Article Text

Abstract
Objective Whether sex-related differences in the prognosis of infective endocarditis (IE) are due to differences in disease severity or comorbid patterns, physiological specificities or a treatment indication bias is unclear. We conducted an analysis of the pooled database of two population-based cohorts of IE to reassess the relationships between sex, early valve surgery (EVS) and outcome in patients with IE.
Methods Demographic and baseline characteristics, complications and outcome were compared in men and women with Duke-definite left-sided IE. A propensity model for EVS was constructed using multivariate logistic regression. Factors associated with 1-year mortality were identified using multivariate Cox models adjusted for EVS factors.
Results The study population included 466 (75%) men and 154 (25%) women. Compared with men, women were older (p=0.005), were more often on haemodialysis (p=0.04), more often had a mitral valve IE (50.0% vs 35.8%, p=0.02), less often developed a septic shock (p=0.05), less often underwent EVS (p=0.001) yet had comparable inhospital mortality rates (20.1% vs 20.0%, p=0.96) and similar 1-year survival probability (logrank p=0.68). Female sex was neither associated with EVS (OR 0.76 (95% CI 0.49 to 1.16)) nor mortality (HR 1.17 (95% CI 0.80 to 1.69)). However EVS was associated with an increased risk of death in women in the early postoperative period (HR 8.72 (95% CI 3.42 to 22.24), p=<0.0001).
Conclusions Women underwent EVS less often than men. However female sex was independently associated with neither EVS nor 1-year mortality. The reasons for a higher risk of early postoperative mortality in women must still be elucidated.
Statistics from Altmetric.com
Introduction
Nearly every previously published study showed that infective endocarditis (IE) occurs more frequently in men than in women, with a male:female sex ratio >2 : 1.1–6 The pathophysiological explanations for this observation remain speculative and largely unknown. In the last few years, it was also suggested that characteristics of IE are different in women and in men. Several studies showed that women are more likely to have more severe manifestations of IE and/or more severe underlying conditions, are less likely to undergo early valve surgery (EVS), and are more likely to have worse outcomes, particularly a higher mortality rate.7–10 Studies that analysed factors associated with EVS provide conflicting results. In their study performed in 439 patients (187 women), Aksoy et al found that female sex was associated with a lower rate of EVS but was not associated with mortality after adjustment for confounding factors. The authors suggested that sex difference in the rate of EVS resulted mainly from pre-existing and/or coexisting conditions such as diabetes, haemodialysis and chronic immunosuppression, which were more frequent in women.7 The study by Sambola et al, performed on 271 patients (88 women), found different results. Although women in this cohort were older than men, they did not have more comorbid conditions and yet they underwent EVS less frequently than men when surgery was indicated. The authors attributed the worse outcome observed in women to their lower rate of EVS.10
However it is important to note that the analytical methods used in the studies by Aksoy et al and Sambola et al were suboptimal. First, in both studies, cases were identified in tertiary care centres, to which the most severe patients and/or those needing cardiac surgery are referred, which potentially induced a referral bias.11 Second, although the two studies correctly used adjusted Cox models with 1-year mortality as the end point, the EVS variable was entered in the model as a binary variable (yes vs no), which introduces a survivor selection bias and usually results in an inaccurate overestimation of a protective effect of surgery.12
Thus it is still unclear whether sex-related differences in the prognosis of IE result from one or more of the following factors: sex-related physiological differences; actual differences in disease severity or pre-existing and comorbid patterns; a treatment indication bias; uncontrolled confounding factors; or inappropriate modelling methods. Therefore we decided to re-evaluate the relationship between sex, EVS and outcome of IE using a data set obtained from two population-based studies and appropriate analytical methods, which included EVS propensity-adjusted Cox models, 1-year mortality as an outcome and coding surgery as a time-dependent variable. We first assessed the relationship between sex and EVS in a propensity model and then we assessed the relationship between sex and 1-year mortality in a multivariate Cox model adjusted for EVS propensity factors.
Methods
Study population and clinical data
We used the pooled data bases of two French population-based cohorts of IE that were initiated in 1999 and 2008. The methods used for data collection in these cohorts were identical and are described in detail elsewhere.3 ,6 In brief, all consecutive adult patients diagnosed with IE between 1 January and 31 December of the study year in the participating regions (six regions with a total population of 16 million in 1999, seven regions with a total population of 19.5 million in 2008) were enrolled in each study. Only definite cases of left-sided IE using the Duke criteria modified by Li13 were analysed, the assignation to a Duke category being validated by independent experts for each individual case.
The following data were collected: sex, date of birth, residence, dates of first symptoms and first hospitalisation, transfer from/to another facility, history of heart disease, comorbidities (including diabetes mellitus, cancer, dialysis and immunosuppressive therapy), Charlson comorbidity index,14 procedures and other risk factors for IE, signs and symptoms of IE, echocardiographic data, microbiological data, laboratory and imaging findings, medical and surgical treatment, and outcome. Location of IE was determined by echocardiographic findings and was updated by surgical findings, as needed.
EVS was defined as valve surgery performed during antibiotic treatment. Inhospital mortality was defined as death from any cause during hospitalisation. One-year mortality was defined as death from any cause within 1 year after the diagnosis of IE.
Outcomes
The primary outcome end point was 1-year mortality. Information on each patient’s condition at that end point was collected using one or more of the following: review of hospital medical records, interviews of the patient’s general physician, the register of births and death, or, when necessary, by direct phone contact with the patient. Information collected included at least patient’s status (alive/dead), occurrence of IE relapse and performance of valve surgery.
Statistical analyses
Men and women were compared for demographics, clinical characteristics and outcome characteristics using the χ2 test for categorical variables and the Wilcoxon rank-sum test for continuous variables.
Univariate and multivariate logistic regression analyses were used to identify predictors of EVS. Candidate variables were those known to be potentially associated with EVS based on prior studies: sex, age, number of comorbidities, hypertension, diabetes mellitus, current smoking, intravenous drug use, previous IE, fever, streptococcal IE, staphylococcal IE, location of IE, valve perforation, intracardiac abscess, valve dehiscence, severe regurgitation, cardiac failure, septic shock, vascular event, serum creatinine >180 µmol/L, C reactive protein >120 mg/L.15–19 Variables entered into multivariate model were sex, survey and those associated with EVS in univariate analysis with p<0.2. A stepwise selection method was used with a threshold of entry of 0.1 and a threshold of exit of 0.05. The validity of the logistic regression models was checked using the Hosmer and Lemeshow goodness-of-fit test. Results are expressed as ORs and 95% CIs. Probability of 1-year mortality was compared between men and women using Kaplan-Meier curves and logrank test. Probability of 1-year mortality was analysed in Cox models, using the same variable selection method as for factors associated with EVS. In all Cox models, EVS was analysed as a time-dependent variable. The impact of EVS on 1-year mortality was further analysed after partitioning the follow-up time after valve surgery in two periods: (1) short-term, from Day 0 to Day 14 after valve surgery, and (2) long-term, from Day 15 to Day 365 after valve surgery. Results are expressed as HRs and 95% CIs.
All statistical analyses were performed using SAS V.9.2 (SAS institute, Cary, North Carolina, USA).
Results
The study population included 466 (75%) men and 154 (25%) women with definite, left-sided IE. EVS was performed in 301 patients (48.5%). EVS rate was not significantly different whether patients had native valve IE or prosthetic valve IE (50.1%, 42.5%, p=0.36).
Compared with men, women were older (64.3 years vs 60.4 years, p=0.005), received chronic haemodialysis more often (5.2% vs 1.9%, p=0.04), had a mitral valve IE more often (50.0% vs 35.8%, p=0.02), developed a septic shock less often (4.0% vs 9.0%, p=0.05), underwent EVS less often (37.0% vs 52.4%, p=0.001), and had similar inhospital mortality rate (20.1% vs 20.0%, p=0.96) and 1-year mortality rate (26.6% vs 24.9%, p=0.67) (table 1).
Characteristics of infective endocarditis (IE) according to sex
In multivariate analysis, the usual predictors of EVS (younger age, aortic location of IE, valve perforation, intracardiac abscess, severe regurgitation and congestive heart failure) were confirmed to be associated with EVS, whereas female sex was not (OR 0.76 (95% CI 0.49 to 1.16)) (table 2).
Variables associated with EVS: bivariate and multivariate propensity logistic regression analyses
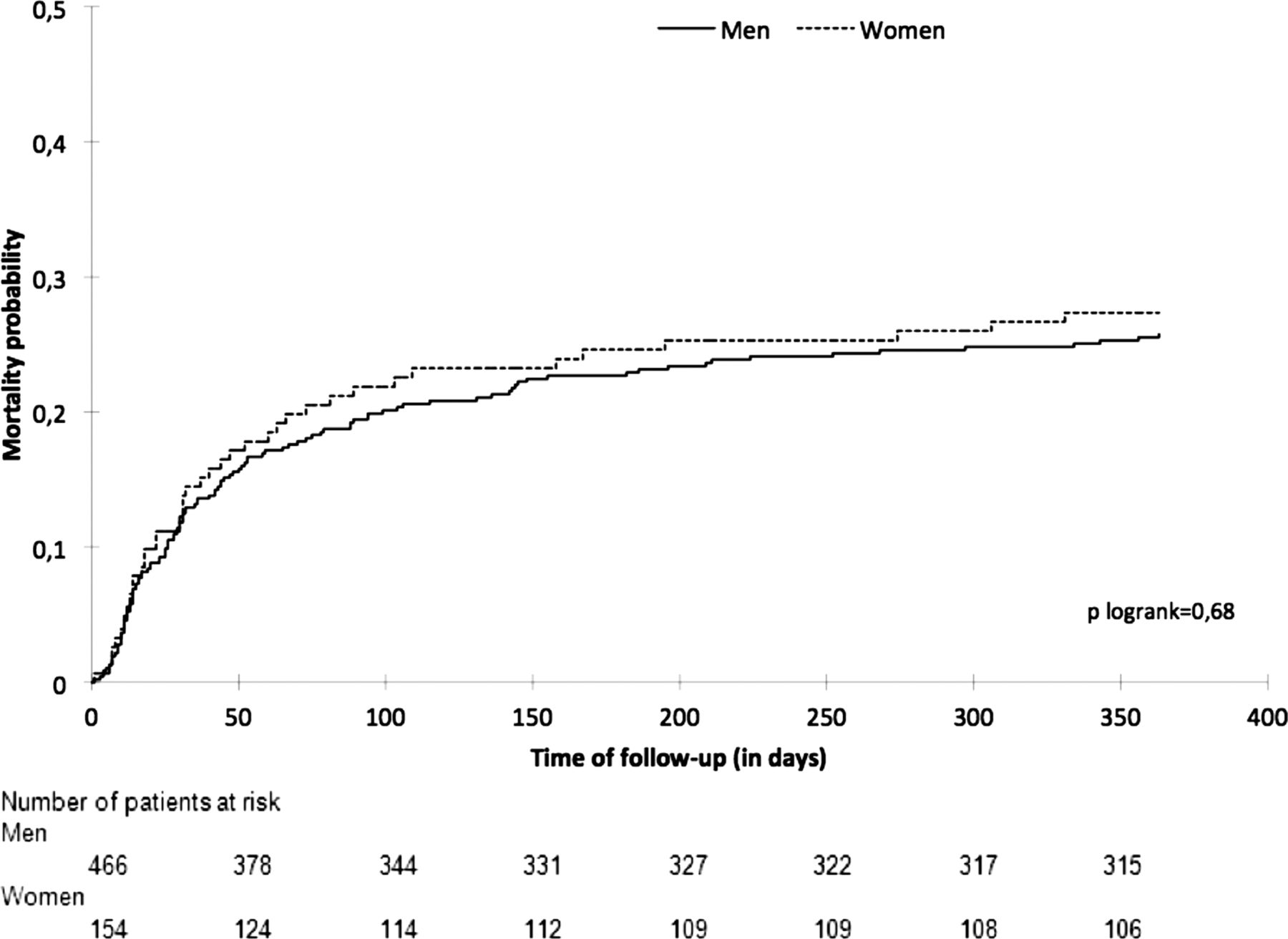
The probability of 1-year mortality was similar in men and women (logrank p value=0.68, figure 1). Factors associated with 1-year mortality included age ≥65 years, number of comorbidities, cardiac failure, vascular event or septic shock, serum creatinine level higher than 180 µmol/L, C reactive protein level higher than 120 mg/L, and EVS, which was associated with an increased mortality during the 14 days following surgery (table 3). Being female was not a significant predictor of 1-year mortality (HR 1.17 (95% CI 0.80 to 1.69). The impact of EVS on 1-year mortality was different in men and women (table 4). When entering EVS as a time-dependent and a time-partitioned variable in the multivariate Cox model, EVS was associated with a significant higher risk of short-term mortality and a decreased risk of long-term mortality in men and women. The increased risk of short-term mortality was more pronounced in women (p for interaction equal to 0.03). A trend towards a long-term benefit of EVS was observed in men whereas a trend towards a long-term higher risk of mortality persisted in women.
Variables associated with 1-year mortality
Relationship between EVS and 1-year mortality, by sex. Multivariate Cox model, with EVS as a time-dependent partitioned variable

{kind=link}
1-year mortality probability, by sex. Kaplan-Meier curves and logrank comparison.
Discussion
The main findings of our study are threefold: (1) the clinical presentation of IE differs in men and women, with women being older and having more comorbid conditions than men; (2) although women underwent EVS significantly less frequently than men, sex was not an independent predictor of EVS; and (3) although sex was not an independent predictor of 1-year mortality, women had a significantly higher risk of early postoperative mortality than men.
In this study we minimised the impact of potential referral bias by using data from two large population-based cohort studies. We also used appropriate analytical methods in order to minimise any other biases, especially survivor selection bias when analysing the relationship between valve surgery and outcome.12
However, this study has two significant limitations. The most important one is that we do not have information about the complications or events that occurred after EVS, especially within the first 14 days. Thus, we cannot identify factors other than female sex that might have contributed to early mortality after surgery. On the other hand, we do not have information on the reasons why EVS was not performed, which are essentially twofold: absence of indication or contraindication to surgery. It could have been helpful to compare the distribution of these two reasons between men and women. For instance men may have been more prone to undergo EVS because they had aortic valve IE more often than women or women may have been denied surgery because of apparent frailty.
Compared with the two major publications about sex differences in IE,7 ,10 our findings are similar in terms of women's demographics and baseline characteristics: women with IE are older than men, more often on haemodialysis and more often have a mitral valve IE. In all three studies, women underwent EVS less often than men. Sex was not an independent predictor of EVS in our study and in Aksoy et al’s. In Sambola et al’s, female sex was associated with a lower relative risk of EVS (RR 0.4 (CI 95% 0.2 to 0.7)) and EVS was less often indicated in women than in men (36% vs 54%, p=0.008). The authors suggested that EVS was performed less often in women because of factors influencing the decision to rule out valve surgery such as older age or higher rate of comorbidities and because women more often had mitral valve IE, a condition associated with a lower rate of valve surgery. Actually, the main indications for EVS in IE are heart failure, uncontrolled infection and prevention of embolic events.20 ,21 Heart failure is the most frequent complication of IE and is more often observed in aortic valve IE than in mitral valve IE. Moreover, in our study, aortic valve IE was identified as a predictor of EVS, whereas mitral valve was not and women more often had mitral valve IE and had or tended to have heart failure, systemic embolism or septic complications less often than men. In summary our data are consistent with the explanation that EVS was performed less often in women because there were fewer indications for valve surgery in women than in men.
Results on mortality in the three studies are different. Inhospital mortality rate was higher in women than in men in studies by Aksoy et al and Sambola et al (22.5% vs 12.7%, p=0.007 and 32% vs 23%, p=0.05 respectively) as was 1-year mortality rate in the study by Sambola et al (38% vs 26%, p=0.04). Conversely, we found that inhospital mortality and 1-year mortality rates were similar in women and men. In our study, the relationship between EVS and sex-related 1-year mortality using a multivariate adjusted Cox-model with time-partitioned EVS variable showed—not surprisingly—a higher risk of mortality in the early postoperative period. Interestingly this risk was more pronounced in women than in men (HR 8.72 (95% CI 3.42 to 22.24) and HR 2.26 (95% CI 1.32 to 3.86), respectively). Unfortunately, we can hardly explain this observation because we could not compare the causes of death between men and women. Interestingly, in a recent study aimed at evaluating mortality and morbidity in patients who survived IE, Thuny et al22 found that women exhibited a higher risk of age-adjusted mortality, especially those who had developed an aortic valve IE. Sex-related outcome differences were also observed in other surgical procedures such as cardiac valve surgery in patients with no IE, and coronary artery bypass graft surgery.23–25 Being female was identified as independently associated with higher risk of postoperative death (OR 1.19, p<0.001) in the American Society of Thoracic Surgeons valve surgery database that included 176 096 women. Interestingly, among other variables associated with postoperative death, there were endocarditis (OR 1.59, p<0.001), congestive heart failure (OR 1.39, p<0.001), acute presentation (OR 2.11, p<0.001), advanced age (OR 1.88, p<0.001) and comorbidity (OR 1.19, p<0.001).23 When focusing on mitral valve surgery, Song et al24 showed that inhospital mortality rate was higher in women compared with men with similar risk factors (p=0.048). They and others26 suggested that oestrogen withdrawal states observed in postmenopausal women may potentiate ischaemia-reperfusion injury by impairing endothelial function, increasing endothelial cell apoptosis, and increasing levels of tumour necrosis factor α and interleukin 6, eventually contributing to a higher mortality risk after surgery in women. Thus, female sex per se appears to be a prognosis factor of postoperative mortality, but pathological mechanisms require elucidation.
In sepsis and severe infections, the impact of sex on management strategies, outcomes and mortality has also been explored, but conclusions remained controversial and sex differences were often associated with confounding factors.27 ,28
In summary, our study confirms that clinical characteristics and outcomes of IE are different in men and women. Although EVS was performed less often in women, female sex was neither independently associated with EVS nor with 1-year mortality. Interestingly, we showed that women with IE had a higher risk of early postoperative mortality, as shown previously after other cardiac surgical procedures. The reasons for this higher risk of mortality after surgery require further elucidation.
Key messages
What is known on this subject?
-
Previous studies showed that infective endocarditis (IE) occurs more frequently in men than in women, and suggested that characteristics of IE differ by gender. Several studies showed that women are more likely to have more severe manifestations of IE and/or more severe underlying conditions, are less likely to undergo early valve surgery (EVS), and are more likely to have worse outcomes and a higher mortality rate.
-
Whether sex-related differences in the prognosis of IE are due to differences in disease severity or comorbid patterns, physiological specificities, or a treatment indication bias remains unclear.
What might this study add?
-
We conducted an analysis of the pooled database of two population-based cohorts of IE to re-evaluate the relationships between sex, EVS and outcome in patients with IE.
-
Our study confirmed that:
-
the clinical presentation of IE differs in men and women, with women being older and having more comorbid conditions than men;
-
although women underwent EVS significantly less frequently than men, sex was not an independent predictor of EVS;
-
although sex was not an independent predictor of 1-year mortality, women had a significantly higher risk of early postoperative mortality than men, which had been shown previously after cardiac surgery in other indications. The reasons for this higher risk of mortality after surgery require further elucidation.
-
How might this impact on clinical practice?
-
In women who undergo valve surgery for IE, attention should be paid to their care during the early postoperative period, especially in those who have comorbid conditions.
Acknowledgments
The authors are indebted to the investigators who participated in the AEPEI EI1999 and EI2008 studies. They also want to thank G Ralph Corey, M.D., Daniel J Sexton, M.D., and Vance G Fowler Jr, M.D., for their thoughtful comments in the preparation of the manuscript.
References
Footnotes
-
Contributors All authors have seen and approved the manuscript, and contributed significantly to the work.
-
Funding The EI 2008 study was supported by a research grant from the French Ministry of Health (Programme Hospitalier de Recherche Clinique 2007), grants from the Société Française de Cardiologie, the European Society of Clinical Microbiology and Infectious Diseases, and Novartis France, and the Société Française de Chirurgie Thoracique et Cardiovasculaire. The EI 1999 study was supported by a research grant from the French Ministry of Health (Programme Hospitalier de Recherche Clinique 1997), the Fédération Française de Cardiologie, and the Aventis and GlaxoSmithKline Laboratories, France. For both studies, the sponsor was Délégation à la Recherche Clinique et à l’Innovation, Centre Hospitalier Universitaire de Besançon.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.