Article Text

Abstract
Objectives To ascertain if motivational techniques and a structured exercise programme can increase activity in adolescents afflicted with congenital heart disease (CHD).
Design Prospective randomised controlled trial.
Setting One hundred and forty-three patients aged 12–20 years attending the tertiary centre for paediatric cardiology in Northern Ireland.
Main outcome measures Increase in exercise capacity as assessed by duration of exercise stress test, and number of minutes spent in moderate to vigorous physical activity (MVPA) per day.
Results Eighty-six patients were men (60%), mean age was 15.60±2.27 years. Seventy-three percent were considered to have major CHD. Seventy-two participants were randomised to the intervention group. Following intervention, duration of exercise test increased by 1 min 5 s for the intervention group (p value 0.02) along with increase in predicted VO2Max (p value 0.02). There was a significant increase in minutes of MVPA per day for the intervention group from baseline to reassessment (p value <0.001) while MVPA remained much the same for the control group. Fourteen patients met the current recommendation for more than 60 min MVPA per day at baseline. This doubled to 29 participants at reassessment. There were no adverse effects or mortalities reported.
Conclusions Exercise training is safe, feasible and beneficial in adolescents with CHD. Psychological techniques can be employed to maximise the impact of interventions.
Trial Registration Number ISRCTN27986270.
- CONGENITAL HEART DISEASE
Statistics from Altmetric.com
Introduction
Improved survival among children afflicted with congenital heart disease (CHD) has dramatically increased the number of adolescents and adults with complex heart conditions. The spectrum of adult congenital heart disease (ACHD) in the UK is one of a young population with a relatively low rate of mortality but high morbidity.1
Ability to exercise has received attention recently as an important prognostic indicator. There is evidence that exercise limitation correlates with outcome in terms of predicting hospitalisation and death in patients with ACHD.2 Capacity for exercise is variable, and it has been suggested that exercise intolerance affects around one-third of patients with CHD.1 ,3 Many patients have a positive attitude towards exercise but may be unsure of what is appropriate or beneficial.4–6
The role of exercise-based rehabilitation is well established. Recently, the benefits of exercise programmes have begun to extrapolate to CHD. A small number of studies with mixed methodologies have demonstrated that improvements in exercise capacity may be made and maintained.7 ,8 Participation in, and adherence to, exercise training is variable but could be influenced by motivational interview style techniques designed to move an individual through the stages of change in relation to exercise behaviour.
Since physical activity has emerged as an important quality-of-life measure affecting functional status, structured training programmes may be useful to improve psychological well-being, as well as protecting cardiovascular health.9 The developmental crucible of adolescence, during which adult behaviours are tested and become established, is an ideal time for health promotion strategies, which could potentially influence the public health burden of tomorrow's adults.
This study aimed to ascertain if an exercise-based motivational session followed by a structured programme of exercise training could be used to increase physical activity and improve psychological health in a group of adolescents with CHD who attend the tertiary centre for paediatric cardiology in Northern Ireland. This paper reports findings related to physical activity.
Methods
Recruitment
This was a prospective randomised controlled trial. Ethical approval was obtained from the Office for Research Ethics Committee of Northern Ireland.
Suitable patients aged 12–20 years were identified from the Heartsuite Database at The Royal Belfast Hospital for Sick Children (RBHSC). Four hundred and fifty-five patients were approached to participate in the study with a detailed information pack sent by post or provided at clinic. Patients were excluded if they had a syndromic diagnosis, major learning difficulty, or if exercise was contraindicated (ie, severe left ventricular outflow tract obstruction, severe aortic stenosis). Informed consent was obtained at the first visit, which was carried out in the Department of Paediatric Cardiology, RBHSC. Participants were divided into major and minor CHD groups. Major CHD was defined as any condition requiring lifelong catheter or surgical intervention. Participants were subdivided into four groups based on diagnosis (shown in table 1), to facilitate further detailed comparison.
Diagnostic groupings and demographics of study participants
Preliminary assessment
Each participant underwent a full clinical examination including assessment of growth parameters. Body Mass Index (BMI) was calculated using the standard formula and converted into SD scores (SDS) using BMI reference curves for the UK (Cole et al). Deprivation, an indication of socioeconomic status was assessed using the multiple deprivation measure based on the electoral ward available on the Northern Ireland Neighbourhood Information Service (NINIS) website, a branch of the Northern Ireland Statistics and Research Agency (http://www.ninis.nisra.gov.uk last accessed 8th August 2012). A low deprivation index indicates the individual comes from a more deprived area.
Assessment of activity
Participants completed an activity questionnaire to self-rate their physical activity and answer some general questions about exercise habits (after Casey et al 1994).10
A formal exercise stress test (EST) was carried out on a treadmill ergometer using a Marquette 2000 treadmill connected to a Maxpersonal Exercise Testing System (Marquette, Wisconsin, USA). Participants were encouraged to exercise to their maximum capacity (within reason) using the graded treadmill exercise protocol described by Bruce et al.11 Exercise was discontinued when the participant reached 85% of maximum predicted heart rate for age, stated he/she could go on no longer or if any non-reassuring data were recorded. A 12-lead ECG was recorded at baseline and at 3 min intervals during exercise and recovery. Blood pressure was measured at 3 min intervals during exercise with a manual sphygmomanometer. Oxygen saturations were continuously monitored during exercise using a Nellcor N-20 pulse oximeter (Nellcor Purition Bennell, Pleasanton, USA) attached to the left earlobe and recorded at 3 min intervals. Each patient was recovered for 6 min with full monitoring before the test was terminated. VO2max was estimated from the EST data using the Bruce Cardiac Max equation that is, predicted VO2max=(2.33×duration of EST (minutes)+9.48.12
Day-to-day free-living activity was assessed using an ActiGraph GT1M accelerometer (ActiGraph, Pensacola, Florida). The ActiGraph GT1M is a dual-axis accelerometer designed to monitor human activity and record energy expenditure. It has been extensively validated as a reliable measure of activity in both children and adults during walking/running and free-living activities13 ,14 Each participant was asked to wear an ActiGraph during their waking hours for 1 week (7 days). The accelerometer was positioned around the subject's waist, and securely held against the body using the elastic belt. The device was programmed to collect data in normal activity mode over 60 s epochs. Patients were required to complete at least 4 days of wear including 1 weekend day for their data to be submitted for analysis. Activity counts were downloaded using the ActiLife software interface (ActiLife V.3.5.1. 2008) for data reduction and subsequent analysis. Moderate to vigorous physical activity (MVPA) (>3 metabolic equivalents (METs)) was estimated (approx >2200 counts/min) by established methods using age-specific cut points.15 Average number of minutes per day spent in MVPA was calculated and compared with current physical activity recommendations for 5–18-year-olds in the UK.16
Randomisation and intervention programme
Participants were randomised using balanced blocks of four to intervention and control groups. Randomisation was not stratified by any factor. Intervention group participants were invited to attend one of six activity days held in The Queen's University of Belfast Physical Education Centre.
The activity day was conducted as a motivational interview style group exploring the nature of motivation towards exercise using small group and visualisation techniques. The concept of motivation was introduced. Participants completed a motivational ratings sheet assessing their own feelings towards the importance of exercise, confidence and readiness with regard to increasing their activity presession and postsession.
During the session, group members discussed the pros and cons of exercise along with ways to surmount obstacles to a healthy active lifestyle. Participants spent time visualising themselves as fitter, more active individuals, and how they would feel on completion of the programme. Each participant was seen individually and suggestions were discussed for ways to increase their activity over the next 6 months in a manner suitable for their diagnosis. They were also given a written exercise training plan to implement at home.
The activity day was followed-up with a letter summarising the discussions from the group. Each participant was contacted once a month to check on progress with their exercise plan and discuss any problems. Participants could contact the research team at any stage should they have any interim problems.
The control group participants received their usual level of care from the Department of Paediatric Cardiology, RBHSC. All participants were recalled for reassessment after the 6-month intervention period was completed for each individual in the intervention group, and baseline measures were repeated.
Analysis
Data obtained were analysed with PASW Statistics V.18.0 for Mac (SPSS, 1989–2010) using parametric methods as the dataset satisfied the assumptions of normality. Major and minor groups were compared using an independent samples t test and study subcategories (acyanotic no-intervention, acyanotic corrected, cyanotic corrected and cyanotic palliated) were analysed using a one-way analysis of variance (ANOVA). Posthoc tests were conducted when a significant F-statistic was obtained from the ANOVA on an a priori basis; no Bonferroni corrections were employed.
Outcomes between the intervention and control groups at baseline and reassessment were compared using a general linear model multivariate analysis of variance with repeated measures. For all tests, p<0.05 was accepted as significant.
Results
Participants
One hundred and forty-three patients were recruited, 86 were men (60%) and the mean age was 15.60±2.27 years. Seventy-three percent were considered to have major CHD. There were no significant differences between study participants versus non-responders in terms of age, number of men, diagnostic group or deprivation measure. The distribution of participants across four diagnostic subgroups is given in table 1. There were no significant differences in deprivation measure among major/minor groups or study subcategories. Most individuals fell within two SDs of their expected mean for growth parameters. Participants with major CHD had lower SDS for weight (table 1) and posthoc analysis confirmed that complex individuals are shorter and lighter (minor CHD no-intervention vs cyanotic palliated group; height SDS p value 0.03 (CI 0.06 to 1.48), weight SDS p value <0.01 (CI 0.23 to 1.77), BMI SDS p value 0.04 (CI 0.02 to 1.51)).
Activity at baseline
There were no significant differences in activity score across major/minor groups. Ninety-four percent of participants stated they exercised regularly each week (ie, played a sport or went to the gym), with 47.6% exercising more than three times per week, and 56.6% said they played a sport each week.
One hundred and forty-two participants attempted a formal EST, one patient left before completing all the assessment components. There were no significant differences between major and minor groups for duration of exercise, predicted VO2max or maximum METs achieved during exercise. Mean exercise time (minutes) was comparable between three of the subgroups; minor CHD no-intervention (11.7±3.4), acyanotic corrected (11.4±3.3) and cyanotic corrected (11.5±3.0) groups. ANOVA demonstrated that cyanotic palliated patients have a markedly reduced exercise tolerance (8.3±4.0) compared with the other subgroups (p value 0.01). There were significant differences in predicted VO2max (p value 0.01) and maximum METs (p value <0.01) achieved.
One hundred and thirty-nine (97.2%) received an actigraph accelerometer; one patient left his first appointment before it was complete, and three did not return to collect a monitor when one became available for them. Mean number of days of wear was 5.72±1.29 days with 11.0±1.7 h of wear per day. Six individuals (4.3%) wore their actigraph for less than 4 days; therefore, this data was not submitted for analysis. Accelerometer data is included in table 1. There were no significant differences in minutes of MVPA per day between major and minor groups or across study subgroups.
Intervention programme
Seventy-two participants were randomised to the intervention group and 71 participants to the control group. There were no significant differences between intervention and control groups in terms of age, sex, diagnostic group, activity or psychological variables at baseline. There was a significant difference between the groups in terms of deprivation measure with the intervention group having a higher index, meaning that they came from a less deprived area (table 2). Consequently, deprivation measure was used as a covariate for subsequent analysis.
(a) Characteristics of intervention and control groups at baseline, (b) Exercise parameters of intervention and control groups at reassessment
In total, six intervention activity group sessions were held. Four patients who were randomised to the intervention group did not attend the group sessions offered. These patients were analysed with the rest of the intervention group on an intention-to-treat basis. Mean number of participants in each group was 11.3±4.6. Feedback from the intervention groups was positive. Postsession means for the motivational ratings scale components were significantly higher that is, importance of exercise 7.8±2.3, p value <0.01 (−1.27, −0.65); confidence to change behaviour 7.6±2.1, p value <0.01 (−1.35, −0.59); readiness to change behaviour 7.7±2.0, p value <0.01 (−1.27, −0.61), highlighting the effect the session had on these issues.
Reassessment
One hundred and one patients (70.6%) attended for reassessment. Twenty-three participants did not attend despite being offered three separate appointments, and a number of patients withdrew at this stage. A significantly higher number of participants were lost from the control group (χ2 test 16.75, p value <0.001). There was no significant difference in percentage loss from across the study subgroups (χ2 1.6, p value 0.66) or between sexes (χ2 3.89, p value 0.06). Figure 1 summarises participant progression through the study. There were no significant differences between growth parameters for study groups at reassessment.

Participant progression through study.
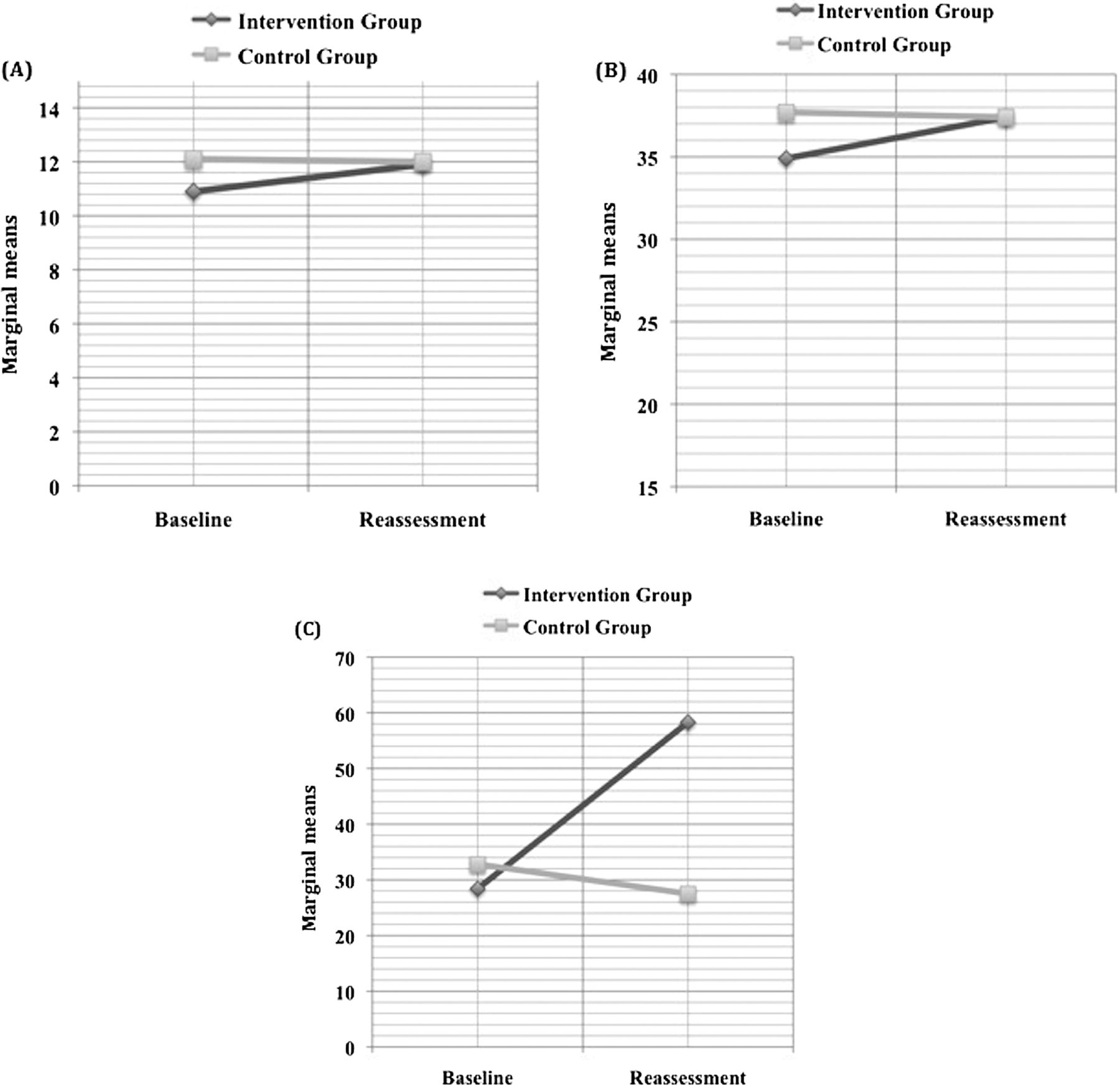
There were distinct differences on exercise testing between intervention and control groups at reassessment. The duration of exercise test increased by 1 min 5 s for the intervention group (p value 0.02). The intervention group also had a significant increase in predicted VO2Max (p value 0.02) compared with baseline. There was a trend to increased maximum METs achieved at peak exercise among the intervention group members at reassessment, although this did not reach statistical significance (table 2 and figure 2).
{kind=link}
{kind=link}
Plots of marginal means for (A) Duration of EST, (B) Predicted VO2max, (C) Minutes spent in moderate to vigorous physical activity per day (covariate—deprivation).
Ninety-eight patients (97%) received an actigraph accelerometer for reassessment. Three study participants opted not to have the activity monitor for a second time as they felt wearing it was too disruptive to their day-to-day lives. Mean number of days of wear was 4.86±1.11 days with 10.2±1.9 h of wear per day for reassessment. Five participants (4.95%) wore the monitor for less than 4 days in total; therefore, their data was not submitted for analysis. There was a significant increase in average minutes of MVPA per day for the intervention group from baseline to reassessment (p value <0.001) while minutes of MVPA remained much the same for the control group (table 2 and figure 2). Fourteen patients met the current recommendation for more than 60 min MVPA per day at baseline. This doubled to 29 participants at reassessment. There were no adverse effects reported and no mortality during the intervention programme.
Discussion
Improved survival among children afflicted with CHD has shifted focus to patients having the best possible outcome in terms of quality of life and functional status. This study demonstrates that patients with CHD can safely participate in activity and an exercise-based motivational session followed by a 6-month self-implemented exercise-training plan which can produce significant gains both in peak exercise capacity and day-to-day activity levels in young people with CHD who are maintained in the short term.
The majority of patients participate in exercise each week and a large number of them play sport competitively. This includes the most complex patient group. There were no significant differences in activity score among the study groups indicating that patients with complex CHD consider themselves to be as active day to day as those with less complex problems. However, subjective measures of activity are inherently flawed, and self-reported measures might be unreliable.2 Exercise testing in this group confirmed that complex patients are limited at peak exercise, even if they consider themselves to be asymptomatic. These findings are similar to those reported by Diller et al.2
As these patients are young and relatively ‘well’, it may be that they have not yet reached a point in the natural history of their condition where exercise limitation truly becomes apparent. Low levels of activity documented in patients with ACHD may reflect a poor exercise capacity, development of more symptoms, or a general deterioration in health with age.2 ,17 Studies in patients with ACHD also show there is potential for increasing exercise capacity through training18 indicating that this phenomenon cannot be entirely blamed on symptomatology alone. Perceived functional status and self-efficacy are important determinants of activity, meaning that it is not what someone is capable of that is important, but what they perceive they are capable of.19 The psychological well-being of this group will be discussed in a companion paper (under preparation).
The concept of exercise training as a method of improving exercise tolerance in patients with CHD has been around since the 1990s.20 However, it is only in recent years that, following the heart-failure paradigm, that cardiac rehabilitation for patients with CHD has begun to receive a lot of attention as a method of altering morbidity and mortality for the future. There is firm evidence that diminished exercise capacity is linked to hospitalisation and death in patients with a wide range of conditions, including transposition of the great arteries, tetralogy of Fallot, and single ventricle physiology.2 ,20–23 There are a limited number of studies examining exercise training in young people with CHD.6–8 ,24 These have offered encouraging results, however, methodologies are mixed, in particular, with regard to the structure of the exercise training programme. Many require patients to travel to participate in each session. Few of the current published studies include education, activity counselling or psychological intervention, all of which are key components of adult cardiac rehabilitation theory.
The study presented here is unique in terms of exercise training intervention. It used a psychotherapy style session based on motivational interviewing techniques to educate about exercise, stimulate and maintain changes in exercise behaviour. Participants received an individual training plan to implement at home. Education and personal choice form key components of the intervention. Motivational ratings scales completed presession and postsession, indicated the very strong effect the sessions had on confidence and readiness to change exercise behaviour. At reassessment, the intervention group had significantly increased their day-to-day MVPA, and the number reaching the recommended 60 min of MVPA doubled.
Traditional exercise programmes are difficult to maintain. They require significant input in terms of time, facilities and resources. The intervention programme described here can be implemented with existing resources on a sustainable basis. It can easily be adapted to include patients outside urban areas and has a significant impact on activity levels. There is evidence that most patients are willing to participate in exercise but are uncertain as to the safety or benefits. Reviews recommend that activity participation should form part of outpatient clinic discussion.6 ,25 A motivational style intervention and a home-based exercise training plan would fit neatly into formal transition programmes for this patient group.
Study limitations
There are a number of limitations to this study which should be noted. Of the 455 patients approached, only 143 (31.4%) chose to participate, 37 less than desired based on the initial power calculation. There were small numbers of patients in the most complex group despite efforts to recruit the maximum number of patients possible. At 6-month follow-up, the number of patients continuing in the study had fallen to 101 with an attrition rate of 29.4%. A larger number of participants were lost from the control group, which could be expected, as they did not receive any contact during the intervention period other than their normal input from the tertiary centre. Compared with other studies involving similar techniques whose sample size ranges from 20–60 patients, sample numbers obtained here, and the number of patients retained throughout, is really quite large.26–28 Historically, such studies attract small sample groups, as the effort required from both parties involved is enormous.
Many potential participants may have perceived the study as requiring considerable effort in terms of time and travel to study sessions from distant parts of Northern Ireland, especially when one considers these would be combined with their usual medical checkups. The decision to participate is the result of a mixture of motivations. The premise of the study may have appealed to individuals who were already interested in activity. There was limited information available regarding activity levels among non-responders although there were no significant differences across other variables. A number of methods were employed to assess activity, however, the accelerometers were not waterproof and had to be removed for water-based activities and may, therefore, have under-represented activity levels in some participants. VO2Max was not measured directly due to resource limitations, but was predicted using a standard equation. Future studies could use physical work capacity (PWC170) as a marker of maximal oxygen uptake.
Conclusions
This study confirms that adolescents with CHD can exercise safely, and that training programmes are both feasible and beneficial for young people with CHD. This study is unique in that it employed psychological methods to maximise the impact of its interventions. Consideration for issues, such as maintenance of activity, psychological well-being and promotion of good lifestyle choices must be given when planning formal transition programmes for this group and other services for their future.
Acknowledgments
The authors gratefully acknowledge statistical advice provided by Dr Chris Patterson.
References
Footnotes
-
Contributors FAC, AJS Concept, study design, and revision of manuscript. MLM study design, recruitment, data collection, analysis and interpretation, manuscript preparation and revision. PPMcK study design and revision of manuscript. CMcC MMcM psychological support. BGC, BG recruitment.
-
Funding This work was funded by a research fellowship from RBHSC Medical Staff Committee.
-
Competing interests None.
-
Ethics approval ORECNI.
-
Provenance and peer review Not commissioned; externally peer reviewed.