Article Text

Abstract
Objective To evaluate the agreement between multislice CT (MSCT) and intravascular ultrasound (IVUS) to assess the in-stent lumen diameters and lumen areas of left main coronary artery (LMCA) stents.
Design Prospective, observational single centre study.
Setting A single tertiary referral centre.
Patients Consecutive patients with LMCA stenting excluding patients with atrial fibrillation and chronic renal failure.
Interventions MSCT and IVUS imaging at 9–12 months follow-up were performed for all patients.
Main outcome measures Agreement between MSCT and IVUS minimum luminal area (MLA) and minimum luminal diameter (MLD). A receiver operating characteristic (ROC) curve was plotted to find the MSCT cut-off point to diagnose binary restenosis equivalent to 6 mm2 by IVUS.
Results 52 patients were analysed. Passing–Bablok regression analysis obtained a β coefficient of 0.786 (0.586 to 1.071) for MLA and 1.250 (0.936 to 1.667) for MLD, ruling out proportional bias. The α coefficient was −3.588 (−8.686 to −0.178) for MLA and −1.713 (−3.583 to −0.257) for MLD, indicating an underestimation trend of MSCT. The ROC curve identified an MLA ≤4.7 mm2 as the best threshold to assess in-stent restenosis by MSCT.
Conclusions Agreement between MSCT and IVUS to assess in-stent MLA and MLD for LMCA stenting is good. An MLA of 4.7 mm2 by MSCT is the best threshold to assess binary restenosis. MSCT imaging can be considered in selected patients to assess LMCA in-stent restenosis.
Statistics from Altmetric.com
Introduction
Multislice CT (MSCT) is an evolving non-invasive technique able to reconstruct accurately the lumen contours of coronary arteries.1–5 Although the evaluation of coronary stents is challenging, due to artefacts created by the metal of the struts, MSCT has proven reliable in assessing in-stent restenosis.6–8 The accuracy of MSCT to assess in-stent restenosis is even better when large stents (>3 mm nominal diameter) are investigated.9
Coronary artery bypass grafting (CABG) is considered to be the recommended treatment for left main coronary artery (LMCA) stenosis.10 ,11 However, percutaneous coronary intervention (PCI) of LMCA stenosis can be considered for patients with a low SYNTAX score and for patients who are not suitable for CABG.12–14 Although routine follow-up invasive coronary angiography in patients with LMCA stenosis treated with PCI is under debate, this has been suggested in current European guidelines to be performed at 3–12 months follow-up.13 In those patients, intravascular ultrasound (IVUS) allows a more accurate analysis of the LMCA stent, the assessment of neointimal hyperplasia, and the assessment of lumen area and diameter than coronary angiography.15
Non-invasive imaging techniques such as MSCT can be helpful to evaluate in-stent restenosis in patients with LMCA stenting at follow-up.16 ,17 However, there is a lack of information comparing the in-stent lumen dimensions between MSCT and IVUS imaging. Furthermore, the role of MSCT to assess in-stent restenosis in patients with LMCA stenting in routine clinical practice is not well defined.
The aim of the present study is to evaluate the agreement between MSCT and IVUS to assess the in-stent lumen diameter and lumen areas of LMCA stents at follow-up. A secondary end point of the present study is to define a cut-off value for MSCT derived minimum luminal area (MLA) that is able to predict significant in-stent restenosis.
Methods
This is a prospective, observational single centre study. Since November 2010 all consecutive patients with de novo LMCA stenosis treated with stenting were included in the study. MSCT was performed in all patients 9–12 months after LMCA PCI. None of the recruited patients presented with symptoms previous to the scheduled MSCT. Coronary angiography and IVUS were performed within a week of the follow-up MSCT imaging.
Exclusion criteria were chronic renal failure with creatinine clearance <60 ml/min, previous allergic reaction to contrast media, contraindication to β-blocker treatment, and atrial fibrillation or atrial flutter. All patients provided written informed consent and the protocol was approved by the local ethics committee.
MSCT
Non-invasive coronary angiography was performed with a 64-slice CT scanner (Lightspeed VCT 64-slice GE Medical Systems, Waukesha, Wisconsin). Patients with a heart rate over 65 beats/min received propranolol (1 mg/ml) intravenously to reduce their heart rate. A bolus dose of 80 ml of contrast (iodixanol, 320 mg of iodine per 1 ml; Visipaque, GE Healthcare UK) was infused at 5 ml/s and saline solution was infused immediately after the iodine contrast to reduce hyperattenuation of the right cavities (20 ml at 5 ml/s). No non-contrast study was previously performed.
MSCT data were acquired by the fluoroscopic bolus tracking technique, which was started as soon as the signal density level in the ascending aorta reached a threshold of 100 Hounsfield units.
Scan parameters were as follows: a detector collimation width 64×0.625 mm, gantry rotation time 350 ms, 0.2 pitch, and use of dose modulation (peak tube current of 600 mA during 65–85% of the R-R interval and minimal tube current of 300 mA). For estimation of the effective dose, the product of the dose–length product and the chest organ weighting factor (k=0.014 mSv×(mGy×cm)–1 averaged between male and female models) was calculated.18
Image reconstruction was retrospectively gated to the ECG. An experienced radiologist and an experienced cardiologist jointly evaluated the original axial images and multiplanar reformatted reconstructions. Cross-sectional orthogonal lumen areas and diameters were measured throughout the entire stent length and the minimum luminal diameter (MLD) and MLA were visually determined and assessed. Stent external and internal diameters including the blooming artefact can be easily defined along the stent.19 In case there was no evidence of neointimal proliferation, we measured the internal diameter with electronic calipers, as some grade of neointimal proliferation could be hidden by the artefact. When the neointimal proliferation was large enough to overtake the blooming artefact and be detected by MSCT, the MLD and MLA were measured. Analyses of MSCT images were performed at a dedicated workstation (GE Medical Systems, Waukesha, Wisconsin, USA).
A semiquantitative analysis of the MSCT data was also performed. The stent segment, including its proximal and distal borders, was analysed in detail. In the case of LMCA bifurcation stenting, each of the three segments (LCMA, left anterior descending, and circumflex coronary artery) were evaluated individually. The stent was classified as patent when no neoproliferation or a non-obstructive neoproliferation was seen; it was classified as in-stent restenosis when >50% narrowing of the lumen diameter was detected. Binary angiographic stenosis was also assessed at the left anterior descending and left circumflex coronary ostia. Stents not assessable by MSCT were defined when binary in-stent restenosis could not be ruled out due to the bad quality of the images; stents not assessable were assigned as having binary in-stent restenosis.
X-ray coronary angiography
Conventional coronary angiography was performed using standard techniques after intracoronary injection of 2 mg glyceryl trinitrate (GTN). Two or three orthogonal views were performed, without foreshortening or side-branch overlap. The same views were repeated immediately after the procedure and at late follow-up. Quantitative coronary angiography was performed by an experienced analyst blinded to the MSCT data with dedicated software (CAAS II system, Pie Medical, Maastrich, The Netherlands). The MLD, MLA, and binary angiographic in-stent restenosis rate (>50% diameter stenosis) were assessed within the in-stent segment.
IVUS
IVUS imaging was performed at follow-up according to standard procedures. Following the administration of 5000 IU heparin and 2 mg GTN, the IVUS catheter (Boston Scientific Atlantis SR 2.8F 40 MHz) was positioned at least 10 mm distal to the stent edge in the left anterior descending artery. IVUS imaging was recorded during an automatic pullback at 0.5 mm/s. Two experienced observers, blinded to the MSCT imaging, analysed the IVUS images using quantitative coronary ultrasound by dedicated software (QCU-CMS, MEDIS, Leiden, The Netherlands). This system performs a previous contour correction for cardiac motion artefacts using a combination of transversal and longitudinal contour detection techniques that allow accurate two and three dimensional analysis.20 MLA, mean stent area, MLD, mean stent diameter, and maximal neointimal hyperplasia (mm) were estimated within the stent segment.
Statistics
Continuous normally distributed variables were presented as mean ±SD, and non-normally distributed variables were presented as median and IQR. Categorical variables were presented as counts and percentages. Continuous variables were compared by Student's t test when variables were normally distributed and by Mann–Whitney U test when variables were non-normally distributed. All tests were two-tailed, and a p value of 0.05 was considered significant. Categorical variables were compared by χ2 test. All statistical analyses were performed with PASW statistics 18.0 (SPSS Inc, Chicago Illinois, USA).
Agreement analysis between MSCT and IVUS imaging was performed using the Passing–Bablok regression analysis and Bland–Altman plots. In brief, Passing–Bablok regression analysis obtains an α and β coefficient. The α coefficient assesses the systematic bias: a confidence interval (CI) below zero denotes a constant underestimation trend whereas values over zero denote an overestimation trend. The β coefficient assesses the proportional bias: a good agreement is present when its CI includes 1.21 Bland–Altman analysis reveals the delta between both techniques and its CI. Furthermore, consistency and absolute interclass correlation coefficients (ICC) were obtained in order to further discern possible additive or proportional differences. An ICC <0.4 indicates bad agreement, an ICC between 0.4 and 0.75 indicates moderate agreement, and ICC values >0.75 indicate excellent agreement.22 Agreement between binary variables was measured with the κ index.
Test accuracy (percentage of patients correctly classified), sensitivity, specificity, and positive and negative predictive values of MSCT for the detection of in-stent restenosis compared to quantitative coronary angiography were calculated on a per patient basis. A receiver operating characteristic (ROC) curve was plotted in order to find the cut-off point of MLA assessed by MSCT to identify in-stent restenosis better, using as gold standard an MLA of 6 mm2 determined by IVUS, which is a recently validated clinically significant MLA for LMCA lesions.23
Results
Seventy-two patients with previous PCI of LMCA were screened. A total of 52 patients met the inclusion criteria and were prospectively included. Eight patients were excluded because of atrial fibrillation, 10 patients due to chronic renal failure, and two patients because they withdrew consent. An MSCT study was performed at a median follow-up of 331 days (IQR 295–386 days) after PCI of LMCA. All but one underwent coronary angiography at a median of 7 days after MSCT. This patient withdrew consent after undergoing MSCT and was also excluded from the study. After MSCT examination IVUS images could not be obtained in four patients because of failure to progress the IVUS catheter through the stent (severe stenosis, angulated anatomy or stent protrusion into the aorta). These patients were excluded from quantitative analysis.
Patient demographics and procedural findings are summarised in tables 1 and 2, respectively. More than 70% of the patients were treated with a single stent technique and the mean stent diameter was 3.42 mm, permitting a correct evaluation of stent patency with MSCT (table 2). MSCT characteristics are shown in table 3. Two patients could not be assessed because of severe vascular calcification and movement artefacts resulting from an inability to maintain prolonged apnoea. Both were classified as presenting in-stent restenosis. No procedure complications developed in any of those cases. Table 4 shows LMCA stent measurements by quantitative coronary angiography, MSCT, and IVUS. Agreement analysis for MLD and MLA is shown in figure 1. Bland–Altman plots for the MLA and MLD values between MSCT and IVUS are shown in figure 2A and B and revealed a good agreement for both MLD and MLA; however, the derived MSCT, MLD, and MLA values presented with an underestimation trend of 0.4 mm and 2 mm2 with respect to IVUS derived parameters. Bland–Altman plots also showed good agreement between MSCT and quantitative coronary angiography for MLD (figure 2C).
Clinical features
Procedural characteristics
Multislice CT features
Measures of left main coronary artery stents

Passing–Bablok regression results. (A) Agreement between multislice CT (MSCT) and intravascular ultrasound (IVUS) minimum luminal diameter (MLD). (B) Agreement between MSCT and IVUS minimum luminal area (MLA). (C) Agreement between MSCT and quantitative coronary angiography (QCA) MLD.
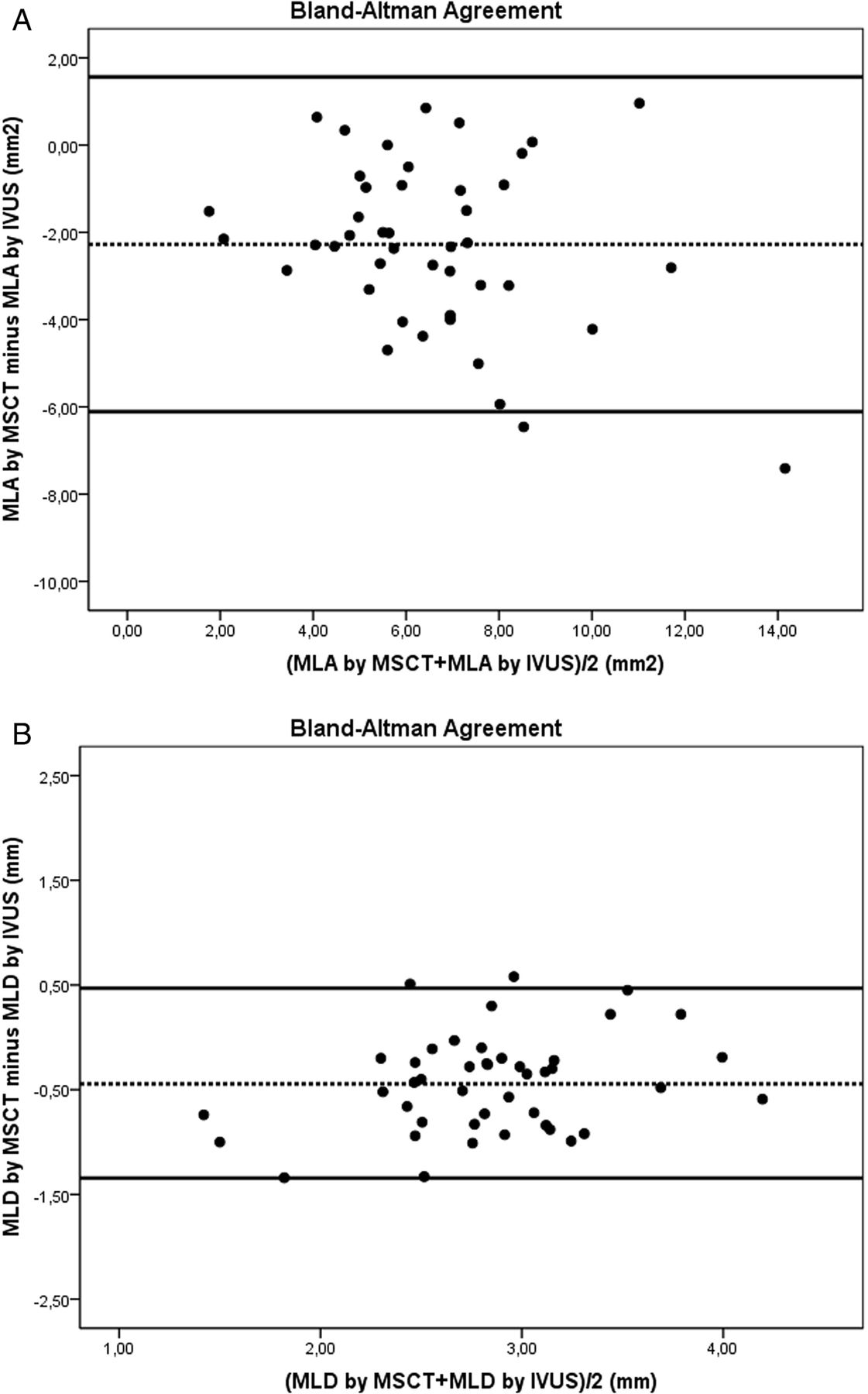
Agreement analysis using Bland–Altman regression between multislice CT (MSCT), intravascular ultrasound (IVUS), and quantitative coronary angiography (QCA). (A) Comparison of MSCT and IVUS minimum luminal diameter (MLD). (B) Comparison of MSCT and IVUS minimum luminal area (MLA). (C) Comparison of MSCT and QCA MLD.
Agreement between MSCT and IVUS measured by consistency ICC was excellent both for MLD (0.826, 95% CI 0.681 to 0.905) and MLA (0.823, 95% CI 0.675 to 0.903), whereas absolute ICC was moderate for MLD (0.717, 95% CI 0.084 to 0.886) and MLA (0.666, 95% CI 0.143 to 0.874). Agreement between quantitative coronary angiography and MSCT derived MLD was good both for consistency and absolute ICC: 0.792 (95% CI 0.661 to 0.889) and 0.753 (95% CI 0.478 to 0.876), respectively.
On coronary angiography, 14% of patients presented with binary in-stent restenosis. MSCT accuracy to predict angiographic binary in-stent restenosis was 88% (95% CI 58.0% to 97.3%), with a sensitivity of 90% (95% CI 59.6% to 98.2%), a specificity of 90% (95% CI 78.0% to 96.0%), a positive predictive value of 69.2% (95% CI 38.9% to 89.6%), a negative predictive value of 97.3% (95% CI 84.2% to 99.8%), and a κ index of 0.719. There was one false negative case; this patient was treated with a T stent technique and presented with side branch restenosis. There were four false positive cases, all of them with a complex two stent technique.
On IVUS, 15% of patients presented with in-stent restenosis (MLA ≤6 mm2). The ROC curve, with the cut-off point that best defines significant restenosis by MLA assessed by MSCT, is plotted in figure 3. An area under the curve of 0.811 (95% CI 0.673 to 0.950) was obtained, showing that an MLA <4.7 mm2 was able to detect significant restenosis with a sensitivity of 87%, a specificity of 62%, a positive predictive value of 66%, and a negative predictive value of 94%. Figures 4 and 5 show examples of the correlation of MSCT and IVUS images.
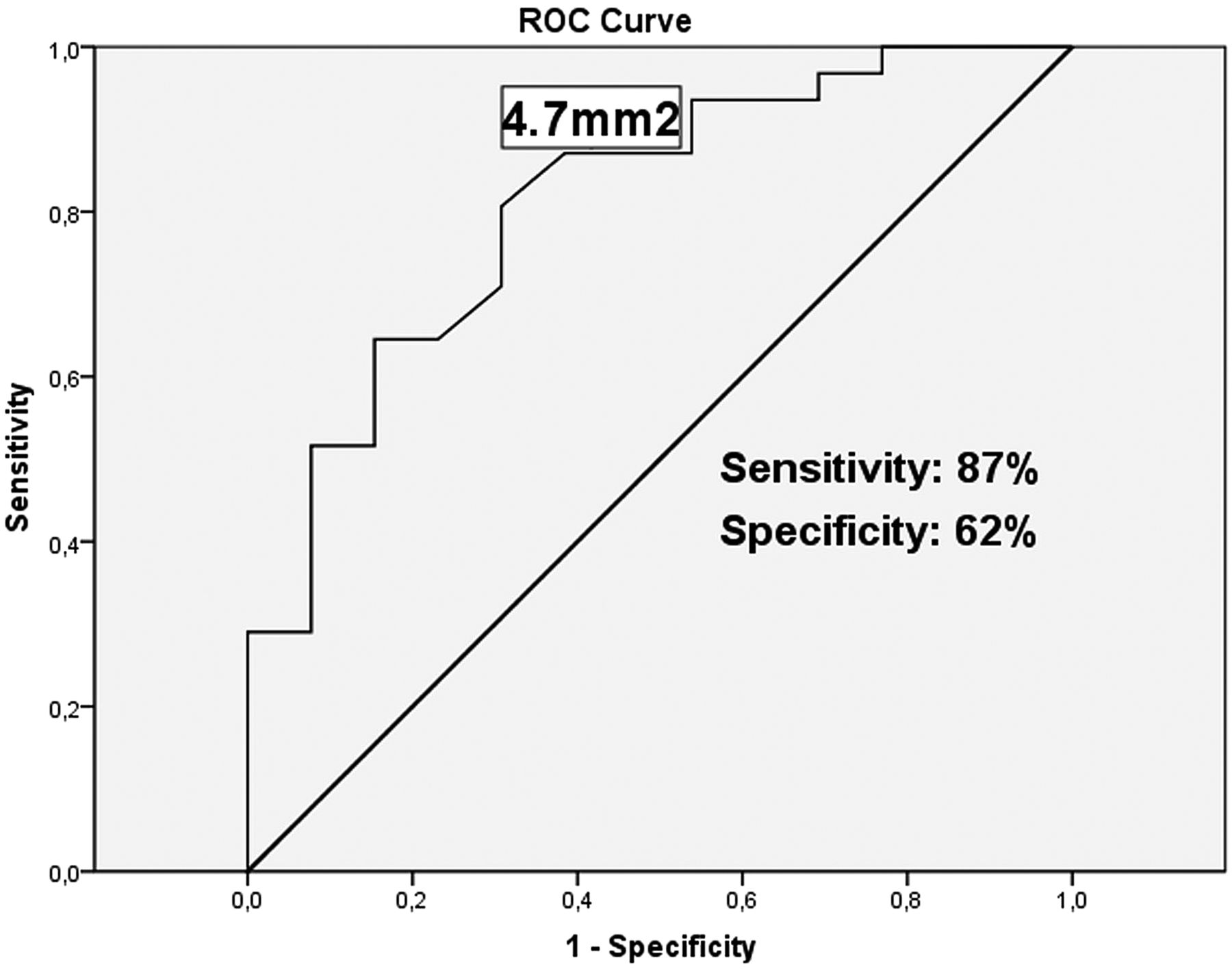
Receiver operating characteristic (ROC) curve for minimum luminal area assessed by multislice CT for detection of significant restenosis defined as minimum luminal area <6 mm2 assessed by intravascular ultrasound. An area under the curve of 0.811 was obtained with a cut-off point of 4.7 mm2.

(A) Multislice CT (MSCT) image of a patent stent in the left main coronary artery with no in-stent restenosis. (B) Cross-section MSCT image. (C) Cross-section intravascular ultrasound (IVUS) image. (D) Longitudinal IVUS image of the same patent stent.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
(A) Multislice CT (MSCT) image of a left main coronary artery stent with in-stent restenosis. (B) Cross-section MSCT image. (C) Cross-section intravascular ultrasound (IVUS) image. (D) Longitudinal IVUS image of the same stent.
Discussion
The main results of the present study are: (1) agreement between quantitative angiography, MSCT and IVUS is good when assessing LMCA in-stent MLD and MLA; (2) MSCT systematically underestimates the LMCA in-stent MLD and MLA compared to IVUS; (3) the MSCT derived MLA cut-off value of 4.7 mm2 seems to be the most appropriate threshold to assess stent patency at 12 months follow-up.
Sixty-four row CT allows a spatial resolution of 350–400 µm, while previous CT generations had a significantly lower resolution. IVUS catheters allow a spatial resolution of around 100–150 µm. For this reason, current guidelines suggest that non-invasive study of stents should be performed with at least a 64 channel MSCT.24 Previous studies evaluating LMCA stent patency with MSCT were performed with 16 row CT and a combination of 16 and 64 row CT.16 ,17 This study is the first to analyse LMCA stents with a 64 row MSCT.
The present study shows an underestimation trend of MSCT for in-stent measures quantified around 0.4 mm in MLD and around 2 mm2 in MLA compared to IVUS. The underestimation trend of MSCT could be explained by the blooming artefact of metallic struts. Metallic struts hamper detection of the lumen contour and may partially hide the neointimal tissue between the artefact. A previous publication comparing in-stent measures between MSCT and IVUS found that MSCT was able to detect neointimal hyperplasia >1 mm.16 Below 1 mm the blooming artefact did not allow an appropriate measurement. In addition, a good agreement between quantitative coronary angiography and MSCT measurements was observed (with a slight non-significant underestimation trend), a point that strengthens our results and supports MSCT as a good non-invasive technique for LMCA stent examinations.
Furthermore, we found a cut-off point of 4.7 mm2 on MSCT derived MLA to assess in-stent restenosis. This cut-off has been correlated with the 6 mm2 threshold assessed by IVUS.
It is important to note that flow fractional reserve could have been a good standard to compare with; however, we have performed the comparison with IVUS due to recent growing evidence in regard to this scenario.23
A recently published study23 has clinically validated this IVUS derived MLA in LMCA, showing that patients with an MLA above this point have an excellent clinical prognosis. Moreover, the 6 mm2 value was obtained from Murray's law (considering an MLA of 4 mm2 as the ischaemic threshold of the branches),23 and has been supported by a study that used IVUS and pressure wire flow fractional reserve.25 The difference between 4.7 mm2 and 6 mm2 is explained by the underestimation produced by the blooming artefact, which is also reflected by the modest absolute ICC obtained between these two techniques. Therefore, the MSCT cut-off may have important clinical implications.
Patients with LMCA stenosis treated with a single stent technique, without severe coronary artery calcification and nominal stent diameter >3 mm, are suitable for a non-invasive follow-up to rule out in-stent restenosis. In those patients it is reasonable to use the 4.7 mm2 threshold for a non-invasive follow-up, avoiding the invasive test suggested by the current guidelines.13
The usefulness of non-invasive testing for the evaluation of LMCA stenosis treated with a double stent technique is still uncertain; therefore, this technique cannot be recommended as routine practice in this setting. The double layer of struts produces an excessive metallic artefact that does not allow for a proper analysis of the lumen. In fact, we report three false positive cases and no false negative cases. It is remarkable that all misclassified cases were patients treated with complex double stent techniques (Crush stent technique and T stent technique). All patients treated with one stent were correctly diagnosed.
Study limitations
The first limitation of the present study is the low incidence of in-stent restenosis, which may have an important influence on the relatively low positive predictive value.
The second limitation is the exclusion criteria. Patients with atrial fibrillation, which is not a rare phenomenon in individuals with cardiac disease, were excluded from this study, thus preventing conclusions to be drawn about an important group of patients who may benefit from this technique in the future.
Finally, it is well known that different types of stents have different blooming artefacts by MSCT.19 The present study used different types of metallic platforms, strut thickness and alloys; therefore, the suggested cut-off to assess in-stent restenosis by MSCT may slightly change according to the stent type.
Conclusions
MSCT is an adequate technique to analyse LMCA stents, showing a good correlation with IVUS, albeit with an underestimation trend due to blooming artefacts observed with MSCT. The present study supports a cut-off of 4.7 mm2 MLA, as assessed by MSCT, which provides an appropriate threshold for the diagnosis of LMCA in-stent restenosis. Non-invasive MSCT imaging can be considered in selected patients with an LMCA stent to assess in-stent restenosis, instead of an invasive imaging technique.
References
Footnotes
-
Contributors GR designed the study, collected the data and drafted the manuscript. JG-L collaborated in designing the study methodology and reviewed all the previous drafts of the manuscript. JLF, JAG-H, and RR collaborated in the data acquisition. LMT and EC collaborated in data interpretation and analysis. EE, FA and AC revised and approved the final draft.
-
Competing interests None.
-
Patient consent Obtained.
-
Provenance and peer review Not commissioned; externally peer reviewed.