Article Text

Abstract
Background: The severity of angina is related to a reduction in global quality of life (QoL), which may be improved by anti-ischaemic treatment. It is not known, however, whether improvements relate only to physical or also to mental and social domains of QoL and whether women benefit in a similar way to men.
Objectives: To relate improvements in angina severity through anti-ischaemic treatment to physical and mental domains of QoL in elderly men and women and to assess differences in this relation between the sexes.
Methods: Angina severity and full assessment of QoL by structured, self-administered and validated questionnaires were measured prospectively at baseline and after 6 months’ optimal drug or revascularisation treatment in all 301 patients of the Trial of Invasive versus Medical therapy in Elderly (TIME) patients with chronic angina.
Results: At baseline, angina severity correlated significantly with physical domains of QoL (trend test at least p<0.02) and daily activities (p = 0.05). At similar angina levels, women had significantly lower QoL scores than men. With anti-ischaemic treatment, physical as well as mental and social QoL domains and daily activities improved, together with a relief in angina (trend tests at least p<0.02). This was true for women and men and was more pronounced after revascularisation than with medical treatment.
Conclusions: These findings confirm the relation between angina severity and physical limitation. In addition, they show that anti-ischaemic treatment not only relieves angina and improves physical components of QoL but also improves mental and social domains. This is true for women as well as for men despite the lower overall scores for women.
Statistics from Altmetric.com
It is widely accepted, that patients with angina pectoris (angina) due to chronic coronary artery disease (CAD) also have a reduced quality of life (QoL1–3). The reduction of QoL is, however, mainly related to limitations in physical activities, physical health interferences with work and intensity of pain. These aspects are generally summarised as physical components of QoL. After coronary artery bypass surgery, percutaneous coronary intervention or medical treatment, symptoms generally improve and so does overall QoL.1 2 4–12 Previous studies evaluating the relationship between improvement in chest pain and QoL primarily focused on overall health status or the physical components without providing a detailed analysis of the impact of anginal chest pain and its relief by anti-ischaemic treatment on emotional, mental and social components of QoL. These components express the extent to which emotional problems interfere with work or daily activities. Furthermore, they include general mental health and the interference of physical or emotional problems with normal social activities.
Previous reports of the Trial of Invasive versus Medical therapy in Elderly patients with chronic angina (TIME) showed a significant effect of anti-ischaemic treatment on global QoL5–7 and important sex-related differences—namely, significantly lower overall QoL scores for women than for men, again without analysing the different components of QoL.8
To examine this interrelation by a more comprehensive approach, data of the 301 patients enrolled in the TIME study were analysed, which included prospective repeated evaluations of the symptomatic status as well as full assessments of QoL. Specific aims of this study were (a) to define the relationship between the severity of angina and the different domains of QoL at baseline; (b) to search for baseline factors, particularly gender differences, influencing this relation and (c) to correlate improvements in symptoms due to anti-ischaemic treatment with changes in the different domains of QoL.
PATIENTS AND METHODS
Patients
The TIME study included 301 patients ⩾75 years with chronic angina Canadian Cardiac Society (CCS) class ⩾II despite treatment with at least two antianginal drugs, as previously described.5 Patients with an acute myocardial infarction within the previous 10 days, with significant valvular heart disease or congestive heart failure and those with other life-limiting comorbidities were excluded.
Methods
At baseline, patients were evaluated clinically, including a standard 12-lead electrocardiogram and a stress test if feasible.13 In addition, the severity of angina and QoL was assessed by structured, self-administered and validated questionnaires. Angina pectoris was graded according to the CCS classification (score from 0 to 4, with 4 indicating pain at rest and 0 indicating no pain)14 and the Rose angina score.14 QoL was measured using the Short Form 36 (SF-36) health survey,15 16 which consists of 36 items assessing eight different domains: physical functioning, physical role functioning, pain, health status, vitality, social functioning, emotional role functioning and wellbeing (score from 0 to 100, with higher scores indicating a more favourable status). The 12 most powerful items are grouped in a physical and a mental component score (SF-12).17 To determine possible limitations in daily activities, the 12 questions of the Duke Activity Status Index (DASI)18 were included in the query (score from 0 to 58, with higher scores indicating a more favourable status).
All these measurements were performed at baseline and after 6 months of anti-ischaemic treatment consisting either of optimised antianginal drug treatment (n = 127 (42%)) or revascularisation (n = 174 (58%)) by angioplasty or bypass surgery. Patients were randomised to the two treatment strategies,5 but for the primary analysis of this paper, these anti-ischaemic treatments have been grouped together.
Analyses and statistics
First, the severity of angina by CCS class (II, III and IV) at baseline was correlated with the different domains of QoL and daily activity. Then, a possible influence of age (<80 vs ⩾80 years), sex and presence/absence of diabetes mellitus, which may all be related to pain perception, was determined. To assess treatment effects, the change in angina severity after 6 months compared with baseline was correlated with the changes in QoL. For that purpose, the change in angina severity was categorised as follows: marked improvement = improvement by three CCS classes; mild improvement = improvement by one or two CCS classes; no improvement = no change in CCS class; deterioration = any increase in CCS class. Obviously, patients who died during the 6-month follow-up (n = 19) could not be included in these analyses.
Missing items of the SF-36 were imputed only if at least half of the items were present by computing the subject’s score within the existing items multiplied by the ratio of the maximum possible score for the entire scale to the maximum possible score for the existing items.
Data are presented as mean (SD), as box plots indicating median values, 25th and 75th quartiles and outliers or as mean and 95% CI. Relative group differences were compared using the Fisher exact test and the trend test, whereas continuous data were analysed with the Wilcoxon–Mann–Whitney or the Kruskal–Wallis tests as appropriate. A p value <0.05 was considered to represent a significant difference. Mean QoL changes from baseline to 6 months’ follow-up were adjusted by sex, age, smoking, diabetes and prior coronary heart failure (CHF) using generalised linear models. Statistical analyses were performed using the SAS 8.02 statistics program.
RESULTS
Baseline characteristics
Of the 301 patients analysed, 66 (22%) had angina CCS class II, 141 (47%) CCS class III and 94 (31%) CCS class IV. Table 1 shows the baseline characteristics of these three patient groups. More symptomatic patients showed a tendency toward older age and had more often been treated with long-acting nitrates and heparin (for their symptoms at rest). Gender, however, as well as medical history, risk factors and comorbidities were similarly distributed among the three groups.
Relationship between angina severity and QoL
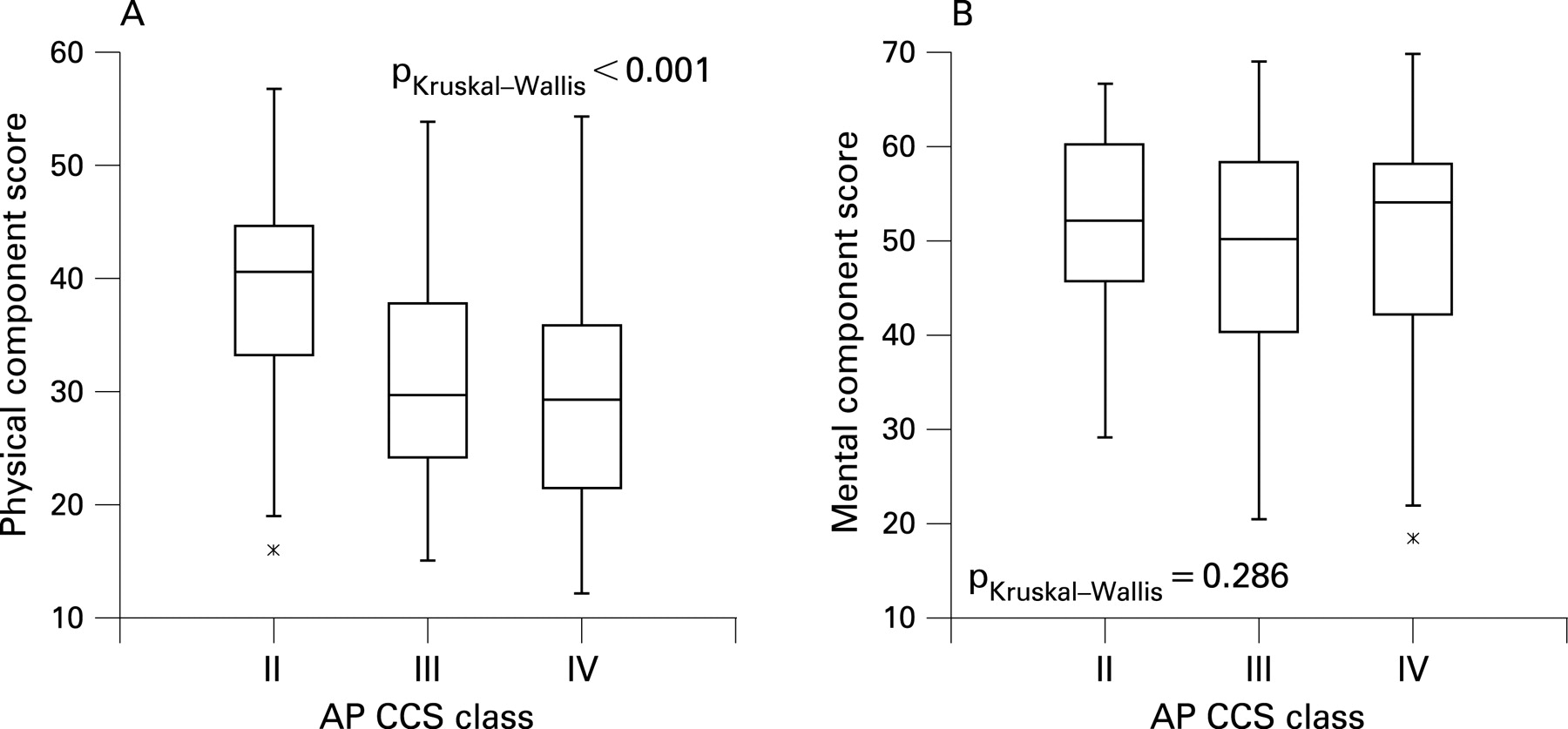
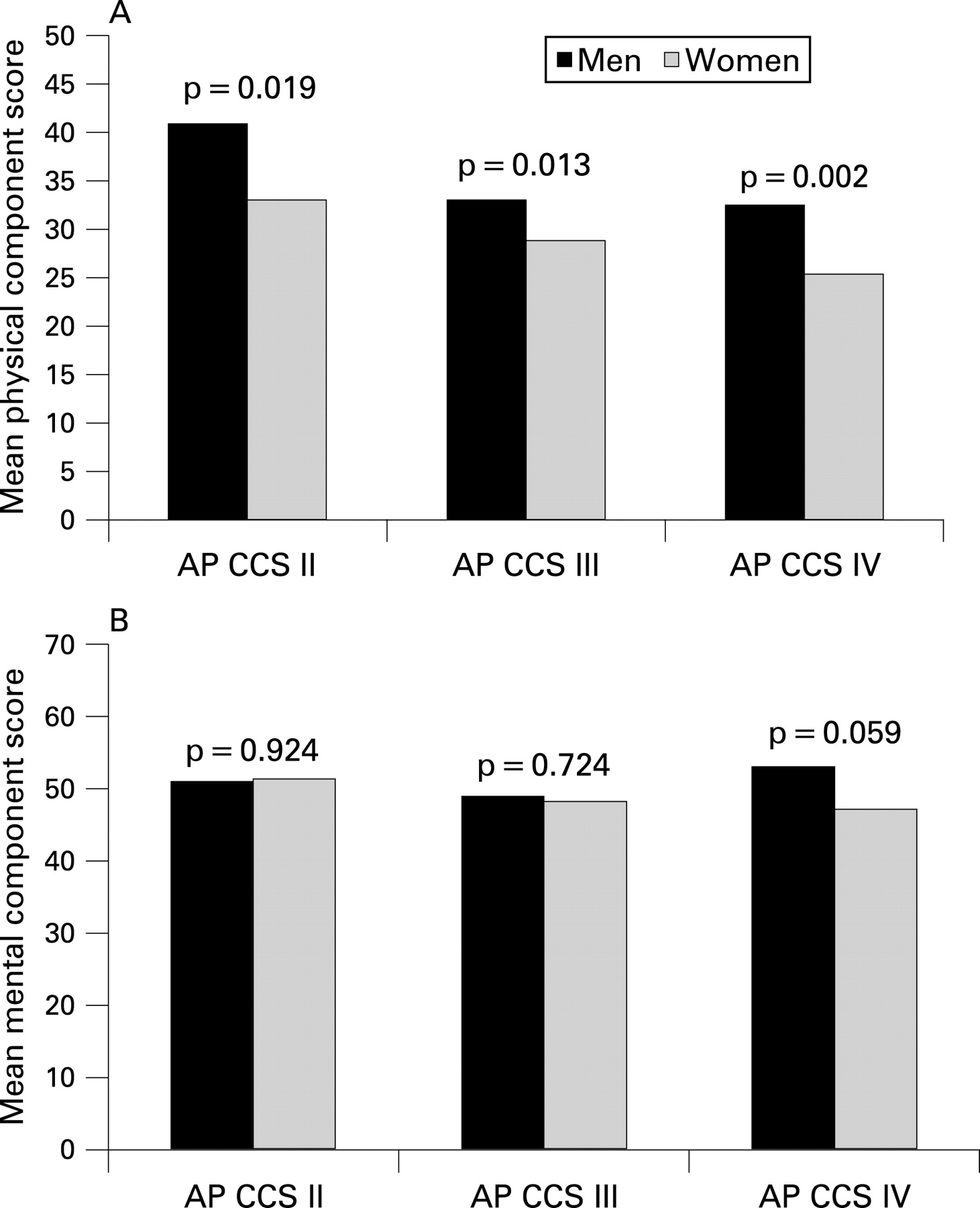
At baseline, there was a significant relationship between angina severity and the physical component score of the SF-12. Thus, lower values in the physical component score were associated with a higher degree of angina (fig 1): CCS II: mean (SD) score 38.6 (9.9), CCS III: mean (SD) score 31.3 (9.3), CCS IV: mean (SD) score 29.5 (9.7) (p<0.001, trend test). In contrast, this relationship was not found for the mental component score. Furthermore, the physical component score was significantly lower in women than in men (p<0.02) for all angina severity groups, again without differences in the mental component score (fig 2). There were, however, no relevant differences between older and younger patients or between patients with and those without diabetes in the SF-12 component scores.

Regarding the different components of the SF-36, angina severity negatively correlated with physical role functioning, physical functioning, pain, health status and vitality as well as with the DASI score but not with social functioning, emotional role functioning and wellbeing (table 2).
Sex differences noted in the SF-12 physical component score were also significantly present in most of the SF-36 physical domains (table 3) as well as in the DASI score (fig 3). Additionally, in the angina severity class CCS IV, DASI scores showed significantly lower values for the very elderly than for younger patients (p<0.02; fig 3). Findings of the Rose score paralleled those of the CCS class so closely that results are only presented for the more familiar CCS class.

Changes of angina severity and QoL in patients receiving anti-ischaemic drug treatment
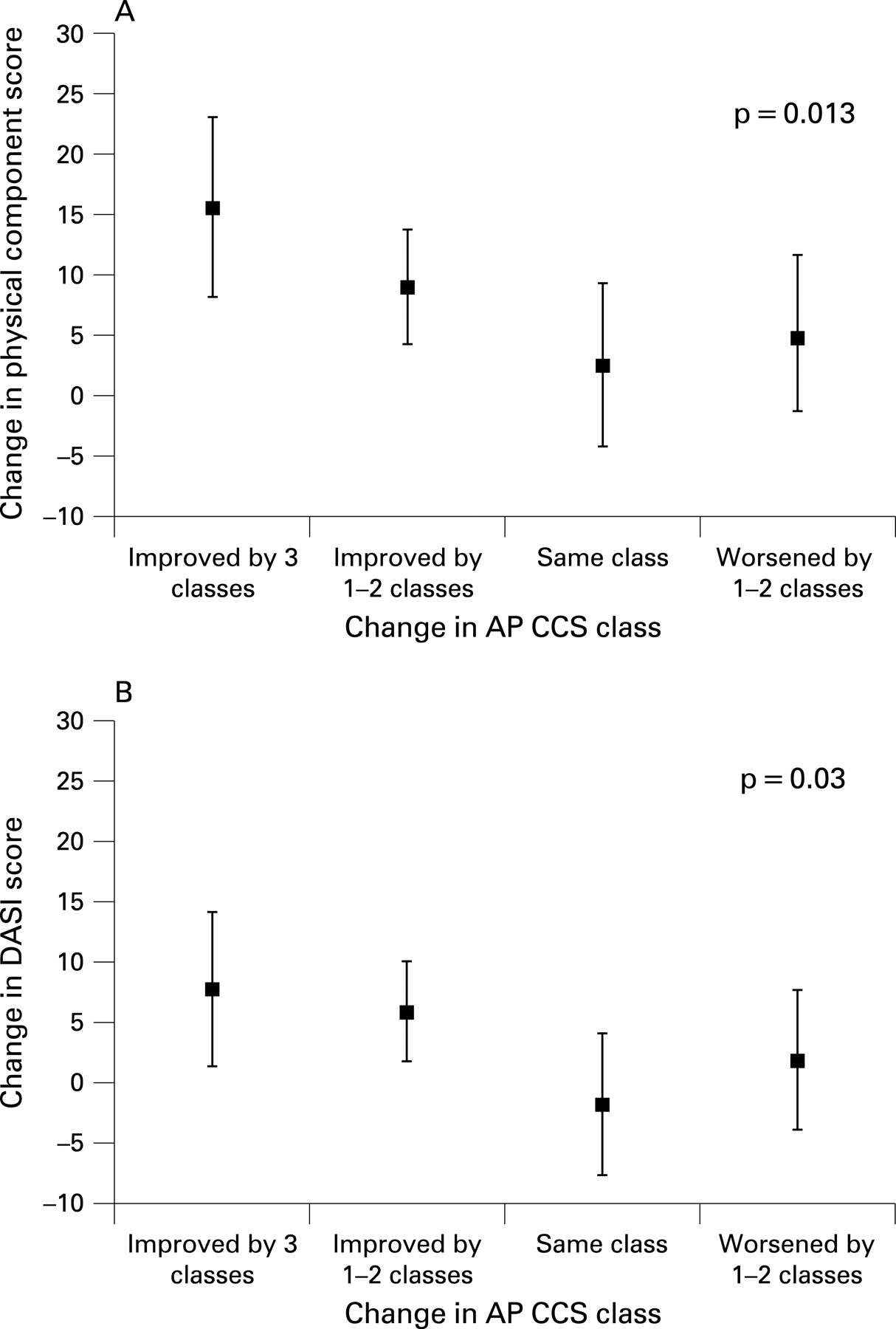
During anti-ischaemic treatment, 78 patients (35%) showed a marked improvement in angina, 73 patients (33%) a mild improvement, while 34 patients (15%) had no change and 37 (17%) complained of more severe symptoms. Changes in angina severity correlated significantly with changes in the SF-12 physical component score (trend test p = 0.013) and the DASI score (trend test p = 0.03; fig 4). These relationships were found both in men and in women (data not shown). In addition and in contrast to baseline findings, the changes in angina severity with anti-ischaemic treatment not only paralleled those of physical domains of the SF-36 but also changes of social functioning, vitality and wellbeing (table 4).
Influence of the type of anti-ischaemic treatment
Of the 301 patients of TIME, 174 (58%) were revascularised within the first 6 months while 127 (42%) received optimised medical treatment.19 Revascularised patients showed a significant relationship between change in angina and the SF-12 physical component score as well as most of the SF-36 domains (pain, physical functioning, health status, vitality, social functioning and wellbeing). In comparison, medically treated patients at best showed a weak correlation between these variables, except the DASI score, where a significant relationship could be shown. Figure 5 illustrates improvements in three representative domains (physical functioning, pain, general health status) for patients with marked, mild, no improvement or deterioration of angina over time. This shows that improvements were present with both anti-ischaemic treatments but more pronounced after revascularisation.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
DISCUSSION
These findings show for the first time that improvements in angina severity by anti-ischaemic treatment improved not only physical QoL domains but also general wellbeing, vitality and social functioning. This was particularly true after revascularisation treatment. Despite sex-related differences in QoL and pain perception, women and men benefited similarly from these treatment-induced improvements in QoL domains. In addition, these findings confirm the relationship between angina severity and limitations in physical and daily activities as described before.1 2 4–7 Thus, these findings add yet another dimension to the gender differences noted in the management of stable angina.20 21
Two previous studies reported reduced measures of QoL with increasing angina severity without relating their findings to the various domains of QoL or treatment effects.3 4 Moreover, a study by Brorsson et al based on a Swedish questionnaire found reduced values of both physical and mental scores in patients with chronic CAD compared with a normal population.1 In contrast, however, Kiebzak et al did not find any differences in the SF-36 domain wellbeing (a mental domain) between patients with CAD compared with a normal population.2 More important seems the finding of our study that improvement in symptomatic status by anti-ischaemic treatment not only improved physical QoL domains and the ability to perform daily activities but also general wellbeing, vitality and social functioning. This reflects the major impact of CAD, independent of its severity, on general wellbeing which can be profoundly improved by anti-ischaemic treatment.
The fact that revascularisation treatment improves symptoms and overall QoL has been shown for bypass surgery and angioplasty1 2 4–12 and these effects were generally more pronounced than those after medical treatment. This analysis confirms these findings. This is a critical point, particularly in an elderly population such as that studied here, where improvements in symptomatic status and QoL may be more important than survival benefits. It is of note, however, that improvements were seen also on optimal medical treatment, although they were less pronounced than after revascularisation.
The lower measurements, especially in physical QoL domains, found in women compared with men in each group of angina severity are a relatively new finding. Previous studies using various QoL questionnaires such as the Seattle Angina Questionnaire (SAQ) and the SF-36 showed that women with CAD generally achieve lower QoL scores than men.1 8 20 21 Six months after revascularisation by coronary artery bypass grafting (CABG) or percutaneous coronary intervention (PCI), QoL improved significantly both in men and women as confirmed by the data presented here. In addition, the present analysis shows that mental as well as physical scores are improved in both genders in response to anti-ischaemic treatment.
This study involved elderly patients and therefore findings may not directly apply to younger patients as well, although the QoL instruments used were developed and validated for younger rather than elderly patients.22 Similarly, there may be gender differences in responses to certain questions of these questionnaires; however, these instruments have been validated for men and women.
Despite these possible limitations, this analysis underlines the direct impact of anginal chest pain on physical and daily activities, and even more importantly, the positive effect of anti-ischaemic treatment, particularly revascularisation, on general wellbeing, vitality and social functioning in addition to improvements in physical and daily activities. These beneficial effects of treatment were noted in women as well as in men despite the lower overall QoL scores of women compared with men.
REFERENCES
Footnotes
Competing interests: None.
Funding: The TIME study has been supported by grants from the Swiss Heart Foundation, Berne, Switzerland and the Adumed Foundation, Switzerland.
The TIME Investigators are listed in reference 5.
Ethics approval: Ethics approval was obtained.