Article Text

Abstract
Objectives To examine the contribution of exercise echocardiography (ExE) to the diagnosis of heart failure with preserved ejection fraction (HFpEF).
Design Cross-sectional study of patients undergoing ExE.
Patients 436 patients with fatigue or dyspnoea presenting for ExE were studied.
Methods Current criteria for the diagnosis of HFpEF (evidence of symptoms or signs of heart failure, EF>50%, abnormal transmitral flow and supplementary tissue Doppler measurements (E/e′) suggesting raised left ventricular filling pressure) were applied to this population. The impact of reclassification of clinical status based on exercise E/e′ >13 and ischaemia was evaluated.
Results Of 436 patients, 37 had E/e′ >15 and 111 had E/e′ 8–15, with supplementary echocardiography criteria indicating HFpEF (n=148). Only 36 patients fulfilling the diagnosis of HFpEF had reduced exercise capacity. Fifteen of these patients had evidence of raised E/e′ with exercise, half (7) of whom had inducible myocardial ischaemia. Of 13 patients with raised filling pressure at rest or exercise, objective exercise intolerance and no ischaemia, five did not reach the current criteria for HFpEF.
Conclusion The current classification for HFpEF may include patients with preserved functional status and many with ischaemia and normal exercise E/e′. Reduced exercise capacity, increase of E/e′ with exercise and ischaemia are three objective aspects of the HFpEF syndrome that might be considered for incorporation in the definition.
- Heart failure with preserved ejection fraction (HFpEF)
- exercise
- ischaemia
- diastolic dysfunction
- echocardiography-exercise
Statistics from Altmetric.com
- Heart failure with preserved ejection fraction (HFpEF)
- exercise
- ischaemia
- diastolic dysfunction
- echocardiography-exercise
The ratio of transmitral passive filling velocity (E) and annular tissue velocity (e′) at rest reflects left ventricular (LV) filling pressure,1 2 is a predictor of outcome3 and has a central role in the recognition of heart failure with preserved ejection fraction (HFpEF).4 However, resting E/e′ may be insufficiently sensitive to identify patients with early HFpEF, in whom symptoms appear and filling pressure increases only on exertion.5 In addition, exercise intolerance with increased resting E/e′ may be insufficiently specific because dyspnoea may be an angina-equivalent.6
Exercise echocardiography (ExE) offers several important pieces of information that might clarify the diagnosis of HFpEF. First, the current guidelines stipulate the presence of symptoms of heart failure, but awareness and perception of dyspnoea may be an important source of variation in these patients,7 to which objective evidence of exercise capacity may be a useful adjunct.8 9 Second, the acquisition of exercise E/e′ permits the detection of increased filling pressure with exercise.10 As the attribution of exercise intolerance to heart failure is difficult to sustain in the absence of raised LV diastolic pressure (LVDP), the absence of this finding might suggest another explanation for dyspnoea. Conversely, the recognition of ischaemia may present both an alternative explanation to HFpEF, as well as different therapeutic targets. This study sought to examine the implications of exercise capacity, E/e′ and ischaemia for the current criteria for HFpEF.
Patients and methods
Patient selection
We studied 531 consecutive patients referred for ExE for investigation of fatigue or dyspnoea from 1555 patients presenting for ExE between January 2005 and December 2008. Patients with LV dysfunction (EF <50%; n=43) and those with worse than mild valvular heart disease (n=27) were excluded. Patients in whom E/e′ was not measurable, either at rest or exercise (n=25), were also excluded from the data analysis, leaving a study population of 436 consecutive patients. Clinical characteristics of the study population are presented in table 1. The study was approved by the hospital research ethics committee and patients gave written informed consent.
Clinical characteristics
Resting echocardiography
Imaging was performed by experienced sonographers using a standard echocardiography machine (ie, 33 or Philips 7500, Philips, Andover, Massachusetts, USA) with a 3.5 MHz transducer. Images from standard parasternal and apical views were digitally recorded for offline analysis.
Early (E) and late (A) diastolic mitral inflow velocities were measured from the transmitral flow profile, recorded in the apical four-chamber view with the sample volume placed at the level of the mitral valve leaflets in diastole. Systolic (s'), early (e′) and late (a') diastolic tissue velocity was also measured in the apical four-chamber view by pulsed wave tissue Doppler of the septal mitral annulus. Mean LVDP was estimated by the ratio of E/e′, calculated by the average of three cardiac cycles at rest and exercise. Left atrial area (LAA) and volume index (area–length method) were measured in the apical two- or four-chamber view and LV mass index (LVMI) was measuredby standard criteria.11 Diastolic dysfunction was classified as normal, impaired relaxation, pseudonormal filling or restrictive filling. Impaired relaxation was determined by deceleration time (DT) >2SD of age-dependent normal values. Pseudonormal filling was identified by normal DT, and E/e′ >15 or E/e′=8–15 in the presence of left atrial (LA) enlargement. A restrictive filling pattern was identified by DT <140 ms.
Exercise echocardiography
Patients exercised using standard symptom-limited treadmill protocols with 12-lead ECG monitoring. Cine loops from the parasternal and apical views were acquired before and immediately after symptom-limited treadmill exercise and stored digitally. Transmitral flow and tissue Doppler was measured after acquisition of these loops.10 Conventional 16-segment analysis was used by two experienced observers to measure wall motion scores for the detection of inducible ischaemia.11 Segments were scored as normal (1), hypokinetic (2.0), severely hypokinetic (2.5), akinetic (3) or dyskinetic (4), with the average of these segments determining the wall motion score index. Ischaemia was identified by an experienced reader where new and inducible wall motion abnormalities were seen in one or more segments.10 Diastology was assessed by two experienced observers, with exercise E/e′ >13 signifying raised LVDP (>15 mm Hg).10 A hypertensive blood pressure response to exercise was denoted as brachial blood pressure >210/105 for men and >190/105 for women.
HFpEF classification
The current European Society of Cardiology guidelines for the diagnosis of HFpEF4 were used to identify patients who fitted the criteria of HFpEF (approach 1). Supplementary approaches were devised to classify patients with the addition of exercise capacity (approach 2), exercise E/e′ (approach 3) and inducible ischaemia (approach 4). Finally, a combined approach (approach 5) considering exercise capacity, exercise E/e′ and inducible ischaemia was developed to further classify patients with suspected HFpEF. All patients had preserved EF >50% and symptoms of dyspnoea or fatigue, which were considered indicative of congestive heart failure in the outpatient setting.4
Patients underwent objective assessment of exercise intolerance to identify functional impairment (approach 2), identified if treadmill metabolic equivalents (METs) were less than published age and sex-specific normal values.8 9 According to the European guidelines,4 patients with symptoms of fatigue or dyspnoea with resting E/e′>15 were classified as HFpEF. In patients with non-conclusive E/e′ (8–15), further echocardiographic assessment was made on the basis of atrial fibrillation, LA size (LA volume index >40 ml/m2 or LAA >20 cm2 if LA volume was unobtainable),11 12 LVMI >122 g/m2 (men) or >149 g/m2 (women) or E/A ratio <0.5 and deceleration time >280 ms. Patients with raised LV filling pressure (approach 3) were defined by elevation at either rest (E/e′ >15 or 8–15 with supplementary features) or with exercise E/e′ (>13).10 Ischaemia at ExE was also used to identify potentially treatable symptoms in patients otherwise classified as HFpEF (approach 4).11
Statistical analysis
Comparisons of continuous and categorical variables were analysed by t test and by χ2, respectively. Associations between continuous variables were assessed by Pearson's correlation coefficient, whereas categorical variables were assessed by Spearman's rs. Comparisons across multiple groups were made with Bonferroni-corrected analysis of variance. A subset of 20 randomly selected patients were re-measured to define reproducibility within and between observers, and expressed by the Bland–Altman and intraclass correlation methods. All data were analysed using standard statistical software (SPSS version 17) with p<0.05 considered significant.
Results
Table 1 summarises the clinical details of 436 patients with symptoms of fatigue or dyspnoea in the outpatient setting who underwent ExE between January 2005 and December 2008.
Approach 1: Current criteria
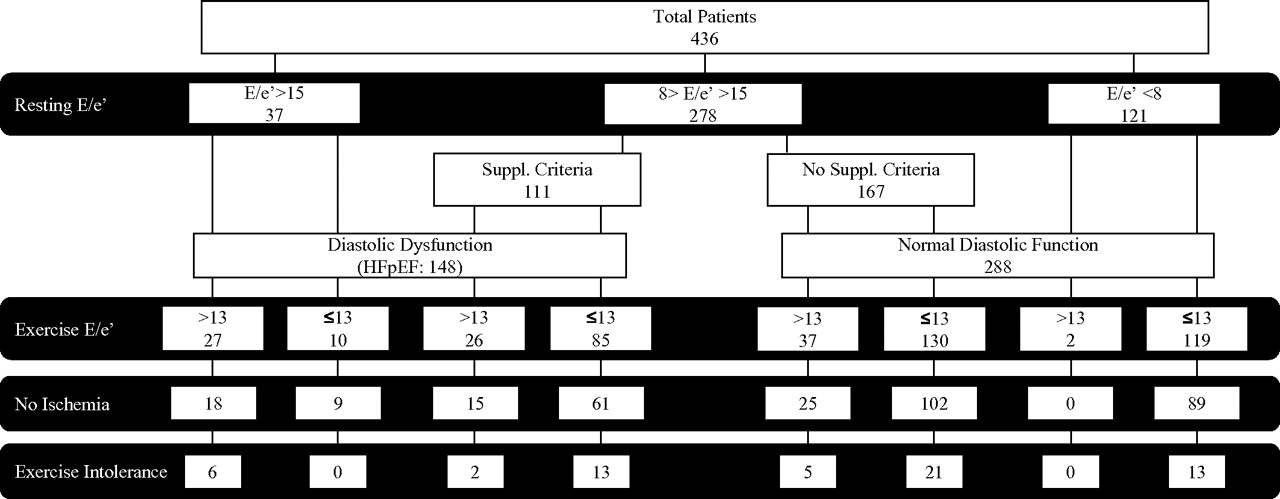
Of 436 patients, 148 fulfilled the criteria for HFpEF (figure 1).

{kind=link}
Combined criteria for heart failure with preserved ejection fraction (HFpEF). Flow chart categorising patients based on current criteria for HFpEF with consideration of exercise capacity, exercise E/e′ and inducible ischaemia.
Approach 2: Exercise testing
Only 36 (24%) of the 148 patients with suspected HFpEF showed objective evidence of exercise limitation (figure 1). Patients with raised E/e′ at rest had a lower exercise capacity than the remainder (8.3±2.5 vs 10.3±3.1 METs; p<0.001) and increased exercise E/e′ was associated with lower workload (8.7±2.7 vs 10.4±3.1 METs; p<0.001).
Approach 3: Exercise echocardiography
Of 37 patients fulfilling the criteria for HFpEF with resting E/e′ >15, ExE showed raised exercise E/e′ (>13) in 27 (73%; figure 1). In 111 patients with non-conclusive resting E/e′ and supplementary criteria, 26 (23%) had raised E/e′ with exercise. Therefore, from 148 patients with suspected HFpEF by the current criteria, 63 had evidence of raised E/e′ either at rest or with exercise and with consideration of exercise E/e′, were classified as HFpEF. An additional 37 patients with non-conclusive E/e′ did not meet the supplementary criteria, yet displayed evidence of raised LV filling pressure with exercise, and were therefore reclassified as HFpEF. Only two patients (1.5%) with no tissue Doppler evidence of diastolic dysfunction (DD) at rest developed raised exercise E/e′. Resting and exercise E/e′ was correlated with age, METs, heart rate (rest and peak) and baseline blood pressure (table 2). Among patients with raised exercise E/e′, resting E/e′ correlated with exercise capacity and heart rate (rest and peak).
Correlates of the E/e′ response to exercise
Fifteen patients (two men, 13 women) had elevated exercise E/e′ and a hypertensive blood pressure response to exercise, whereas the majority of patients had neither (n=310). The proportion of patients with an exercise E/e′ >13 was similar between those with and without a hypertensive blood pressure response (table 3).
Association between raised exercise E/e′ and a hypertensive response to exercise
Approach 4: Ischaemia
Inducible myocardial ischaemia was identified in 117 patients (27%), among whom the average wall motion score index was 1.11±0.20 at rest and 1.55±0.34 with exercise. Eleven of these 117 patients had a hypertensive response to exercise, which may have contributed to the inducible wall motion abnormality. One-third of patients with suspected HFpEF had inducible ischaemia on ExE (figure 1). The proportion of patients with ischaemia was similar between patients with resting E/e′ >15 and those with E/e′ 8–15 and those with resting E/e′ <8 (p=NS for all). Inducible ischaemia was associated with age (Spearman's rs=0.19; p<0.001), male gender (rs=0.19; p<0.001), METs (rs=−0.13; p<0.009) and previous myocardial infarction (rs=0.21; p=0.001).
Approach 5: Combined criteria for HFpEF
After consideration of exercise E/e′, only 102 patients from the original study population (n=436) had evidence of raised filling pressure either at rest or exercise (Figure 1). When patients with evidence of inducible ischaemia were excluded, the number of patients with suspected HFpEF decreased to 67. After consideration of exercise E/e′, ischaemia and exercise capacity, there were 13 patients from 436 fitting the refined categorisation of HFpEF. There was no difference in use of drugs between patients with HFpEF by the current criteria and those with consideration of this combined approach (p>0.05 for all; table 1).
Reproducibility
Intraobserver variability of E/e′ was low, with small mean differences and high intraclass correlations (ICCs) at rest (0.0±0.3; ICC=0.996, p<0.001) and exercise (0.0±0.3; ICC=0.975, p<0.001), although there was less intraobserver variation for resting E/e′ (p=0.001 for z score between ICCs). Interobserver variability was also low, with small mean difference between observers at rest (−0.2±1.1) and exercise (0.1±1.3). The interobserver ICC for resting E/e′ was 0.953 (p<0.001), which was significantly higher than the ICC for exercise E/e′ (ICC=0.873; p<0.001; p=0.04 for z score between ICCs).
Discussion
The use of non-invasive estimation of LVDP by the E/e′ ratio has been proposed as key criterion in the classification of HFpEF. The results of this study show that patients classified in this way would be quite different if HFpEF were identified as present in patients with increased E/e′ at rest or stress, in the presence of reduced exercise capacity and the absence of ischaemia.
Measurement of exercise capacity
Primary symptoms of HFpEF include dyspnoea and fatigue, leading to a reduction of exercise capacity. However, only one-quarter of patients with suspected HFpEF in this study had objective evidence of exercise intolerance. In patients with HF, there is a poor relationship between perceived exercise tolerance and objective measures of circulatory, ventilatory or metabolic abnormalities during exercise.7 An objective measure of exercise capacity is therefore important in determining functional status in patients with HFpEF. Although the HFpEF criteria stipulate objective evidence of DD as part of the diagnostic criteria, many patients with DD are asymptomatic at rest,13 14 and become breathless only on exertion when LV filling pressures are elevated.15 Exercise testing, and in particular ExE, is therefore a valuable tool with potential for identifying patients with impairment of functional capacity and raised LV filling pressure.
Role of LV filling pressure in HFpEF
HFpEF is associated with hypertension,16–18 arterial stiffening,19 20 coronary disease,17 18 diabetes mellitus,18 21 obesity22 or other forms of cardiomyopathy.23 Regardless of aetiology, however, HFpEF is characterised by ventricular stiffening and impaired relaxation, resulting in suboptimal filling and raised LV filling pressure.
Until recently, the diagnosis of HFpEF has been one of exclusion. Recent recommendations for the diagnosis of HFpEF have included the positive identification of DD.4 The identification of raised LV filling pressure with ExE (approach 3) may be a worthwhile addition, because many patients with HFpEF are not symptomatic at rest, but display significant dyspnoea, fatigue and exercise intolerance during stress testing.10 24 Measurement of E/e′ during exercise is feasible,25 and has been invasively validated for the estimation of LVDP,10 26 with E/e′>13 accurately identifying raised LVDP (>15 mm Hg).10 Application of this cut-off point to our population showed that most patients (and all patients with exercise intolerance) with elevated resting E/e′ maintain elevated filling pressure with exercise. In those patients with non-conclusive resting E/e′ (8−15) with supplementary criteria for DD and exercise intolerance, exercise E/e′ was only elevated in three patients (two were free of ischaemia), indicating the poor relationship between exercise intolerance, objective measures of LV filling pressure during exercise and the diagnosis of HFpEF by conventional resting criteria. Despite separate criteria for exclusion of HFpEF in the guidelines, if LVDP is normal during symptom-limited exercise, HFpEF is unlikely.27
Previous work has demonstrated the importance of dyspnoea in patients with and without known coronary artery disease.6 Owing to the subjective nature of reporting dyspnoea, the origin of dyspnoea in patients with alleged HFpEF may be determined more accurately by ExE.28 The current findings support the relationship between DD and exercise capacity.5 10 29 30
Role of ischaemia in HFpEF
The addition of ExE to the diagnostic criteria also allows the identification of ischaemia (approach 4). One-third of patients diagnosed with HFpEF may have underlying coronary artery disease—an important finding because ischaemia has marked effects on LVDP.31 The aetiology of raised LV filling pressure is, therefore, likely to influence possible treatment strategies. These considerations are also likely to influence the reported prevalence of HFpEF in relation to heart failure with reduced EF,14 32 which currently does not consider the influence of ischaemia on DD and heart failure symptoms.
Limitations
This study assessed consecutive patients with dyspnoea or fatigue referred for clinically indicated ExE, so the study group is heterogeneous. The lack of data from invasive haemodynamic measurements and biomarkers also reflects the usual management of these clinic patients.
There are potential technical limitations for the measurement of E/e′ relating to the fusion of mitral inflow and tissue Doppler measurements. In patients with fused Doppler parameters, images were acquired when the heart rate fell sufficiently to define transmitral profile or Doppler signal.10 This process permits successful assessment of LV filling pressures for several minutes after exercise termination.33 It is also possible that some patients may have had raised LV filling pressure independent of coincidental ischaemia. At present, however, we are unaware of data exploring the interaction between the severity of ischaemia and its influence over LV filling pressure.
Clinical application
This study suggests that ExE is important for identifying exercise intolerance, raised LV filling pressure and detecting ischaemia in patients undergoing assessment of HFpEF. Currently, patients with exercise limitation and raised filling pressure at rest are classified as HFpEF regardless of their exercise response. The measurement of LV filling pressure during exercise is particularly useful in patients presenting with inconclusive resting E/e′—most such patients classified as HFpEF on the basis of supplementary criteria do not display raised filling pressure at exercise. Conversely, a similar proportion of patients with non-conclusive resting function who have elevation of E/e′ during ExE do not meet the current supplementary criteria for DD.
References
Footnotes
Linked articles 188946.
Funding Supported by a project grant from the National Health and Research Council, Canberra, Australia.
Competing interests None.
Ethics approval This study was conducted with the approval of the Princess Alexandra Hospital research ethics committee.
Provenance and peer review Not commissioned; externally peer reviewed.