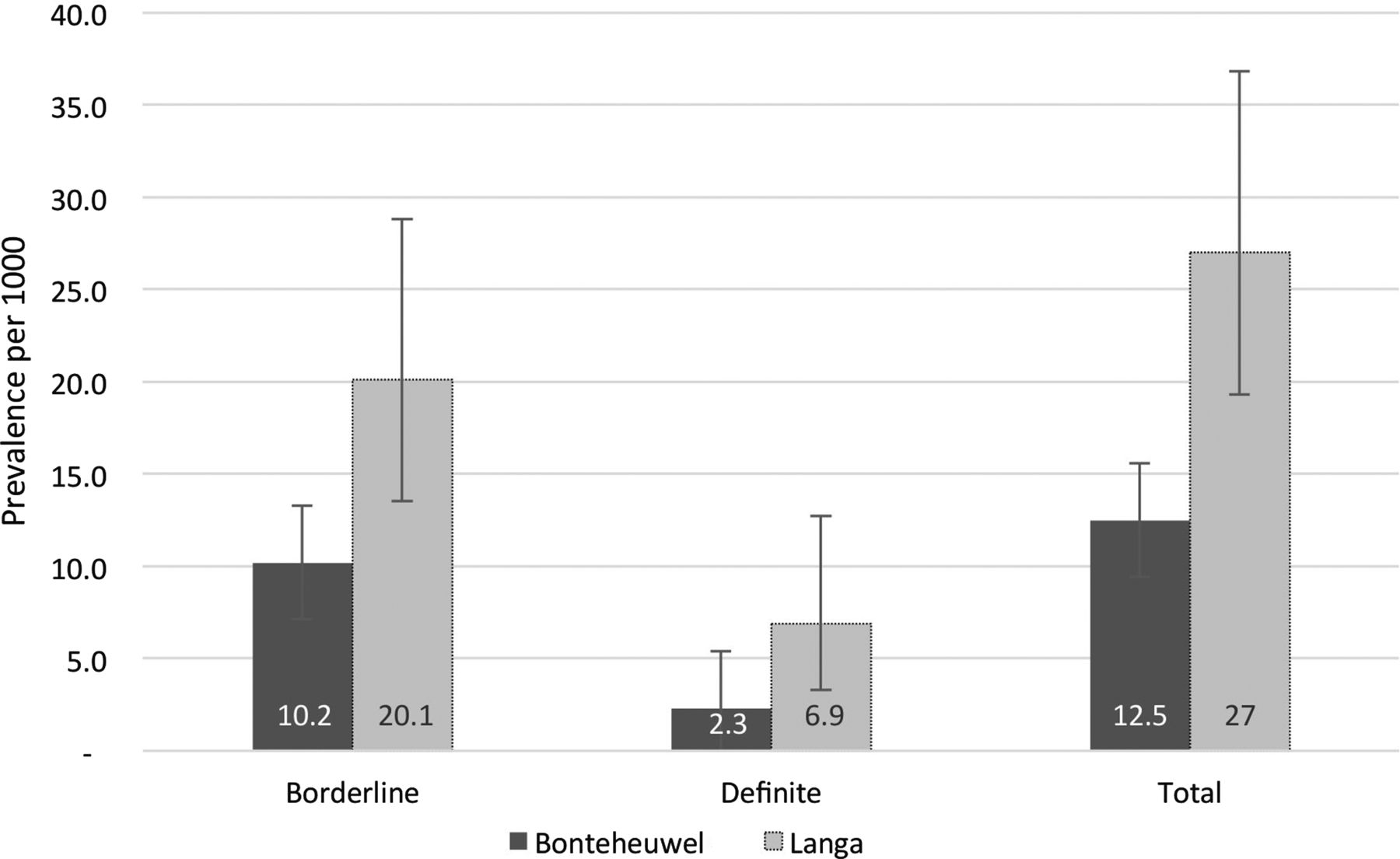
A total of 2875 pupils were invited to participate in this study, 2720 of whom were examined in South Africa. One hundred and fifty-five (5.7%) of pupils who were eligible for enrolment did not participate in the study mainly because of absenteeism and failure to return a signed parental consent form. Table 1 and figure 1 show the age, gender, number of cases of definite and borderline RHD, the prevalence of echocardiographic RHD by country, community and age. Of the 55 subjects with RHD, 13 (23.6%) had definite and 42 (76.4%) had borderline RHD. The odds of detecting a scholar with RHD in Langa compared with Bonteheuwel were 2.2 (OR 2.2; 95% CI 1.2 to 4.2, p=0.0071) (figure 2).
Characteristics of the scholars screened

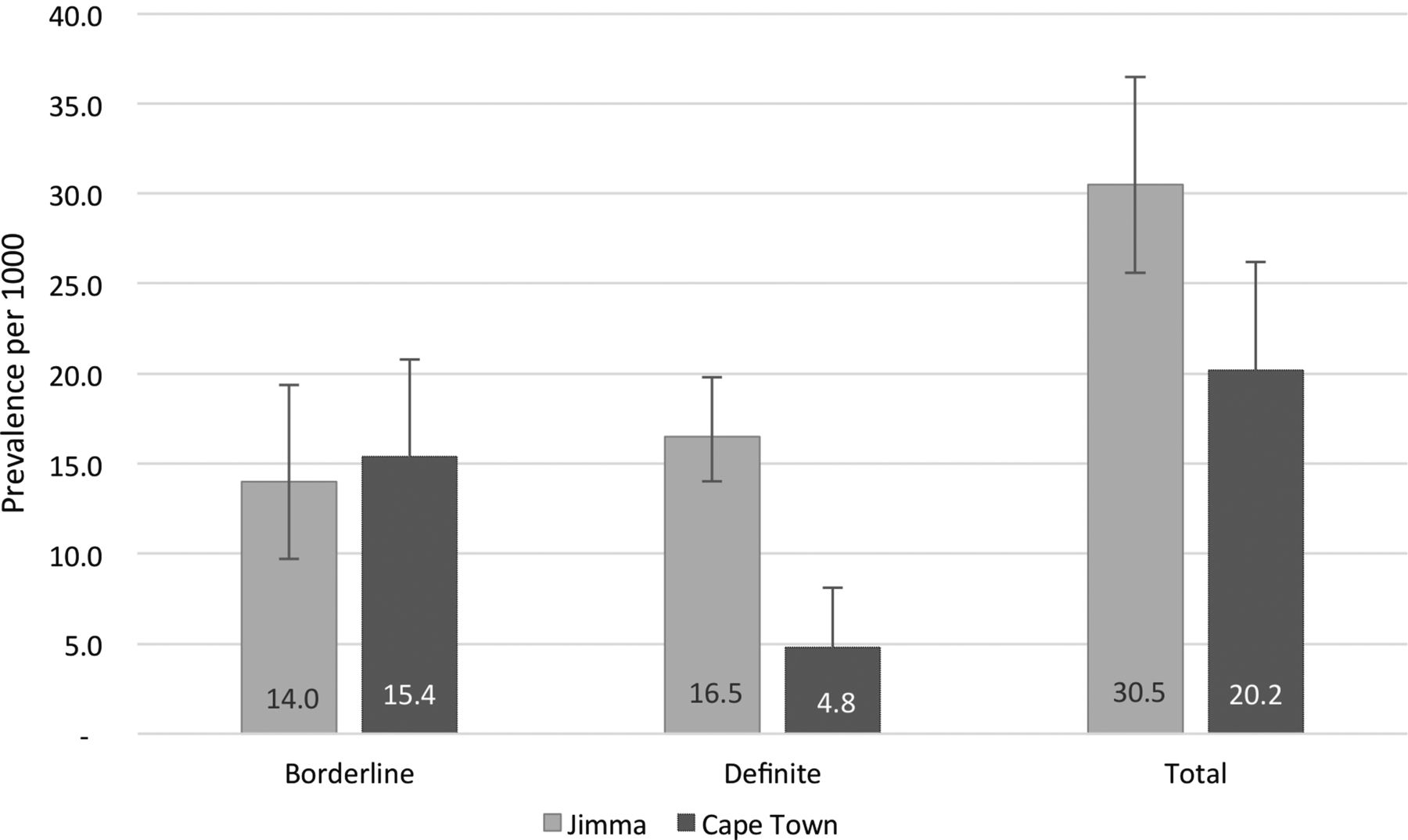
Prevalence of asymptomatic rheumatic heart disease among scholars in Jimma, Ethiopia, and Cape Town, South Africa, by echocardiographic screening.
{kind=link}
{kind=link}
Prevalence of asymptomatic rheumatic heart disease among scholars in the Langa and Bonteheuwel communities of Cape Town, South Africa, by echocardiographic screening.
Ethiopia
A total of 2020 pupils were invited to participate in this study, 2000 of whom were examined in Ethiopia. Twenty (1%) of pupils who were eligible for enrolment did not participate in the study mainly because of absenteeism and failure to return a signed parental consent form. Table 1 and figure 1 show the age, gender, number of cases of definite and borderline RHD, the prevalence of echocardiographic RHD by country, community and age. Of the 61 participants with echocardiographic evidence of RHD, 33 (54.1%) had definite and 28 (45.9%) had borderline RHD. The ratio of definite to borderline cases in Ethiopia was 1.2 compared to 0.3 in South Africa. The odds of detecting a child with RHD in Ethiopia was 1.5 times that in South Africa (OR 1.5; 95% CI 1.04 to 2.2, p=0.02) (figure 1). The odds of detecting definite cases were much higher in Ethiopia than South Africa (OR 3.5; 95% CI 1.8 to 7.3, p<0.0001), whereas the converse applied to borderline disease (OR=0.9; 95% CI 0.5 to 1.5, p=0.7).
Pattern of valve disease
The pattern of valve involvement in definite cases in both countries included two of the four diagnostic categories of the WHF criteria (table 2).10 There were no cases of mitral stenosis nor pathological aortic stenosis with at least two morphological features of the mitral valve. In Ethiopia, 32/33 (84.2%) of definite cases had pathological mitral regurgitation with at least two morphological features of RHD, whereas in Cape Town there were three cases in this category (3/11; 23.1%). In Cape Town, the dominant pattern of definite disease was that of cases characterised by borderline disease of the mitral and aortic valves (10/13; 76.9%).
Pattern of valve disease
Participants in the borderline category in Ethiopia and South Africa had varying proportions of pathological mitral regurgitation (71.4% vs 57.6%), pathological aortic regurgitation (14.3% vs 11.9%) and morphological changes of the mitral valve (14.3% vs 40.5%), respectively.
None of the participants had a past history of acute rheumatic fever.
Discussion
This is the first screening study that has used validated evidence-based criteria for the diagnosis of RHD to allow comparison between different countries and different communities in Africa. There were four main findings. First, there was a high prevalence of RHD in asymptomatic school pupils from South Africa and Ethiopia. The prevalence of echocardiographic RHD (ie, 20–30 per 1000) was much higher than the previous estimates based on clinical auscultation (ie, 4.6–6.9 per 1000) in South African and Ethiopian scholars.19–21 Second, the odds of detecting echocardiographic RHD were different between countries and between adjacent communities from the same country. There was a significantly higher prevalence of asymptomatic disease in Ethiopia compared to South Africa, and in Langa compared to Bonteheuwel in Cape Town. Third, there was variation in the severity of asymptomatic RHD between countries and communities. Scholars from Ethiopia and Langa had more definite disease that those from South Africa and Bonteheuwel, respectively. Finally, these findings suggest that there is a substantial pool of school pupils in South Africa and Ethiopia with definite and borderline RHD who remain undetected. This pool of scholars with a subclinical chronic disease presents a challenge for school-health services.
The heavy burden of asymptomatic RHD in African schoolchildren has been highlighted by four echocardiographic screening studies from Kenya, Mozambique, Uganda and Senegal.8 ,18 ,22 ,23 The prevalence rate of 30 per 1000 and 20.2 per 1000 in Ethiopia and South Africa, respectively, found in this study seems to be typical of sub-Saharan Africa, although there are differences in methods and echocardiographic criteria between these studies. However, the lower frequency of borderline cases of RHD in Ethiopia is counterintuitive. Almost all studies to date have recorded a higher proportion of cases of borderline RHD compared to definite RHD in screening studies.8 ,18 ,23 The higher proportion of definite to borderline cases was confirmed in a reanalysis of the Ethiopian echocardiograms by the South African team, and the inter-reader reproducibility between the paediatric cardiologist in Cape Town and Jimma was remarkably high. This finding, however, remains to be confirmed in future studies.
There are several reasons that may explain the differences in the prevalence rate and pattern of valve disease between Ethiopia and South Africa, and between the communities of Langa and Bonteheuwel. The higher prevalence of RHD in Ethiopia compared with South Africa may not be only related to the differences in income status between the countries (with Ethiopia being low income and South Africa being upper middle income), but also to the largely rural setting of the Ethiopian study compared to the urban environment in Cape Town. Similarly, within Cape Town, the prevalence of RHD was higher in the lower income Langa residential area compared with the higher income Bonteheuwel community. The Ugandan screening study has demonstrated that schoolchildren of lower socioeconomic status had a higher prevalence of subclinical RHD and more advanced disease.8 The higher prevalence of definite compared to borderline disease in Ethiopia compared to South Africa, and in Langa compared to Bonteheuwel is consistent with this observation. However, it was not possible to perform an analysis with explicit adjustment for factors that vary by community and by region because the detailed student level data were not collected. The lack of ability to make such adjusted comparisons is an important limitation of this study. Nevertheless, the apparent variation in prevalence rates of subclinical RHD in endemic countries and communities is relevant for the appropriate modelling of the global burden of RHD.6
The location of these studies in a school setting is both a weakness and strength. It is a weakness because these studies cannot provide information on the population-based prevalence of RHD in children, as has been extrapolated by others.8 ,24 There is a well-known gap between school enrolment and the population, as demonstrated by a drop in school participation among boys after the age of 10 years at the South Africa site.25 Thus, generalisation of these findings may have limitations when considering the population of boys older than 14 years of age. However, the findings of this study are relevant to an existing or developing school health service.
In South Africa and Ethiopia, school health concerns the well-being of approximately 12 million and 20 million learners, respectively, who are attending schools.26 ,27 In recent years the focus on schools as sites of health service provision to the school population and prevention of RHD and other conditions received renewed attention.11 ,28 A recent World Bank Review demonstrated that numerous low-income and middle-incoming countries, including countries across the African continent, have some form of health service provision to school-going students.29 This study reveals that there is a potentially large pool of latent RHD and possibly other chronic health conditions in the school-going population, which highlights the need for national health systems to consider the development of school health services to address preventable chronic conditions such as RHD.11
The 2004 WHO Expert Consultation Report states that echocardiographically diagnosed, clinically silent rheumatic valve involvement should be managed as RHD until proved otherwise.30 However, mass screening for RHD and other chronic health conditions is not a viable option in most country settings, and certainly not in South Africa nor Ethiopia—both because such screening is resource-intense and unaffordable, but also because a consistent referral service response, as a minimum requirement of a good and ethical screening programme, is not available. Furthermore, echocardiographic screening for subclinical RHD remains a research tool pending studies of impact on prognosis.7 At most, targeted screening of high-risk children can be considered and care must be taken when doing so to ensure that the appropriate referral and follow-up services are available.
These findings highlight the need to consider the development of school-health services to meet the needs of the considerable pool of learners with latent chronic diseases such as RHD. Further contemplation is required on how the health needs of children, with as yet undiagnosed, but definite RHD, as well as those newly diagnosed, will be addressed. Here, the link between family, community-based health services, school, school health services where these exist and general health services, including referral services, is critical. In particular, a service response, where good communication, feedback and joint intersectoral management plans that also involve parents/caregivers, is essential.
Conclusion
This study shows a negative correlation between socioeconomic status and prevalence of latent RHD within and between countries. Studies of burden of RHD should take cognizance of the variation in the prevalence of asymptomatic RHD in different countries and different communities in an endemic region such as sub-Saharan Africa. Large-scale prospective investigations of the outcome of subclinical RHD in the school-going population are needed to determine the cost-effectiveness of screening and its impact on prognosis of RHD.7
Research in context
Systematic review
We performed a literature review of publications in PubMed from 28 February 2012 to 9 August 2014, employing no language restriction, on the use of the WHF criteria for the echocardiographic diagnosis of RHD (published on 28 February 2012) in Africa. Search terms included combinations of ‘echocardiography OR echo’, ‘prevalence’, ‘world heart federation’, ‘guidelines’, ‘rheumatic heart OR rheumatic *’ and ‘Africa OR sub-Saharan Africa’. We identified no previous studies which had used the WHF criteria to estimate the prevalence of RHD in Africans.
Interpretation
This study adds to the totality of the evidence in several ways. First, it is the first screening study that has used validated evidence-based criteria for the diagnosis of RHD to allow comparison between different countries and different communities in Africa. Second, we demonstrate that there is significant variation in the prevalence and severity of asymptomatic RHD between different countries and between different communities in the same country. Third, the findings highlight the need to consider the development of school-health services to meet the needs of the considerable pool of scholars with latent chronic diseases such as RHD. Finally, the variations in the prevalence of RHD between countries and communities have important implications for the modelling of the global burden of RHD.
Key messages
What is already known on this subject?
There is a high prevalence of asymptomatic rheumatic heart disease diagnosed by echocardiography in the school population from sub-Saharan Africa, ranging from 10 to 30 per 1000.
What might this study add?
There is variation of the prevalence of asymptomatic rheumatic heart disease measured by echocardiography between and within countries; the variability appears to follow the socioeconomic gradient.
How might this impact on clinical practice?
These findings highlight the need to develop school-health services to meet the needs of the considerable pool of school pupils with asymptomatic rheumatic heart disease.
Acknowledgments
The financial assistance of the National Research Foundation of South Africa for MSK’s contribution towards this research is hereby acknowledged.
References
Footnotes
MEE, AH and LZ contributed equally.
Contributors BMM conceived the study and wrote the first draft of this paper. BMM, MEE, LZ and AH designed the protocol and supervised the collection of data. CEL, MvdW and WD collected and collated the data in Ethiopia. SN organised the fieldwork, entered and collated the data in South Africa. MEE and LZ conducted the statistical analysis. LZ and AH oversaw the clinical aspects of the studies. MSK wrote the sections on the health policy and service implications of the study. All authors approved the final version.
Funding This study was funded by grants from the Life Healthcare Foundation, South African Medical Research Council, Lily and Ernst Hausmann Research Trust, Else Kröner Fresenius Foundation, the University of Cape Town, the National Research Foundation of South Africa and the World Heart Federation. LZ was funded in part by the Discovery Foundation Academic Fellowship, the United States National Institutes of Health Fogarty International Clinical Research Fellowship, the Thrasher Research Fund Early Career Award, the Wellcome Trust Clinical Infectious Disease Research Initiative (CIDRI) Research Officer Award and the Hamilton Naki Clinical Scholarship during the course of this work.
Competing interests None declared.
Ethics approval University of Cape Town Faculty of Health Sciences Human Research Ethics Committee.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement All data related to this are available from the authors upon request.