Article Text

Abstract
Objective To evaluate warfarin prescription, quality of international normalised ratio (INR) monitoring and of INR control in patients with atrial fibrillation (AF) and chronic kidney disease (CKD).
Methods We performed a retrospective cohort study of patients with newly diagnosed AF in the Veterans Administration (VA) healthcare system. We evaluated anticoagulation prescription, INR monitoring intensity and time in and outside INR therapeutic range (TTR) stratified by CKD.
Results Of 123 188 patients with newly diagnosed AF, use of warfarin decreased with increasing severity of CKD (57.2%–46.4%), although it was higher among patients on dialysis (62.3%). Although INR monitoring intensity was similar across CKD strata, the proportion with TTR≥60% decreased with CKD severity, with only 21% of patients on dialysis achieving TTR≥60%. After multivariate adjustment, the magnitude of TTR reduction increased with CKD severity. Patients on dialysis had the highest time markedly out of range with INR <1.5 or >3.5 (30%); 12% of INR time was >3.5, and low TTR persisted for up to 3 years.
Conclusions There is a wide variation in anticoagulation prescription based on CKD severity. Patients with moderate-to-severe CKD, including dialysis, have substantially reduced TTR, despite comparable INR monitoring intensity. These findings have implications for more intensive warfarin management strategies in CKD or alternative therapies such as direct oral anticoagulants.
Statistics from Altmetric.com
Introduction
Chronic kidney disease (CKD) is associated with an increased risk of atrial fibrillation and atrial flutter (AF, collectively).1 The prevalence of diagnosed AF among the US patients with CKD requiring haemodialysis has been estimated at more than 10%, but may be as high as 40%.2 ,3
In AF, risk of stroke also increases in the presence of CKD, and CKD has been shown to increase discrimination and classification over the CHADS2 score alone.4 Paradoxically, the risk of bleeding complications in warfarin is also higher in patients with AF, and CKD has been incorporated into several bleeding risk prediction schemata.5 ,6 While it has been well recognised that CKD impacts both stroke and bleeding risk,7 the impact of CKD on AF disease management and quality outcomes is not well-defined. The combined increased stroke and bleeding risk among warfarin-treated patients with CKD may be due to poor quality of the internationally normalised ratio (INR) control (outside the optimal range of 2.0–3.0). We sought to examine the impact of CKD severity on warfarin prescription, quality of INR monitoring and INR control.
Methods
Data sources
The Retrospective Evaluation and Assessment of Therapies in AF study is a retrospective cohort study of patients with newly diagnosed AF treated in the Veterans Administration (VA) healthcare system,8 the largest integrated health system in the USA. Our methods have been previously described.9 We used data from multiple centralised VA patient datasets: (1) the VA National Patient Care Database (NCPD), which contains outpatient, inpatient and long-term care administrative data representing the universe of Veterans Health Administration (VHA) users,10 (2) the VA Decision Support System (DSS) national pharmacy extract,11 (3) the VA Fee Basis Inpatient and Outpatient datasets, which capture non-VA care, (4) Medicare inpatient and outpatient institutional claims data (part A, part B, carrier files) and (5) the VHA Vital Status File, which contains validated combined mortality data from VA, Medicare and Social Security Administration sources. The study was approved by an Institutional Review Board of Stanford University School of Medicine.
Identification of study cohort and predictors
We created a cohort of patients with newly diagnosed AF and evidence of subsequent outpatient VA care. Figure 1 illustrates cohort inclusion and exclusion criteria. We included patients who met the following criteria: (1) primary or secondary diagnosis of AF or atrial flutter (International Classification of Diseases, 9th Revision (ICD-9) 427.31 or 427.32) associated with an inpatient or outpatient VA encounter (‘index date’ of AF diagnosis) between 1 October 2003 and 30 September 2008; (2) confirmatory AF diagnosis in the 30 and 365 days after the index AF diagnosis; (3) at least one primary care, cardiology, women's health, nephrology, geriatric or anticoagulation clinic outpatient visit in the continental USA in the 90 days postindex date; (4) receipt of warfarin prescription in the 90 days postindex date; (5) baseline creatinine value between −365 days and +90 days from the index date. The study period of 2003–2008 was chosen because this period preceded the introduction of direct oral anticoagulants (DOACs), thereby reducing selection bias among warfarin-treated patients.

Cohort selection diagram. AF, atrial fibrillation/atrial flutter.
Medicare linkage
Veterans who were eligible for Medicare benefits could receive INR testing outside of the VA. Therefore, we searched for outpatient INR monitoring data in the Medicare outpatient files that were linked using a validated algorithm that matched on social security number, gender and two of three elements of the date of birth (month, day, year).
Exposure
The exposure of interest was stage of CKD. We used a baseline serum creatinine from 365 days before to 90 days after the index AF diagnosis and calculated estimated Glomerular Filtration Rate (eGFR) using the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) formula.12 If there was more than one creatinine value in this period, the closest value to the date of AF was used. Dialysis status was determined using ICD-9 and CPT codes for dialysis related procedures or diagnoses. Our methods, including correction factors based on type of laboratory assay used, have been previously described in detail.9
Outcomes
INR monitoring rate
Professional society guidelines recommend that patients have INR monitoring once every month or in 4-week intervals.13 Therefore, we assessed INR monitoring quality by calculating an INR monitoring rate, defined as the proportion of warfarin-issued intervals in which INR testing was performed. As in prior literature, we extended the acceptable period of monitoring to once every 42 days, with a 6-day overlap on the head and tail of a calendar month to allow for situations where stable patients had reasonable INR control even without strict testing based on calendar month.14 This 42-day rolling window for INR testing is used internally within the VA as a quality measure for the minimum acceptable monitoring frequency.
INR monitoring rates were calculated using VA outpatient, Medicare outpatient, VA fee basis and inpatient INR VA laboratory data. We also included inpatient INR tests that were performed on the date of discharge. To avoid potential underestimation of INR monitoring rates, we also included INR testing identified from VA Fee Basis and Medicare outpatient claims. We restricted our measurement of INR monitoring rate to include only INRs drawn during periods of warfarin exposure. INR eligibility was determined by evaluating outpatient warfarin dispensation from the DSS file and by secondarily evaluating the frequency of INR monitoring. Active treatment with warfarin was determined by filling of warfarin prescriptions. A grace period of 30 days between prescriptions fills was allowed. An INR monitoring episode is the 42-day period starting with the day of the INR test and extending for 42 days total. Inpatient days were excluded from analysis.
Time in therapeutic range
The primary outcome was overall time in therapeutic range (TTR) of outpatient warfarin use, which represents the TTR for each patient from index warfarin prescription fill until drug or INR discontinuation. We calculated the TTR using the Rosendaal method, which uses linear interpolation to assign an INR value to each day between successive INR values.15 INR values separated by >56 days were not interpolated. We used INR values from outpatient and inpatient VA files and restricted our measurement of TTR to use only eligible INRs. Patients were also assumed to have continuously been on warfarin if prescriptions were filled within 30 days from the end of their prior prescription's supply. Additionally, patients were assumed to have been continuously on warfarin if there was evidence of INR monitoring every 42 days or less. We excluded inpatient hospitalisations from TTR analyses since warfarin is frequently not administered during hospitalisations.14 TTR was also calculated for the first, second and third full year of warfarin use. In order to minimise selection bias based on patients without any INR gaps, second and third year TTR were not conditioned on having a full measurable TTR in the preceding years.
Secondary outcomes were (1) dispensed warfarin prescriptions identified from DSS within 90 days of AF diagnosis; (2) any use of warfarin within the total follow-up period after AF diagnosis; (3) yearly and total INR monitoring rate and (4) time out of therapeutic range.
Clinical covariates
Baseline patient-level comorbidities were identified up to 4 years prior to the date of first AF diagnosis using NCPD, Fee Basis Outpatient Care and Inpatient encounter files. Descriptions of clinical covariates used are in online supplementary appendix A. ICD-9 and Current Procedural Terminology (CPT) codes used to define comorbid conditions are listed in online supplementary appendix B.
Supplementary appendix 1
Supplementary appendix 2
Statistical analyses
We compared differences in baseline characteristics, warfarin prescription prevalence, INR monitoring rates and TTR among patients with varying eGFR groups using χ2 tests for categorical variables and t-tests or analyses of variance for continuous variables. Unadjusted and adjusted odds ratios for warfarin prescription within 90 days of AF diagnosis were also calculated using hierarchical logistic regression adjusting for clinical covariates. To estimate the independent association of CKD stage on TTR, we used multilevel mixed-effects linear regression with random intercepts (Stata command gllamm) clustered by site and adjusted for patient covariates (age, sex, rate, body mass quartile, distance to VA clinics, VA insurance status, mental health conditions, comorbidity index, cancer, anaemia, prior bleeding, cardiovascular medications and Congestive heart failure, Hypertension, Age≥75 years, Diabetes mellitus, prior Stroke or Transient Ischemic Attack (CHADS) component comorbidities). We performed all analyses with SAS V.9.1 (Cary, North Carolina, USA) and STATA, V.11.0 (College Station, Texas, USA).
Role of funding source
The study was funded by an American Heart Association National Scientist Development Grant, Gilead Sciences Cardiovascular Scholars Award, VA Health Services Research & Development Career Development Award, VA Merit. Review Awards. The sponsors were not involved with the study design, data assembly or analysis or manuscript preparation.
Results
Clinical characteristics
Out of 498 171 patients identified with AF in 2004–2008, there were 123 188 patients with newly diagnosed AF who met our criteria for analysis (figure 1). Baseline characteristics are shown in table 1. The mean age was 72±10 years; 1.6% of patients were women. Patients with lower eGFR were generally older, although patients with eGFR <15 mL/min/1.73 m2 or on dialysis groups were younger than patients with more moderate CKD. There were more black patients in the extreme ends of the eGFR distribution. Patients with lower levels of kidney function had higher CHADS2 scores, higher Anticoagulation and Risk Factors in Atrial Fibrillation (ATRIA) bleeding risk scores and higher Charlson and Selim comorbidity scores. Patients with lower eGFR also had a higher prevalence of coronary artery disease, peripheral arterial disease, congestive heart failure, hypertension, diabetes, prior stroke/transient ischaemic attack (TIA), aspirin use and clopidogrel use. Notably, 9.4% of patients with severely reduced kidney function had a history of stroke or TIA, compared with <5% of patients with normal or mildly impaired kidney function. More than three-fourths of all patients with severely reduced kidney function had high ATRIA scores. More dialysis patients had a history of pulmonary embolus or deep venous thrombosis (3.4%) than patients in other eGFR groups.
Baseline characteristics
Use of warfarin by CKD severity
Use of warfarin within 90 days of AF diagnosis decreased with increasing severity of CKD, ranging from 57.2% to 46.4%, although it was higher in patients on dialysis (62.3%) (table 2). There was a similar pattern among patients receiving warfarin at any point in follow-up. After adjustment for covariates, warfarin use decreased across categories of worsening eGFR in non-dialysis patients (table 2). Findings were consistent and without statistical interaction within subgroups stratified based on stroke risk (CHADS2≥1 vs 0), age (≥75 vs <75) and presence or absence of heart failure diagnosis.
Prevalence of warfarin prescription, stratified by severity of kidney disease
INR monitoring rate and time in therapeutic range
INR monitoring rates among warfarin-prescribed patients across strata of eGFR were not significantly different, with 85%–87% of non-hospitalised month-equivalent blocks covered with at least one INR laboratory test (table 3).
Quality of warfarin-associated INR monitoring and time in INR therapeutic range
Overall TTR could be calculated in 57 337 patients. There was significant variation in mean time in therapeutic range across eGFR strata. The proportion of patients with TTR≥60% was lowest in severe CKD, with only 21.1% of patients on dialysis achieving TTR≥60% (table 3).
After multivariate adjustment for site and patient covariates, TTR for patients with CKD was below the conditional mean of TTR for all CKD strata relative to eGFR of 60–89 mL/min (eGFR 45–59: −0.7 (−1.2 to −0.3); eGFR 30–44: −2.6 (−0.3.2 to −2.0); eGFR 15–29: −5.9 (−7.0 to −0.48): eGFR<15: −8.8 (−11.6 to −5.9); dialysis: −17.7 (−20.1 to −15.3); p<0.01 for all).
Across all strata of CKD, TTR values were lowest for patients in their first full year of warfarin use (figure 2). The full first-year TTR was 52.7% (n=33 645), second-year was 60.8% (n=39 503) and third-year was 63.8% (27 719). However, patients with eGFR<30 or those on dialysis had mean TTRs<60% across all years of TTR.
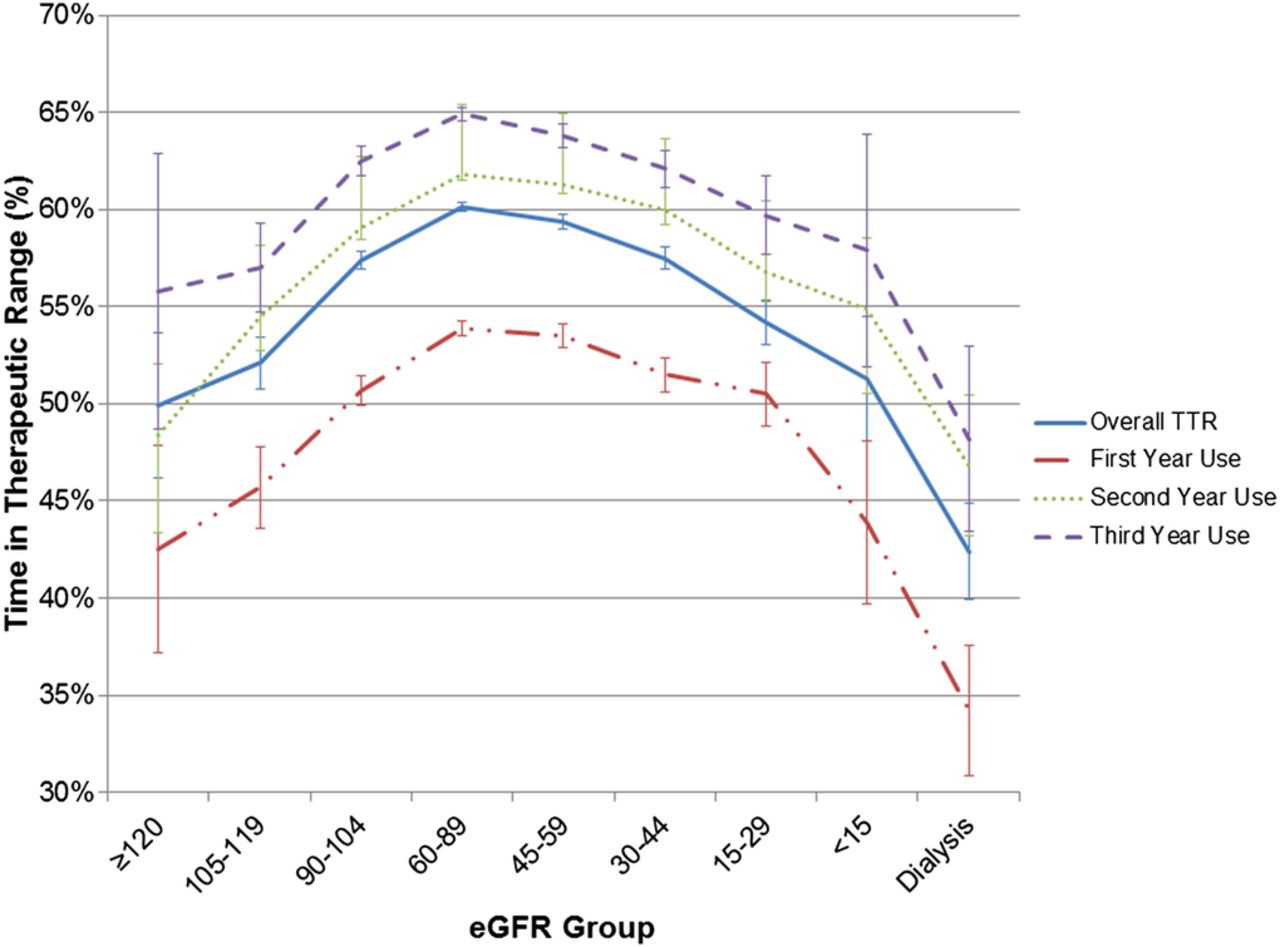
Percent time in therapeutic international normalised ratio (INR) range, stratified by year of warfarin use.
Time out of INR therapeutic range
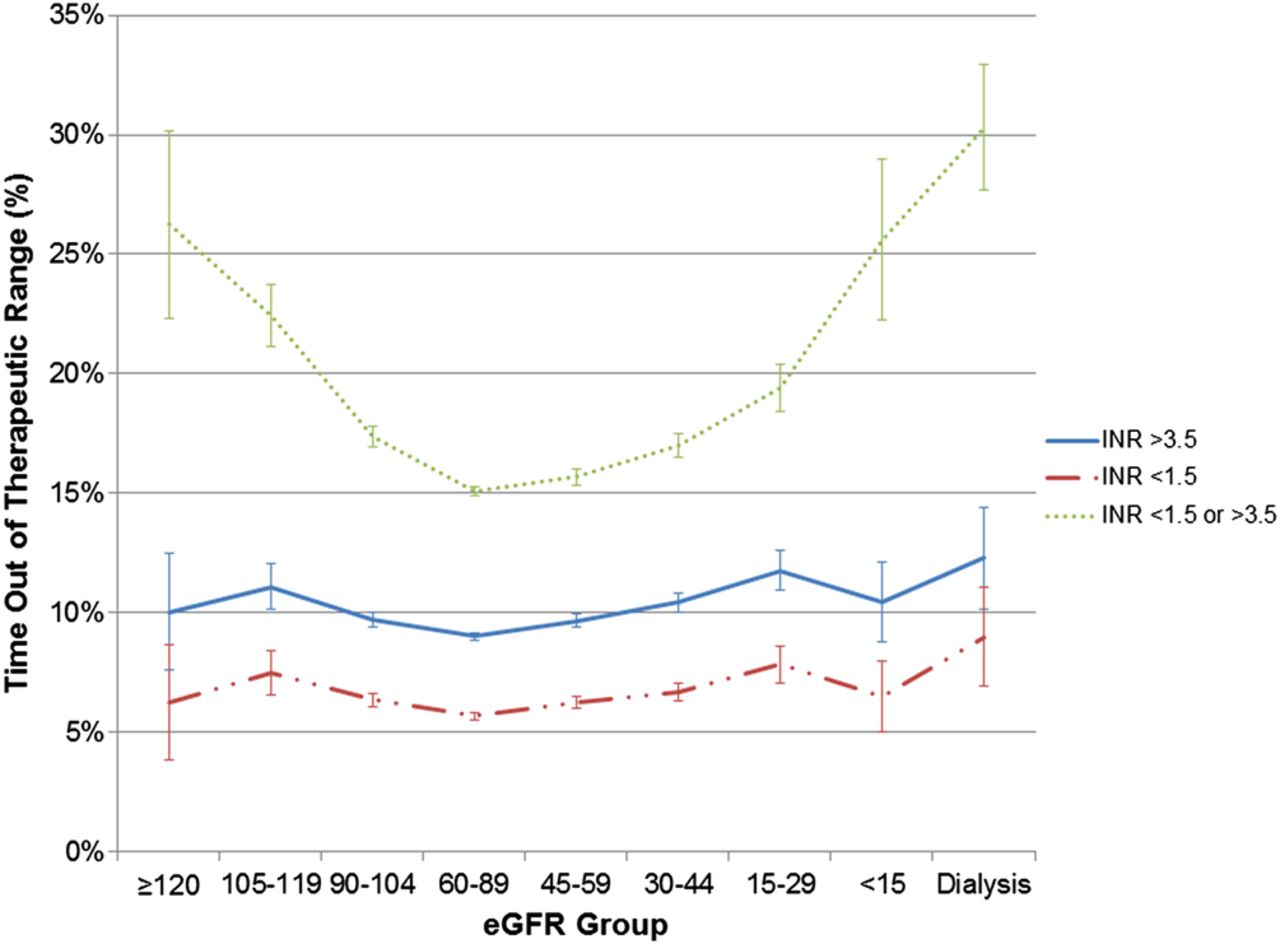
Figure 3 demonstrates the per cent time out of therapeutic range, stratified based on above, below and above or below INR target range. Across all CKD strata, the majority of patients out of range had more supratherapeutic than subtherapeutic time. Among patients on dialysis, 30% of INR time was markedly out of range (INR<1.5 or >3.5), and 12% of INR time was >3.5.

{kind=link}
{kind=link}
{kind=link}
Percent time out of therapeutic international normalised ratio (INR) range.
Discussion
In this US population of VA patients with newly diagnosed AF, we found that: (1) warfarin was prescribed less frequently in patients with moderate-to-severe CKD not on dialysis; (2) patients on dialysis had higher rates of warfarin prescription than non-dialysis CKD patients and (3) patients with CKD, including dialysis, had lower TTR and higher time out of therapeutic range, despite similar INR monitoring intensity. These findings indicate that low TTR in CKD is not mediated by poor INR monitoring and may explain the poor bleeding and stroke outcomes observed in AF with CKD.
Our overall TTR ranges in both new and experienced warfarin users were in line with prior VA studies.13 In the Atrial fibrillation Clopidogrel Trial with Irbesartan for prevention of Vascular Events (ACTIVE-W) trial of warfarin versus clopidogrel plus aspirin, achievement of a TTR of 58% was necessary for treatment benefit with warfarin.16 We found that a strikingly low proportion of patients with severe CKD or on dialysis reached this target despite having similar rates of INR monitoring. Prior studies reported TTR in dialysis patients ranging 10%–49%.17–19
The mechanism by which CKD affects INR levels is not completely understood. Kidney disease can significantly reduce the non-renal clearance and bioavailability of warfarin.20 Animal studies have demonstrated a significant 40%–85% downregulation of hepatic cytochrome P-450 metabolism in patients with CKD.21 Dreisbach and Lertora22 demonstrated a 50% increase in the plasma warfarin S-enantiomer:R-enantiomer ratio among patients with end-stage renal disease. Since the S-enantiomer of warfarin is five times as powerful as the R-enantiomer, this may explain lower reported dosage requirements for warfarin in dialysis patients.23 The decreased non-renal clearance of warfarin and a smaller therapeutic dosage range may explain the difficulty in maintaining INR values in therapeutic range for patients with CKD. The predilection for very subtherapeutic INR values in patients with CKD and dialysis is concerning as these patients frequently have comorbidities which place them at increased for stroke. Additionally, subtherapeutic values indicate the need for continued warfarin dose adjustments, which potentially increase the risk for supratherapeutic values and bleeding.
Current US guidelines advocate regular monthly INR checks as a quality measure and do not provide explicit guidelines on increasing frequency of monitoring in high-risk populations.13 However, more frequent INR monitoring in patients with CKD may be important for management. A prior VA analysis has found that non-white race, poverty, driving distance and mental health conditions increased the likelihood of gaps in INR monitoring.23 However, when adjusting for these and other factors, we found that CKD stage was independently associated with a reduction TTR, with dialysis having the largest effect on the conditional mean of TTR.
There may be lessons to learn from other healthcare systems. A study of patients in Sweden with AF discharged on warfarin after myocardial infarction (MI) found that, across all strata of eGFR, warfarin reduced the risk of a composite of death, MI and ischaemic stroke without increasing bleeding risk.24 Sweden has consistently outperformed other countries in anticoagulation quality, and the majority of centres participate in the AuriculA registry and quality improvement programme, which uses a standardised algorithm for warfarin dosing.25 In AuriculA, more frequent INR sampling is systematically implemented if therapeutic range has not been achieved.
Paradoxically, patients on the higher end of eGFR also had lower mean TTR values. Reasons for this are unclear, although patients in these strata may have artificially elevated eGFRs owing to low muscle mass. Perhaps medication compliance was lower in these groups, which were composed of younger patients with lower CHADS2 scores. Intraperson variability in rates of metabolism or greater dietary variability in younger patients could also be a source for difficulty in INR management.
Finally, DOACs may have a role in moderate-to-severe CKD, although their use in this situation is challenging since all approved DOACs are at least partially eliminated by the kidneys. Physicians are left with few options for dialysis patients with AF. Apixaban is the only DOAC approved in the USA for patients on dialysis. However, the reversibility of warfarin, along with the clinical familiarity of physicians with warfarin, have left it a viable therapeutic option for CKD patients who are already at elevated risk of bleeding and require vascular access multiple times per week. The ongoing introduction of DOAC reversal agents, such as idarucizumab, could alter practice patterns.
Limitations
Our study has several limitations. First, these data were obtained from administrative claims data and there may be misclassification of comorbidities. However, we would expect this to be non-differential across strata of CKD, which could attenuate differences but would be unlikely to cause bias. Second, although we captured Medicare INR values, which were present in a small fraction of patients, we did not have access to INR values from Medicare, thereby potentially leading to larger periods of INR interpolation for TTR measurement in Veteran users of Medicare. Third, in addition to the covariates analysed in the paper, there may also be unidentified confounders, such as frailty, that may not be well ascertained from claims data. Fourth, these data from the VA system may not be generalisable to women or to other healthcare systems. Fifth, it should be recognised that full TTRs for years 1, 2 and 3 of warfarin treatment represent an ‘on treatment’ analysis of patients alive and well enough to remain on warfarin for that duration. Finally, information on albuminuria, the second domain of CKD classification, was unavailable in the vast majority of patients and therefore not considered in our study.
Conclusion
In summary, among patients with newly diagnosed AF, we found wide variation in anticoagulation prescription based on CKD severity. Patients with moderate-to-severe CKD, including dialysis, had substantially reduced TTRs, despite comparable INR monitoring intensity. These findings may have implications for more intensive warfarin management strategies in CKD or alternative therapies such as DOACs, which remain mostly unstudied in patients with advanced CKD.
Key messages
What is already known on this subject?
Patients with chronic kidney disease (CKD) and atrial fibrillation are subject to increased risk for haemorrhage and stroke. Balancing the risk of bleeding events with stroke prevention for patients who receive warfarin is particularly challenging in those with CKD or on dialysis.
What might this study add?
Although international normalised ratio (INR) monitoring quality is similar across the CKD spectrum, patients with decreasing kidney function spend less time in therapeutic range.
How might this impact on clinical practice?
Patients with poor kidney function may require more intensive warfarin monitoring to maximise time in therapeutic range or may require alternative therapies such as direct oral anticoagulants.
References
Footnotes
Contributors All of the authors had a substantial role in the planning, data acquisition, analysis and/or writing of the manuscript.
Funding MPT is supported by a Veterans Health Services Research & Development Career Development Award (CDA09027-1), an American Heart Association National Scientist Development Grant (09SDG2250647), Gilead Sciences Cardiovascular Scholars Award and a VA Health Services and Development MERIT Award (IIR 09-092). WCW's work on this project was supported through NIH grant R01DK095024. The content and opinions expressed are solely the responsibility of the authors and do not necessarily represent the views or policies of the Department of Veterans Affairs.
Competing interests None declared.
Ethics approval Stanford Institutional Review Board.
Provenance and peer review Not commissioned; externally peer reviewed.