Article Text

Abstract
Objective To study trends for 20 years in incidence and 1-year mortality in hospitalised patients who received a diagnosis of either angina or unexplained chest pain (UCP) in Sweden.
Design and setting Register study of all patients aged 25–84 years identified from the Swedish National Hospital Discharge Register who were hospitalised with a first-time diagnosis of UCP or angina pectoris during 1987 to 2006.
Participants A total of 378 454 patients, 235 855 with UCP and 142 599 with angina.
Main outcome measures 1-Year mortality and standardised mortality ratios (SMRs).
Results From the period 1987–1991 to 2002–2006, the observed 1-year mortality rate in men and women with UCP aged 25–74 years decreased from 2.19% to 1.45% and from 1.85% to 0.91%, respectively. SMRs decreased from 1.67 (95% CI 1.39 to 1.95) and 1.63 (1.27 to 2.00) to 1.09 (0.96 to 1.23) and 0.88 (0.75 to 1.00). Corresponding decreases in 1-year mortality for a discharge diagnosis of angina were from 6.50% to 2.49% in men and from 4.80% to 1.68% in women, with SMRs decreasing from 2.69 (2.33–3.05) and 2.59 (2.06–3.12) to 1.09 (0.93–1.25) and 1.05 (0.81–1.29), respectively. Similar changes occurred in patients aged 75–84 years. Only men with UCP aged 75–84 years still retained a slightly increased mortality (SMR 1.14 (1.01–1.28)).
Conclusions The prognosis of patients admitted with chest pain in which acute myocardial infarction has been ruled out has improved for the past 20 years, such that the 1-year mortality of these patients is now similar to that in the general population.
- Myocardial infarction
- angina survival
- mortality
- patients
- population
- acute coronary syndrome
- coronary artery disease (cad)
- epidemiology
Statistics from Altmetric.com
- Myocardial infarction
- angina survival
- mortality
- patients
- population
- acute coronary syndrome
- coronary artery disease (cad)
- epidemiology
Patients with chest pain who are admitted to the hospital with suspected acute coronary syndrome (ACS) comprise a large percentage of all patients attending emergency departments.1 Despite improved diagnostic methods for the past two decades, the evaluation of acute chest pain remains a major challenge to the medical profession. Given the high prevalence of coronary heart disease (CHD) and the still high case-fatality rate associated with ACS, rapid identification of high-risk patients is a major goal of contemporary management. Yet, only a minority of those admitted will have a final diagnosis of acute ischaemia.1–3 At the same time, up to 1 in 20 patients with ACS is not admitted.3 4
The course of patients admitted for chest pain, where acute myocardial infarction (AMI) has been ruled out, is not always benign. One early study of patients with unstable angina showed that one in four either died or had an AMI within 3 years.5 In a recent study from Scotland, patients who received a diagnosis of angina after being admitted to an emergency department had similarly a high age-specific, long-term case-fatality rate as AMI patients (approximately 5% a year).6 In an evaluation of rapid access chest pain clinics in the UK, patients who developed angina had a five times higher risk of ACS or CHD death after 3 years in comparison with patients who developed non-cardiac chest pain. However, one third of subsequent admissions for ACS or CHD deaths occurred in the latter category.7
Outcomes for the past two decades have improved steadily in patients hospitalised with AMI.8–15 Several studies have shown that admissions both for angina and for chest pain have increased, whereas hospitalisations for AMI have decreased.16 17 With the introduction of troponins as more sensitive biomarkers, a new definition for AMI was proposed in September 2000.18 Potentially, this new definition could lead to improved risk stratification, with a decreased risk for patients in whom AMI has been ruled out. Simultaneously, improvement in treatment for patients who developed angina may contribute to decreased mortality for this group. In addition, increased awareness may lead to a lower threshold for admission, with increased admission rates for patients with non-cardiac chest pain. To investigate the potential effect of these changes, we examined incidence rates for emergency admissions with discharge diagnoses of AMI, angina and unexplained chest pain (UCP) for a 20-year period from 1987 to 2006 and trends in 1-year mortality separately for these three diagnoses and then compared them with expected rates for the general population to create age-standardised mortality ratios (SMRs).
Methods
Study sample
Sweden has a publicly financed health system with hospital care available to all citizens at low cost. Swedish hospitals register principal and contributory discharge diagnoses for all patients in the national hospital discharge register. For the purpose of the present study, data from the national hospital discharge and cause-specific death registers were linked through the personal identity number, which is unique for all Swedish citizens. The hospital discharge register has been in operation since the 1960s and has operated on a nationwide basis since 1987. Three separate groups (AMI, n=259 420; angina pectoris, n=142 599; and UCP, n=235 855) were identified and followed up for 1 year regarding all-cause mortality. Only first episodes were included. The International Classification of Diseases, Ninth Revision (ICD-9) was used from 1987 to 1996, whereas the International Classification of Diseases, Tenth Revision (ICD-10) was used from 1997 and onwards. Ischaemic heart disease (IHD) was defined as being discharged with any diagnostic code of 410-414 (ICD-9) or I20–I25 (ICD-10). UCP was defined as being discharged with the diagnostic codes 786F (ICD-9) or R07.2, RO7.3 and R07.4 (ICD-10). The diagnostic codes used for angina pectoris (henceforth termed angina) were 411B, 413 (ICD-9) and I20 (ICD-10), whereas those for AMI were 410 (ICD-9) and 121 (ICD-10). This specification of all first emergency admissions for angina served as a crude proxy for unstable angina. To ensure that data from all years were comparable regarding prior disease, we defined a time frame for a first event as no prior hospitalisation with these diagnoses or any other IHD diagnosis in the last 7 years.
Patients with suspected AMI/ACS in Sweden are generally admitted to a hospital directly through the emergency department, mostly without prior contact with primary care. As a rule, they are first seen by internists and not by cardiologists or emergency physicians. Patients may be admitted to cardiology wards or short-stay internal medicine facilities; there are generally no facilities for managing patients with acute chest pain on an outpatient basis. During the 20-year period of the present study, the number of acute care hospital beds in Sweden has been reduced by more than half (http://www.oecd.org/home/), and Sweden has now the second lowest proportion of acute care hospital beds per 1000 among all Organization for Economic Cooperation and Development countries. With the general shortage of beds, there is no financial or other incitement to admit patients.
Comorbidity was defined as any concomitant diagnosis or as any principal diagnosis in a prior admission within 7 years before and including the index admission, categorised as diabetes (ICD-9 code 250, ICD-10 E10, E11, E14), hypertension (401–405; I10–I15), stroke (430–438, I60–I69), valvular disease (393–398; 424, I05–I09, I34–I35), atrial fibrillation (427D, I48), cardiomyopathy (425, I42), pulmonary embolism (415B, I26), chronic obstructive lung disease (490–496, J44), asthma (493, J45) and cancer (140–239, C00–D48). Coronary procedures (coronary angiography, percutaneous coronary intervention (PCI) and coronary artery bypass graft (CABG)) were recorded up to 30 days after the index admission. Data for these procedures were only available after 1996.
In the final dataset, all personal identifiers were removed and replaced with a code.
Statistical analysis
All analyses were carried out using SAS v.9.1 and R statistical computing system v.2.9.0. Age-standardised annual incidence rates per 100 000 of first hospitalisations for UCP, angina and AMI were calculated using the direct method with the year 2000 population of Sweden as standard. Means and proportions for continuous and categorical variables were calculated for each period and diagnostic group (UCP and angina) and the significance of trends across periods tested using analysis of variance F tests and Cochran–Armitage tests for trend. Logistic regression was used to calculate mean annual change in 1-year mortality. Observed and expected 1-year mortality rates per 1000 were computed and presented for the three patient categories during the period 1987–2006, divided into four 5-year periods (1987–1991, 1992–1996, 1997–2001 and 2002–2006). The expected 1-year mortality rate is based on the age-, sex- and calendar year–specific death rates of the national population (Human Mortality Database, University of California, Berkeley, California (USA) and Max Planck Institute for Demographic Research (Germany), available at http://www.mortality.org).
Results
Trends in incidence rates for discharge diagnoses of chest pain, angina and AMI
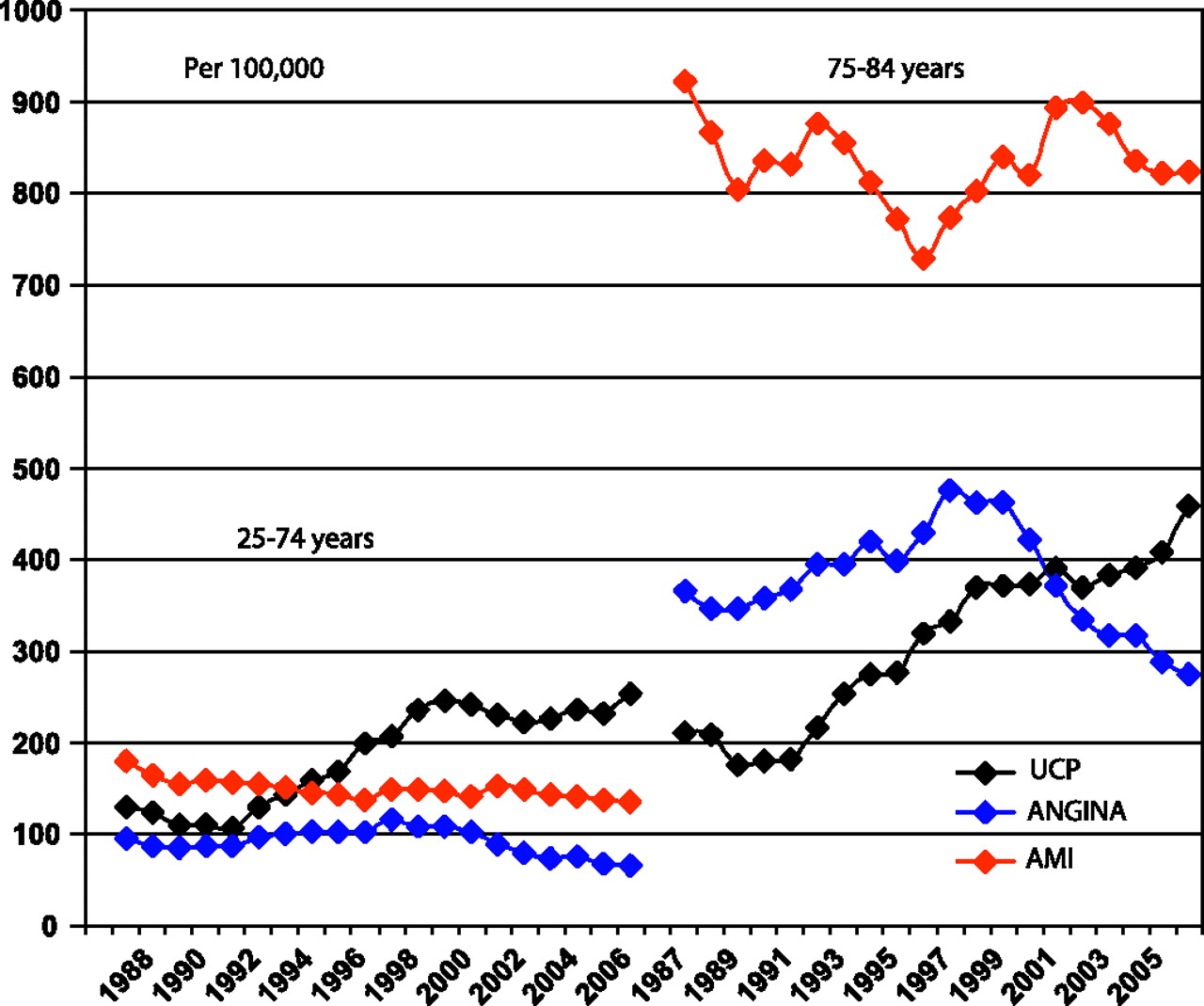
Trends in age- and sex-standardised hospitalisation rates for UCP, angina and AMI for the period 1987 to 2006 are shown in figure 1. In patients aged 25–74 years, UCP increased from the early 1990s and then stabilised during the last years of the study period. In contrast, rates for angina and AMI changed little. In patients aged 75–84 years, AMI rates decreased until 1998, with a marked increase taking place after 1998, which was mirrored in a decrease in angina, potentially reflecting a shift in diagnostic patterns with patients with minor myocardial necrosis moving from angina to an AMI diagnosis. Discharges with UCP increased throughout the period. If a first discharge for any of these diagnoses was considered, the number of patients with AMI or angina was comparatively stable, whereas there was a continuous increase in discharges for chest pain and, accordingly, an increase in the absolute number of patients with suspected ACS (figure 2). However, in the new millennium, there has been no further increase.

Trends in age-standardised incidence rate from 1987 to 2006 per 100 000 by age group and diagnosis.
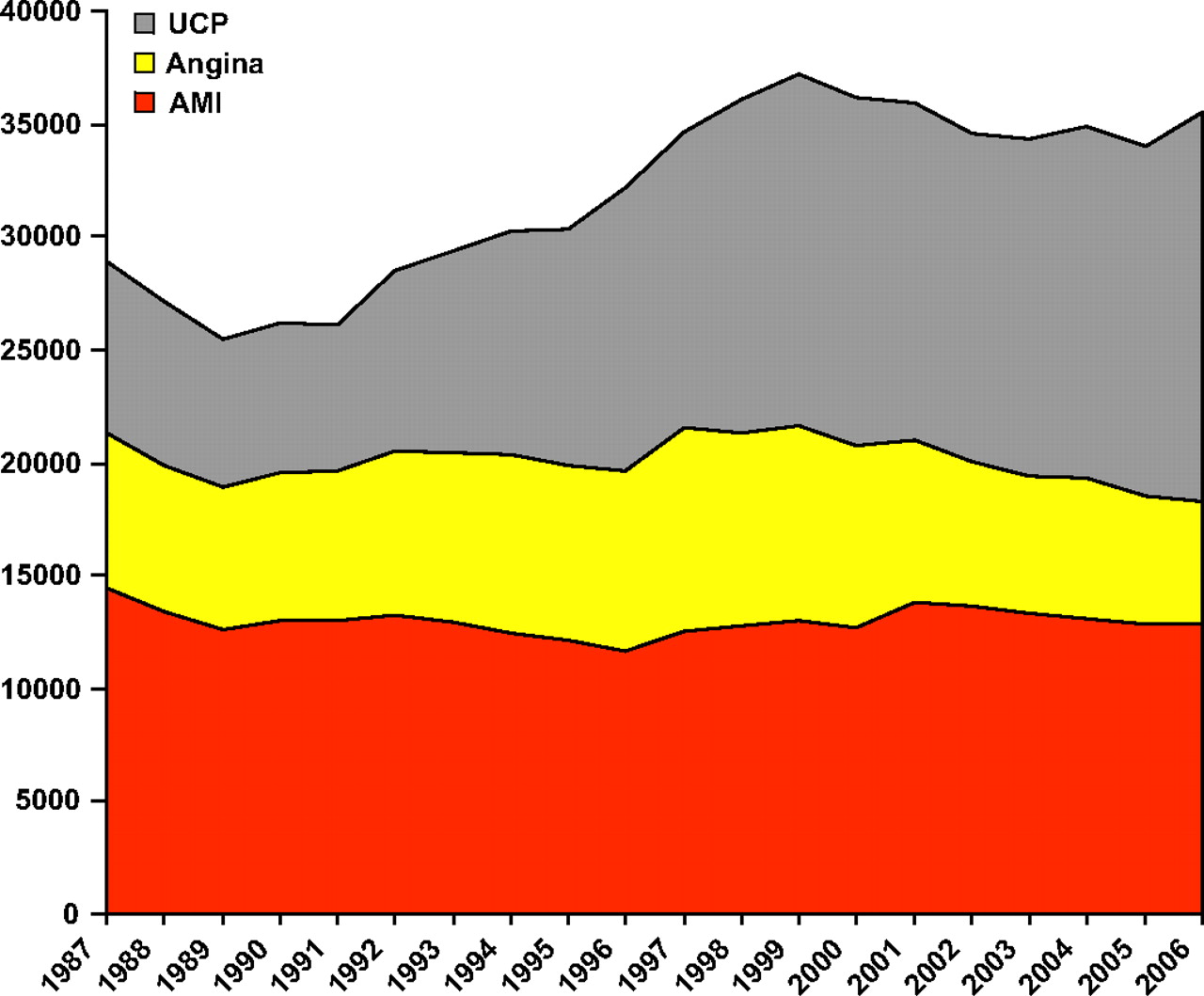
Trends from 1987 to 2006 in the number of discharges for AMI, angina and UCP.
Trends in patient characteristics
Table 1 shows how characteristics of patients discharged with UCP or angina changed over time. Mean age in UCP patients increased slightly from 58.0 to 58.5 years, with the proportion of women increasing from 42.1% in the first period to 50.8% in the last period. Mean (SD) length of hospital stay decreased significantly from 2.4 (2.6) to 1.3 (1.4) days (p<0.0001). The prevalence of coexisting illnesses was low, reflecting the relatively young age of the patient group and the exclusion of patients with prior hospitalisation for IHD. The proportion of patients with a concomitant diagnosis of hypertension, diabetes or atrial fibrillation increased over time (all p<0.0001). Even in the last period (2002 to 2006), few patients with UCP (4.5%) underwent a coronary angiography; in a small number of patients (<1%), the UCP diagnosis was obviously incorrect, as indicated by the need for revascularisation within 30 days.
Trends over time from 1987 to 2006 in patient characteristics with UCP or angina
The angina patients were almost a decade older (mean age 67.1 to 67.6 years) and with fewer women (just above 40%) than the UCP group. Mean (SD) length of hospital stay decreased significantly from 4.3 (4.3) to 3.5 (4.3) days (p<0.0001). In 2002 to 2006, 42.2% of the angina patients underwent coronary angiography within 30 days from admission, 24.1% had a PCI and 11.1% underwent CABG.
Crude 1-year mortality and age-adjusted standard mortality ratio trends
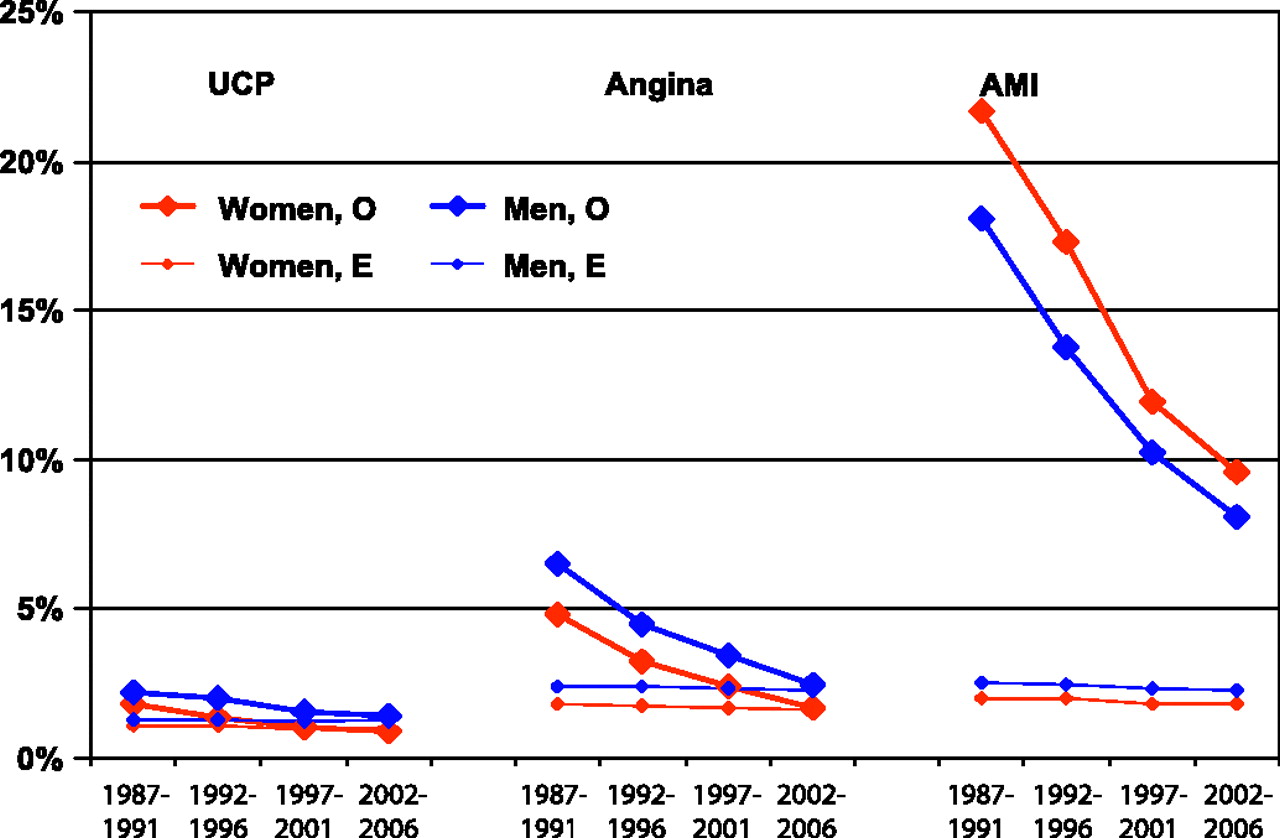
The observed 1-year all-cause mortality rates decreased for the 20-year period for all age, sex and discharge diagnosis categories (figure 3 and 4, table 2). One-year prognosis was considerably worse for patients discharged with AMI than for either angina or UCP. For men aged 25–74 years and a discharge diagnosis of UCP, the crude 1-year mortality decreased from 2.19% to 1.45% and the age-adjusted SMR from 1.67 (95% confidence interval (CI) 1.39 to 1.95) to 1.09 (95% CI 0.96 to 1.23). Corresponding figures for women aged 25–74 years were 1.85% and 0.91% with a decrease in age-adjusted SMR from 1.63 (95% CI 1.27 to 2.00) to 0.88 (95% CI 0.75 to 1.00). The age-adjusted decrease per year for men aged 25–74 years was 3.0% (95% CI 2.3 to 3.8%) and for women 3.9% (95% CI 2.9 to 5.0%). One-year mortality in men aged 75 to 84 years with UCP was much higher than that in younger men, reflecting the high background mortality for men in this age category. The trends in SMR were very similar to those for younger men, however, with an SMR for the last period of 1.14 (95% CI 1.01 to 1.28), indicating a persisting, slightly elevated mortality compared with that in the general population. Women aged 75 to 84 years with UCP had a lower 1-year mortality than the men and did not have a higher mortality at any time than expected; indeed, after 1997, they had a significantly lower mortality.

One-year mortality (percentage; observed (O) vs expected (E)) in UCP (left), angina (middle) and AMI (right) from 1987 to 2006 in men and women aged 25 to 74 years.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
One-year mortality (percentage; observed (O) versus expected (E)) in UCP (left), angina (middle) and AMI (right) from 1987 to 2006 in men and women aged 75 to 84 years.
Trends in 1-year mortality in patients with UCP or angina from 1987 to 2006 by gender and age
Mortality after a discharge diagnosis for angina was higher than that for chest pain for all sex-age categories, particularly for men and during the first 5-year period. However, mortality also decreased at a steeper rate, from 6.50% to 2.49% in men aged 25 to 74 years and from 4.80% to 1.68% in women of the same age group. The age-adjusted decrease rates per year were 6.0% (95% CI 5.4 to 6.7%) and 5.9% (95% CI 4.8 to 7.0%) for men and women, respectively. SMRs decreased from 2.69 to 1.09 (95% CI 0.93 to 1.25) in men and from 2.59 to 1.05 (95% CI 0.81 to 1.29) in women. For men and women aged 75 to 84 years, 1-year mortality rates in 1987 to 1991 were 19.21% and 12.28%, respectively, decreasing to 9.63% (men) and 7.26% (women), with SMRs not significantly different from that of the general population in 2002 to 2006.
Discussion
Our study confirms the improved prognosis in patients with AMI while adding that patients in whom AMI has been ruled out, although at a much lower mortality risk than that in AMI patients, have a markedly lower 1-year case-fatality rate as compared with 20 years ago, despite decreasing length of stay and comparatively few invasive procedures. Only men aged 75 to 84 years who were discharged with a UCP diagnosis still have a slightly higher risk than the age-matched male population. With this single exception, in patients with a diagnosis of angina or considered to have unspecified chest pain, 1-year mortality is now no higher than that of the general age-matched population.
Comparison with other studies
In a study of 2271 Olmsted residents presenting with unstable angina between 1988 and 1992, 22% of the men (mean age 60 years) and 29% of the women (mean age 67 years) died during a 6-year follow-up, although prognosis varied widely across prespecified risk categories.19 A Scottish study6 found that after exclusion of deaths within 30 days, 1-year crude case-fatality rates in men and women discharged with a diagnosis of angina in 1990 to 2000 were 6.5% and 6.4%, respectively. Considering that this estimate did not include deaths occurring in the first 30 days, this 1-year crude case–fatality rate is slightly higher than the 1-year mortality rates for our total sample of men and women aged 25 to 84 years, which were 6.5% and 5.2% for the periods 1992–1996 and 1996–2001, respectively.
Few studies have compared survival in patients with angina to that of the general population. In the study by Capewell et al,6 the 5-year case-fatality rate for angina in men was 25.8%, with the expected 5-year mortality for a 64-year-old man in Scotland (mean age of the angina group) 15.3%. Likewise, the 5-year mortality in women in the general population was lower (13.2%) than that of patients with angina (25.2%). Accordingly, estimates for relative mortality for angina would be approximately 1.5 to 2 or not very different from the SMRs for 1-year mortality for the corresponding periods in our sample. A subset of angina patients with high-risk features from the Olmsted study had 3-year mortality rates of 25% (men) and 32% (women), which can be compared with expected mortality rates of 12% (men) and 14% (women).19 However, low-risk patients did not have an elevated mortality risk.
Although stable angina pectoris should not be confused with unstable angina, it is noteworthy that we previously found a relative risk of 1.63 for long-term risk of death in middle-aged men with angina pectoris diagnosed in the 1970s relative to men without angina,20 which was lower than the threefold increased risk of death identified for AMI. Similar relative risks for angina were observed in the long-term follow-up of the Reykjavik study.21 A recent study from Ireland found that mortality and cardiac outcomes for primary care patients with angina pectoris alone were similar to those with previous AMI, revascularisation or both.22
In the study by Capewell et al,6 longer-term case-fatality rate was almost as high for angina as for AMI, approximately 5% per year, after exclusion of initial deaths. Obviously, chest pain patients and patients with unstable angina have widely varying risk. One of the most important factors is age. In the present study, although expected annual mortality for the patients aged 25 to 74 years with chest pain was between 1.0% and 1.4% and for those with angina (who were on average 9 years older) between 1.6% and 2.4%, expected mortality in the age band 75 to 84 years was 8% to 10% for the general population. Accordingly, age is of vital importance when comparing case-fatality rates between studies.
Not many studies have evaluated patients with non-specific chest pain. An early cohort study found that men with chest pain not considered to be ischaemic in origin had significantly increased long-term mortality.23 In the Women's Health Initiative Observational study, women admitted at least overnight with non-specific chest pain had more cardiovascular events, but not increased mortality, compared with other women.24 In a recent analysis of patients attending a rapid-assessment chest pain clinic, those considered to be at low risk (based on clinical features and an exercise electrocardiogram (ECG) in most) had a coronary mortality of about half of that expected.25
It is quite clear that making a comparison over an extended period of patients hospitalised for any specific diagnosis is difficult in the sense that the patient groups registered in different periods are not comparable. For example, in the Atherosclerosis Risk in Communities study, with strict criteria for definite or probable AMI, the proportion of incident MI cases with major ECG abnormalities decreased over time.26 A similar decline in the severity of AMI was observed in the Olmsted study.27 A recent publication from a Framingham sample of 9824 men and women showed that AMI incidence, based on ECG criteria alone and thus likely representing a more severe form of AMI, declined by 50% over with a concomitant twofold increase in rates of AMI diagnosed with the aid of markers.28 The case-fatality rates after AMI declined by 50% to 75% from 1960 to 1999, irrespective of which criteria were used. From this finding, it may be concluded that not only that MI trend data may be biased by a diagnostic drift resulting from the advent of diagnostic biomarker tests for AMI but also that decrease in case-fatality rate is probably not dependent on the criteria used. It would be difficult to apply similar severity criteria for angina and impossible to do so for UCP. An increase in the number of patients admitted for suspected ACS has been documented not only in Sweden,17 although media campaigns aimed at reducing delay times in AMI seem not to have had any lasting impact on the number of patients admitted.29 Accordingly, it will have to be accepted that no like-for-like comparison can be attempted for the present study. The improvement in survival will therefore reflect not only differences in management but also differences in the composition of the groups admitted during various periods. In patients with UCP, changes in patient selection is the most likely explanation because there is little evidence of increasing availability of effective treatments for these patients.
Sex differences
Our findings further revealed that in patients aged 25 to 74 years, a larger percentage of patients who developed coronary disease (either AMI or angina) were men, whereas almost half the patients with UCP in this same age group were women. Given the higher prevalence of coronary disease in men in this age group, this finding is not unexpected, but it is not known whether it represents an underdiagnosis of women with coronary disease. Even so, the short-term prognosis in this group was not seriously impaired, with a much lower 1-year mortality rate compared with that in the other diagnostic groups, implying that a potential misdiagnosis of CHD in women did not lead to an impaired short-term prognosis. The higher absolute risk of AMI and CHD death in men, compared with women,30 probably explains the poorer prognosis in men.
Potential explanations for the findings of the study
Although the reasons for the improvement in prognosis for these categories are probably multifactorial, they can be divided into three potential groups. First, lower thresholds for admission, as evidenced by the marked increase of hospitalisations for chest pain, particularly during the early part of the 20-year observation period, will have led to inclusion of milder cases. Second, the probable use of evidence-based medications and other procedures may have played a role, particularly for the angina group, where case-fatality rate improved more than for the chest pain group. Third, the introduction of routine troponin measurements and changing the criteria for myocardial infarction in the year 2000, the full impact of that would have been evident during the last 5 years of the study, will have contributed to remove a subsample of high-risk patients from the angina (and possibly from the chest pain) group to the AMI group. Most UCP patients were managed without invasive diagnostic methods; even in the last period, less than 1 in 20 underwent coronary angiography. However, a small proportion (<1%) were revascularised within 30 days, indicating that the UCP diagnosis was erroneous in these cases.
Strengths and limitations
The main strength of our study was the completeness of data, with a nationwide unselected cohort of patients, with a large number of events that allowed detailed analyses by diagnosis, period, sex and age group. Even so, these data were collected for administrative rather than research purposes. With the exception of revascularisation procedures, there was no information about changes in admission thresholds and therapies during hospital admission and no detailed data on diagnostic procedures. Given that this is a routine dataset with a lack of hard clinical data (eg, troponin levels and extent of investigations including exercise testing), the potential for systematic coding bias and misleading trends is not insubstantial. However, even with these limitations in mind, our findings suggest substantial improvement in persons admitted for suspected ACS with current management of low thresholds for admission, the widespread use of sensitive markers and, probably, use of medication in patients discharged with an angina diagnosis.
Conclusions
Between 1987 and 2006, the SMRs for patients admitted with suspected ACS and discharged with a diagnosis of either unspecified chest pain or angina decreased considerably. Our study confirms the improved prognosis in patients with AMI while adding that patients where AMI has been ruled out, although at much lower mortality risk than AMI patients, now have a markedly lower risk than they had 20 years ago. Both in patients who receive a diagnosis of angina and patients considered to have UCP, 1-year mortality is today similar to that of the general age-matched population. An important next step would be to develop better strategies to avoid unnecessary hospitalisations.
References
Footnotes
Funding the Swedish Research Council, the Swedish Council for Working Life and Social Research and the Swedish Heart and Lung Foundation.
Competing interest None.
Ethics approval This study was conducted with the approval of the ethics committee at the University of Gothenburg (study code 148-07).
Provenance and peer review Not commissioned; externally peer reviewed.