Article Text

Abstract
Objective It is intuitive to suggest that knowledge of the variation in the anatomy of the aortic root may influence the outcomes of transcatheter implantation of the aortic valve (TAVI). We have now assessed such variation.
Methods We used 26 specimens of normal hearts and 78 CT data sets of adults with a mean age of 64±15 years to measure the dimensions of the membranous septum and to assess any influence played by rotation of the aortic root, inferring the relationship to the atrioventricular conduction axis.
Results The aortic root was positioned centrally in the majority of both cohorts, although with significant variability. For the cadaveric hearts, 14 roots were central (54%), 4 clockwise-rotated (15%) and 8 counterclockwise-rotated (31%). In the adult CT cohort, 44 were central (56%), 21 clockwise-rotated (27%) and 13 counterclockwise-rotated (17%). A mean angle of 15.5° was measured relative to the right fibrous trigone in the adult CT cohort, with a range of −32° to 44.7°. The dimensions of the membranous septum were independent of rotation. Fibrous continuity between the membranous septum and the right fibrous trigone increased with counterclockwise to clockwise rotation, implying variation in the relationship to the atrioventricular conduction axis.
Conclusions The central fibrous body is wider, providing greater fibrous support, in the setting of clockwise rotation of the aortic root. Individuals with this pattern may be more vulnerable to conduction damage following TAVI. Knowledge of such variation may prove invaluable for risk stratification.
- transcatheter valve interventions
- cardiac computer tomographic (ct) imaging
- aortic stenosis
- endovascular procedures for aortic and vascular disease
Statistics from Altmetric.com
- transcatheter valve interventions
- cardiac computer tomographic (ct) imaging
- aortic stenosis
- endovascular procedures for aortic and vascular disease
Introduction
New, or worsened, conduction abnormalities following transcatheter implantation of the aortic valve (TAVI) remain a common morbidity.1 This limits the use of TAVI to intermediate-risk and high-risk elderly patients with symptomatic severe aortic stenosis.2–4 The precise anatomical basis for this occurrence is not well understood.1 Structural variation in the aortic root, and its supporting structures, has yet to be taken into account in this regard.
The normal aortic root, extending from the virtual basal ring to the sinutubular junction, has its leaflets hinged from the supporting valvar sinuses in semilunar fashion, producing a crown or coronet-like configuration.5 The spaces on the ventricular aspect of the hinges are occupied by the fibrous interleaflet triangles, with the leaflets coming together distally at the sinutubular junction. In addition to the obvious origins of the coronary arteries, there are subtle asymmetries in the precise structure of these components of the root, including its fibrous support. Such fibrous support usually extends under a portion of the left, and the entirety of the non-coronary sinuses. The support, made up of the area of aortic-to-mitral fibrous continuity, extends from the left to the right fibrous trigones. The fibrous tissue extends further to include the membranous septum, which together with the right fibrous trigone forms the central fibrous body. These differences are in marked contrast to the uniform muscular support provided for the leaflets of the pulmonary root.5 6 The membranous septum is also known to vary in size,7 8 variation recognisable using CT analysis.9 This analysis has also served to identify variation in the rotation of the aortic root relative to the underlying ventricular mass.10 A systematic investigation of variability in the anatomy of the membranous septum relative to rotation of the aortic root, however, has yet to be conducted. This may prove important in understanding, and even reducing, the high prevalence of conduction damage following TAVI. With this in mind, we have analysed the anatomy of the normal aortic root in autopsied specimens, validating the findings by interrogation of CT data sets, with the aim of highlighting any clinical significance of the findings.
Methods
Heart specimen analysis
We studied 26 normal hearts obtained from the Van Mierop Archive at the University of Florida in Gainesville, Florida, the archive at Johns Hopkins All Children’s Hospital in St Petersburg, Florida, and the New York University School of Medicine archive in New York, New York. Transillumination from the right side permitted measurement of the height and width of the membranous septum, along with calculation of its area. Its relationship to the right fibrous trigone was also assessed, permitting identification of any discontinuity between these entities. The height and basal width of the interleaflet triangle interposing between the right and non-coronary leaflets were then measured, again permitting calculation of its area. Rotation of the root was assessed on the basis of the relationship of the interleaflet triangle between the left and non-coronary leaflets to the aortic leaflet of the mitral valve. This permitted recognition of rightward, or clockwise rotation, as opposed to leftward, or counterclockwise rotation relative to the mitral valvar leaflet. Transillumination from the left side permitted assessment of the atrioventricular and interventricular components of the membranous septum, the hinge point of the septal leaflet of the tricuspid valve serving as the dividing line.
CT analysis
Contrast-enhanced CT angiographic data sets performed at Kobe University Hospital in 78 adults with anatomically normal hearts, using the method of orthogonal multiplanar reconstruction,11 were assessed in similar fashion used for the autopsied hearts (figures 1 and 2). The limited quality of the images, however, made it impossible to assess the atrioventricular as opposed to interventricular components of the membranous septum. All the analyses were performed using a commercially available workstation (Ziostation2 V.2.4.2.3, Ziosoft, Tokyo, Japan).
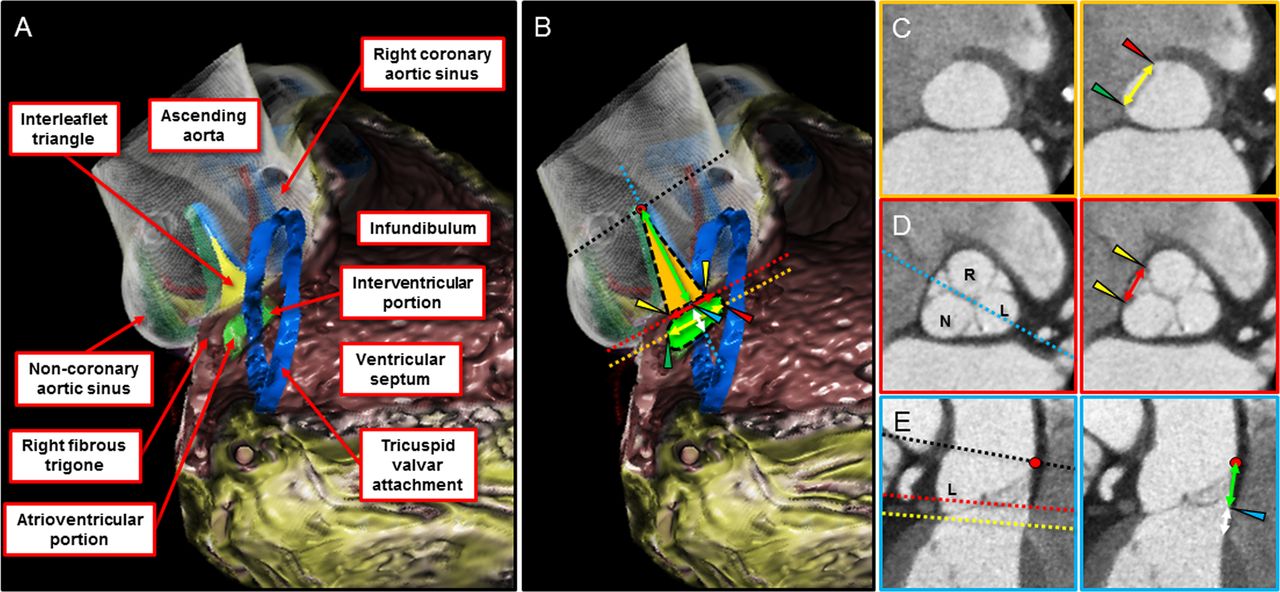
Contrast-enhanced CT angiographic three-dimensional (3D) reconstruction of the aortic root and underlying support (A) demonstrating the membranous septum (green) positioned inferior to the interleaflet triangle (yellow) interposed between the right (R) and non-coronary (N) leaflets (blue and green hinges, respectively). The tricuspid valve annulus (blue circle) bisects the membranous septum into an atrioventricular and interventricular portion. The two-dimensional data sets (C–E) were manipulated to measure the height and width of both the membranous septum and adjacent interleaflet triangle as depicted in this 3D representation (B). (C) The plane of the virtual basal ring (yellow dotted line in panel B) permitted recognition of the anterior edge of the membranous septum (red arrowhead), where the crest of the muscular ventricular septum attaches to the right coronary aortic sinus, and of the posterior edge of the septum (green arrowhead), where it becomes continuous with the right fibrous trigone. The membranous septum width was then measured (yellow double-headed arrow). (D) The virtual basal ring plane was adjusted to the level of the right-sided inner heart curvature (red dotted line) so as to permit measurement of the width of the base of the interleaflet triangle (red double-headed arrow) between the two hinge points (yellow arrowheads) on the plane. (E) The inferior margin of the membranous septum was determined using the orthogonal plane (sky-blue dotted line in Panel D) bisecting the membranous septum and the left coronary aortic sinus (L), as used to identify the edge between the crest of the muscular ventricular septum and the membranous septum. The tip of the interleaflet triangle (red dot) was taken as the sinutubular junction (black dotted line). Note that the sinutubular plane (black dotted line) was not parallel to the virtual basal ring plane (yellow dotted line). This plane was used to measure the heights of both the membranous septum (white double-headed arrow) and the interleaflet triangle interposed between the right coronary and non-coronary aortic sinuses (green double-headed arrow). Note the inferior margin of the low-density tissue (sky-blue arrowhead), corresponding to the epicardial fibroadipose tissue around the right-sided transverse sinus, located just above the membranous septum, where the red dotted plane was set. Each dotted line in panel B corresponds to panels C–E with the same coloured border.

A schematic figure (upper panels) with equivalent CT images demonstrating variations in aortic root rotation using multiplanar reconstruction images (middle panels) with corresponding volume-rendered images (lower panels). Assessment of the rotation of the aortic root was initially determined using the virtual basal ring plane, adjusted parallel up to reveal all three inferior aspects of the three aortic sinuses (upper and middle panels). We focused on the location of the central point of the nadir of the non-coronary aortic sinus (N) relative to the right fibrous trigone (yellow circle), and classifying this marker into either being (A) rotated clockwise (rightward), (B) occupying a central neutral position or (C) rotated counterclockwise (leftward) (upper panels). Note that the membranous septum (white stars) keeps its position below the interleaflet triangle between the right (R) and non-coronary sinuses. The variation is found in its relationship to the right fibrous trigone, being further apart but still in fibrous continuity in the clockwise-rotated root (A), and being immediately adjacent to the right fibrous trigone in the counterclockwise-rotated root (C). Significant difference in the rotation angle of the root is demonstrated among three groups. L, left coronary sinus.
Statistical analysis
Summary statistics of continuous variables were reported as medians and ranges. The Shapiro-Wilk test was used to determine distributional characteristics of continuous variables, the Kruskal-Wallis test for non-normally distributed continuous variables, and χ2 tests to analyse dichotomous and categorical variables. Univariable analyses using linear regression were performed to assess the dimensions of the membranous septum. Intraclass correlations were calculated to evaluate intraobserver and interobserver agreement. JMP V.12 from SAS Institute (Cary, North Carolina, USA) was used for statistical analyses.
Results
Analysis of autopsied hearts
The hearts were obtained from 22 children and 4 adults, with the cause of death known to have been non-cardiac. The dimensions of the membranous septum, found to be independent of rotation, are listed in table 1. When averaged, the atrioventricular and interventricular components proved to be relatively equal, the atrioventricular portion occupying a mean of 48%. There was, however, a wide range of values, from 9% to 91% (figure 3). The dimensions of the adjacent interleaflet triangle, which interposes between the right and non-coronary leaflets, are listed in table 1. The aortic root was located centrally in 14 hearts (54%), with clockwise rotation found in 4 (15%) and counterclockwise rotation in the remaining 8 specimens (31%) (figure 4). Continuity between the membranous and the right fibrous trigone was found in 24 specimens, increasing with clockwise as opposed to counterclockwise rotation of the aortic root. The position of the membranous septum, at the base of the interleaflet triangle, was independent of rotation. In the two specimens with discontinuity, a myocardial band separated the membranous septum from the right fibrous trigone in one (figure 5C). In the other, the interventricular component of the membranous septum itself was bisected by a small strand of myocardium (figure 5D).

(A,B) Variation in the components of the membranous septum as viewed from the rightward aspect with transillumination from behind the septum. The components are determined by the hinge point of the septal leaflet of the tricuspid valve near its commissure with the anterosuperior leaflet at the apex of the triangle of Koch (red and black lines demarcating the tendon of Todaro and the septal leaflet hinge point, respectively). The interventricular component is outlined by a red dotted line, while the atrioventricular component is outlined by a black dotted line.

Variation in rotation of the aortic root. Qualitative assessment of the variation in aortic root rotation was recorded by assessing the interleaflet triangle (asterisk) between the left (L) and non-coronary leaflet (N) relative to the aortic leaflet of the mitral valve. The middle of the aortic leaflet of the mitral valve is marked by a hashed line for reference. (A) Clockwise rotation; (B) neutral position; and (C) counterclockwise rotation. Note the increased distance between the membranous septum (white star) and the right fibrous trigone (yellow circle) with increased fibrous support of the clockwise-rotated aortic root (A) when compared with neutral-positioned (B), and even more the counterclockwise-rotated aortic root (C). Additionally, with counterclockwise rotation of the aortic root, the left coronary sinus becomes almost entirely supported by muscle. R, right coronary leaflet.

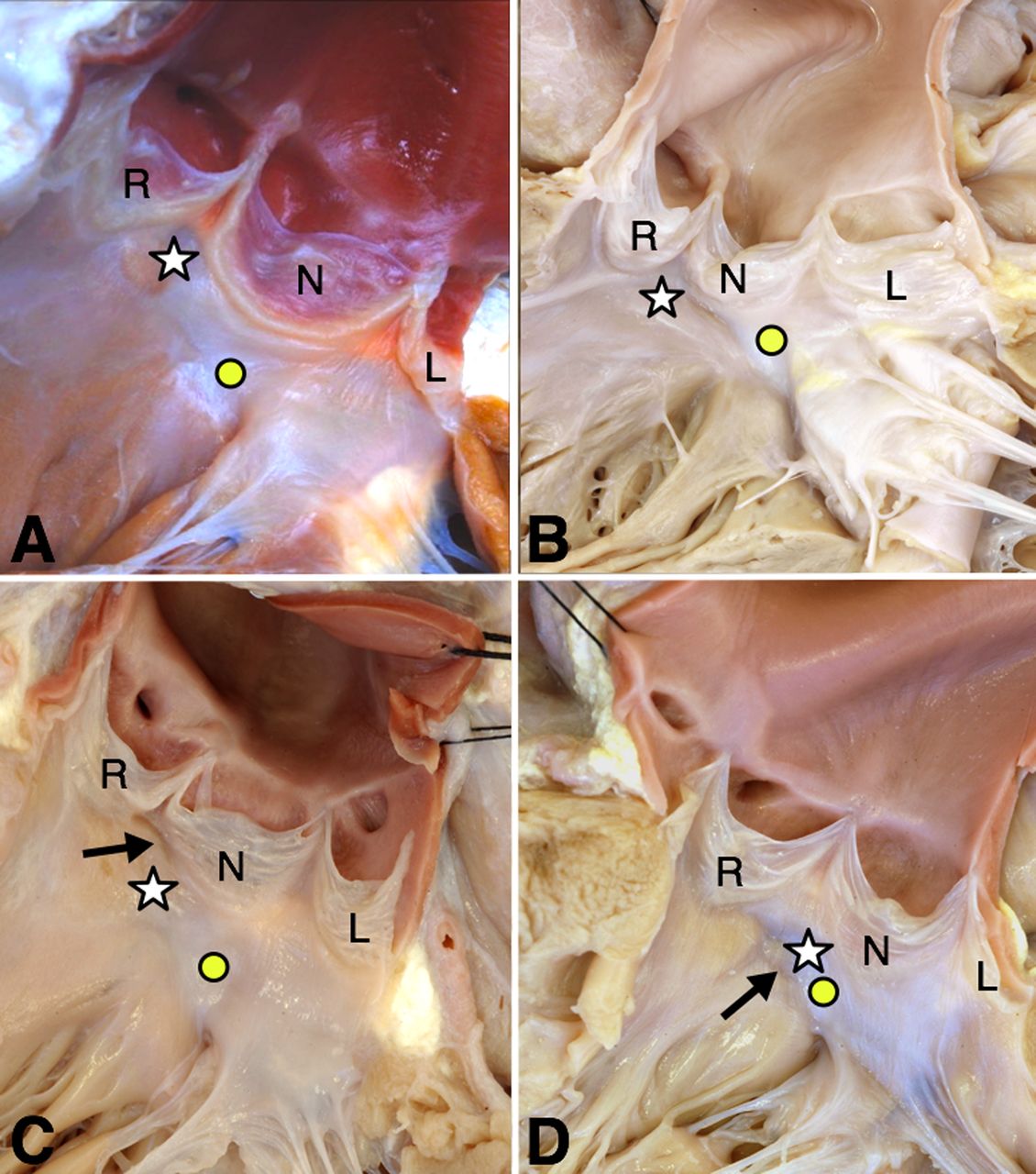
(A) This image shows the normal aortic root in the neutral position. The membranous septum (white star) resides at the base of the interleaflet triangle between the right (R) and non-coronary (N) leaflets, and is in fibrous continuity with the right fibrous trigone (yellow circle), together forming the central fibrous body. The posterior portion of the left (L) and the entirety of the non-coronary sinuses are supported by fibrous tissue in the area of the aortic-mitral fibrous continuity and contiguous central fibrous body. The entirety of the right and the anterior portion of the left coronary sinuses are supported by muscle. (B) In this heart, there is additional fibrous tissue interposed between the right fibrous trigone (yellow circle) and membranous septum (white star), secondary to the clockwise rotation of the aortic root. (C) In this specimen, a band of myocardium (black arrow) separates the membranous septum (white star) from the adjacent interleaflet triangle, thus separating the atrioventricular from the interventricular components. The aortic root is in the neutral position; however, the membranous septum is positioned mostly under the rightward edge of the non-coronary leaflet (N). (D) In this specimen, the band of myocardial tissue (black arrow) extends into the interventricular component of the membranous septum (white star). The aortic root is rotated counterclockwise with the membranous septum and right fibrous trigone (yellow circle) immediately adjacent to each other. The left coronary leaflet (L) is almost entirely supported by muscle.
Heart specimen analysis
When the root was located centrally (54%), the septal myocardium supported the mid-portion of the left coronary leaflet, extending rightward to include the entirety of the right coronary leaflet. Fibrous tissue supported the entirety of the non-coronary leaflet, extending leftward to the mid-portion of the left coronary leaflet. This extent of fibrous support increased or decreased depending on clockwise versus counterclockwise rotation, respectively (figures 4 and 5). Additional significant variations in support, unrelated to rotation, were noted in three specimens (figures 5B,C and 6).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
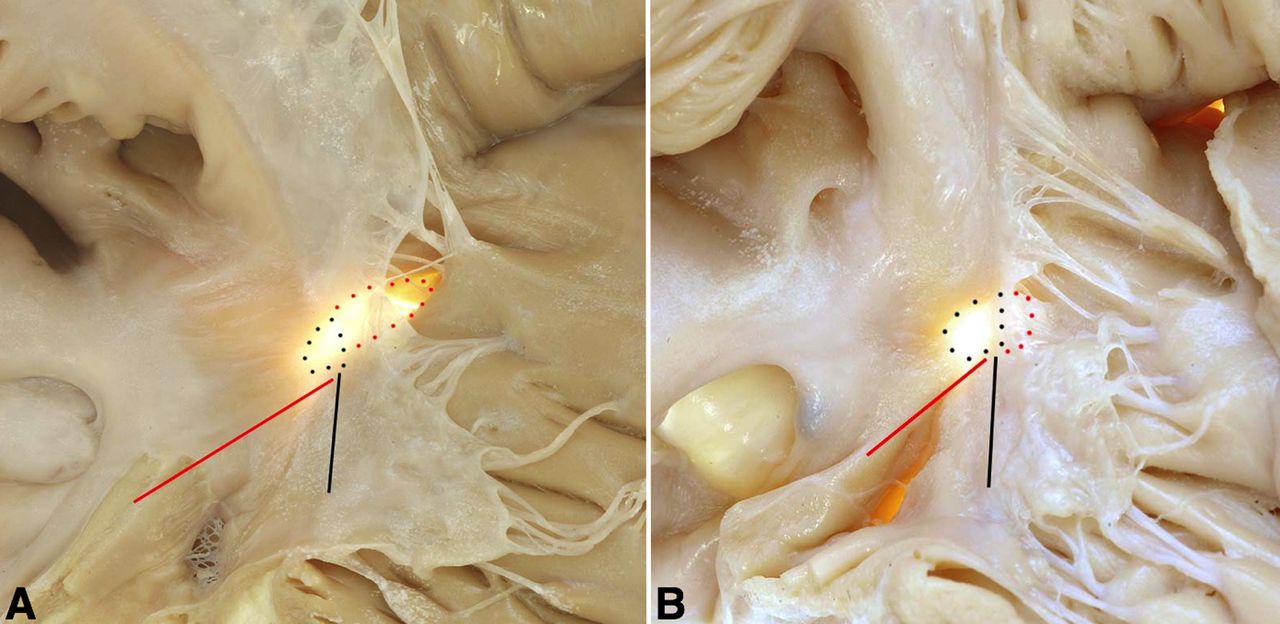
The images show the features of the sinus of Valsalva aneurysm noted incidentally at autopsy in one of our hearts of a patient who died from non-cardiac causes. (A) The membranous septum (white star) is in the usual location, with abnormal extension of fibrous tissue (the extent of which is highlighted with a yellow dashed line) from the right fibrous trigone (yellow circle) and membranous septum, anteriorly underneath the right coronary leaflet (R), presumably weakening the support of the aortic root. An unruptured sinus of Valsalva aneurysm was identified underneath the right coronary leaflet. (B) Viewing the specimen from the right, the sinus of Valsalva aneurysm (green star) is demonstrated protruding between the septal and anterosuperior leaflets of the tricuspid valve partially including the atrioventricular portion of the membranous septum. The intact aneurysmal sac and part of the interventricular component (yellow dots) of the membranous septum were sectioned during autopsy. The triangle of Koch (red and black lines) is directed with its apex pointing towards the aneurysm.
CT analysis
The tomographic scans were obtained from individuals with a mean age of 64±15 years of age, 59% of whom were male. The dimensions of the membranous septum and interleaflet triangle paralleled the findings for the specimens (table 2). The median angulation for rotation of the aortic root was 15.5°, with a range from −32° to 44.7°. The dimensions of the membranous septum again proved independent from rotation of the root. When indexed by body surface area, the height of the membranous septum was positively correlated to its width (r=0.508, P<0.0001), with its position being relatively constant and independent of rotation (figure 2). An increasing separation of the right fibrous trigone and the membranous septum was found with counterclockwise to clockwise rotation (figure 2). The root was located centrally in 44 patients (56%), with 21 patients (27%) having clockwise rotation and 13 patients (17%) counterclockwise rotation (figure 2). There was good intraobserver and interobserver reliability for the measurements undertaken, with correlation coefficients of 0.71 and 0.64, respectively.
CT analysis
Discussion
Our study defines the anatomical relationship between variation in the rotation of the aortic root, the extent of its fibrous structural support and the potential variation in the relationship to the atrioventricular conduction axis. All of these features are important considerations for TAVI. We have confirmed previously reported changes in the shape and size of the membranous septum,7 8 validating our findings using CT analysis of living adults. While confirming that average values for the proportions in atrioventricular as opposed to interventricular location may be equal, we found marked variation in this feature. This has significant implications with regard to estimating the location of the atrioventricular conduction axis. This crucial structure penetrates the atrioventricular component of the septum as it extends to reach the left ventricular outflow tract.12 Rotation of the aortic root is well recognised in the setting of congenitally malformed hearts, such as those with tetralogy of Fallot.13 Normal variation, in contrast, is less well appreciated.10 13 14 It is possible that the changes observed may reflect ageing, including dilation and elongation. CT investigations, which correlated clockwise rotation with dilation of the ascending aorta, however, revealed no association with age.10 Our current findings, therefore, endorse the notion of a congenital aetiology for the rotation, although we found no association between the rotation of the root and the dimensions of the membranous septum. Increasing separation between the membranous septum and the right fibrous trigone, in contrast, was noted in the setting of clockwise rotation. This means that, with such clockwise rotation, the atrioventricular bundle is likely at increased risk during instrumentation or percutaneous implantation of the aortic valve.
Developmental inferences
During initial embryonic development, the entirety of the outflow tract is positioned above the cavity of the developing right ventricle. When initially transferred to the left ventricle, the aortic root remains encased in a turret of outflow tract myocardium. It is only subsequent to regression of this myocardium, concomitant with formation of the aortic valvar sinuses, that there is formation of the fibrous interleaflet triangles. The proximal component of the turret of myocardium, furthermore, also interposes initially between the developing leaflets of the aortic and mitral valves. Initially, therefore, the left ventricle, like the right ventricle, possesses a completely myocardial infundibulum. Only with further maturation does this myocardial inner heart curvature become transformed into the area of fibrous aortic-to-mitral valvar continuity, which serves to anchor the aortic-mitral unit at the summit of the left ventricular myocardial cone.15 16 Variations in the formation and regression of these myocardial components of the developing aortic root account for the changes noted in our study. The changes determining the proportions of the fibrous membranous septum that will be atrioventricular as opposed to interventricular take place subsequent to its initial formation, which completes the process of ventricular septation.17
Implications for transcatheter implantation of the aortic valve
The atrioventricular conduction axis is located along the inferior edge of the membranous septum. It takes its origin from the compact atrioventricular node, which resides at the apex of the inferior pyramidal space.12 The axis, having penetrated the membranous septum, gives rise to the left bundle branch along the crest of the muscular ventricular septum, with the anterior part of the bundle closely related to the nadir of attachment of the right coronary leaflet of the aortic valve. Variability in the location of the atrioventricular bundle has previously been described on the basis of a large autopsy study. In relation to the membranous septum, 50% of individuals were shown to have a relatively right-sided bundle, while 30% had a left-sided bundle. In the remaining 20%, the bundle coursed directly inferior to the membranous septum. This variability had no identifiable gross anatomical association.18 Future studies should assess the correlation of this variability with our novel finding of the association of aortic root rotation and the width of the central fibrous body.
Given the close relationship of the aortic root to the atrioventricular bundle, it is hardly surprising that new, or worsened, conduction abnormalities are prevalent following TAVI, even when using the newer prostheses.1 19–21 The influence of variation in the membranous septum has already been appreciated in the setting of both self-expanding and balloon-expandable valves.19 20 A diminished height of the membranous septum, along with a deeper level of implantation of the device relative to the membranous septum, is now recognised as a predictor for damage to the atrioventricular conduction axis.19 20 22 In the light of these observations, techniques are now proposed to avoid such damage. For the newer Edwards SAPIEN 3 prosthesis, for example, a suggested final depth of implantation of no deeper than 8 mm has been proposed.23 Others have suggested maintaining an aortic percentage of greater than 70%,24 which corresponds to an implantation depth of approximately 5–7 mm, depending on the size of the chosen valve.25 These suggestions are in keeping with the CT findings in our adult cohort, showing the mean height of the membranous septum to be approximately 7 mm.
Most current reports of CT assessment prior to proposed transcatheter implantation, however, suggest analysing the ‘membranous septum’ by using a standard coronal view.19 20 Measurements taken in this plane are likely to overestimate its dimensions. Neither the membranous septum nor the long axis of the left ventricular outflow tract, and hence the alignment of the implanted valve, is located precisely within these planes. Instead, the atrioventricular portion of the membranous septum is located posteroinferiorly, with the interventricular portion located anterosuperiorly (figure 1).
Measurements using an oblique coronal view will be more accurate, since they provide better alignment with the long axis of the left ventricular outflow tract, and hence that of the implanted valve. Unless this oblique plane is objectively defined, the reformatted plane, and the resulting measurements, can be variable. A lack of appreciation of the detailed anatomy could inadvertently lead to inclusion of a portion of the interleaflet triangle in the measurements, thus overestimating the height of the membranous septum. Our own method for assessing both the height and width of the membranous septum, along with the dimensions of the adjacent interleaflet triangle and the degree of aortic root rotation, was designed to avoid these potential caveats. We have shown it to be anatomically accurate and reproducible in the clinical setting.
Strictly speaking, the superior edge of the membranous septum is superior to the plane of the virtual basal ring, or echocardiographic ‘annulus’. The membranous septum is located at the base of the interleaflet triangle between the right and non-coronary leaflets, with the inner heart curvature and the transverse sinus forming its exterior boundaries (figure 1). This implies that the measurement of the membranous septum is inadequate for comparison of the depth of the implantation of the device. The clinically relevant measurement is not the height of the membranous septum, but rather the relationship of the depth of the implanted valve relative to its inferior aspect. If feasible, therefore, it would be preferable to measure the distance between the virtual basal ring and the crest of the ventricular septum. This would permit direct comparison of the intended depth of the implanted device in a plane aligned with the left ventricular outflow tract. It is this distance that is key in estimating the potential risk of inadvertent injury to the atrioventricular conduction axis by the implanted device.26
Our findings are also pertinent to the ongoing variations in design of the prostheses used for transcatheter insertion. The height of the membranous septum is well recognised as an important variable. Its width may prove equally important when considering assessment of calcifications in the left ventricular outflow tract, in particular its impact on potential damage to the atrioventricular conduction axis.2 19–21 27 Appreciation of the normal variation in rotation of the root relative to the membranous septum and central fibrous body, with resulting variation in the underlying fibrous support, should also be taken into account. This is because the conduction axis may take a longer course immediately beneath the clockwise-rotated aortic root, with separation between the right fibrous trigone and membranous septum, increasing its vulnerability during the procedure. Increased fibrous, as opposed to muscular, support of the aortic root may also weaken support of the implanted valve.
Limitations
When calculating the areas of the membranous septum and the interleaflet triangles, we assumed their shapes to be elliptical and triangular, respectively, which is not always the case. The location of the conduction axis itself can also vary relative to the crest of the muscular ventricular septum. As yet, we are unable directly to visualise this feature during life. Measurements made in the autopsy suite, mainly using hearts obtained from children, furthermore, may not be directly comparable to measurements made in living adult patients. Our measurements, nonetheless, demonstrated variability in both cohorts. It was also the case that analysis of the CT data sets was retrospective, carrying its inherent flaws. Inferences made relative to TAVI in these relatively younger patients free of aortic valve disease now need to be validated in individuals who have undergone TAVI. Only in this way will it be shown that these measurements can also reliably be made in the often degenerative and calcified aortic root.
Conclusion
We have demonstrated significant normal variations in the size and shape of the membranous septum, as well as its adjacent interleaflet triangle, which are independent of rotation of the aortic root. Its relationship to the right fibrous trigone, in contrast, does vary depending on rotation of the root. As we have shown, the variability can now be demonstrated using CT interrogation. The findings have obvious clinical significance in revealing the relationship of the aortic root to the atrioventricular conduction axis. Our interpretations can potentially reduce the damage known to occur to the atrioventricular conduction axis following TAVI.
Key messages
What is already known on this subject?
There is normal variation in the rotation of the aortic root and dimensions of the membranous septum.
What might this study add?
The dimensions of the membranous septum vary irrespective of rotation of the aortic root. The width of the central fibrous body, in contrast, is related to such rotation. These features can reliably be assessed by CT assessment.
How might this impact on clinical practice?
The presence of clockwise rotation of the aortic root, with elongation of the central fibrous body, may place individuals at higher risk for conduction damage following transcatheter implantation of the aortic valve.
Acknowledgments
We are indebted to Dr Yu Izawa from the Division of Cardiovascular Medicine at Kobe University Graduate School of Medicine for his assistance in repeating measurements of the CT data sets to assess the reproducibility of our methods. We are indebted to Drs Andrew N Redington and Gruschen Veldtman for their suggestions during the preparation of the manuscript.
References
Footnotes
Contributors JTT planned the study, performed the heart specimen analysis, helped in the statistical analysis, and drafted the initial manuscript and subsequent revisions. SM helped plan the study, performed the CT analysis and related statistical analysis, and made contributions to the revisions of the manuscript. FS helped guide the CT analysis and made contributions to the revisions of the manuscript. SC helped in the heart specimen analysis and made contributions to the revisions of the manuscript. KT and FB helped in the specimen analysis. RSL made contributions to the revisions of the manuscript. TA guided the statistical analysis of the heart specimens and made contributions to the revisions of the manuscript. DES helped in the heart specimen analysis and made contributions to the revisions of the manuscript. RHA guided the study design and made final revisions to the manuscript.
Competing interests None declared.
Ethics approval The studies involved had institutional review board approval at their respective institutions.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Individual data can be shared upon request.