Article Text

Abstract
Background Although the presence of an RV lead is a potential cause of tricuspid regurgitation (TR), the clinical impact of significant lead-induced TR is unknown.
Objective To evaluate the effect of significant lead-induced TR on cardiac performance and long-term outcome after cardioverter-defibrillator (ICD) or pacemaker implantation.
Methods A retrospective cohort of 239 ICD (n=191) or pacemaker (n=48) recipients (age 60±14 years, 77% male) from a tertiary care university hospital, with an echocardiographic evaluation before and within 1–1.5 years after device implantation were included. Significant lead-induced TR was defined as TR worsening, reaching a grade ≥2 at follow-up echocardiography. During long-term follow-up (median 58, IQR 35–76 months), all-cause mortality and heart failure related events were recorded.
Results Before device implantation, most patients had TR grade 1 or 2 (64.0%) or no TR (33.9%), but after lead placement, significant TR was seen in 91 patients (38%). Changes in cardiac volumes and function at follow-up were similar between patients with and without significant lead-induced TR, except for larger RV diastolic area (17±6mm2 vs 16±5mm2, p=0.009), larger right atrial diameter (39±10 mm vs 36±8 mm, p<0.001) and higher pulmonary arterial pressures (41±15 mm Hg vs 33±10 mm Hg, p<0.001) in patients with significant lead-induced TR. Patients with significant lead-induced TR had worse long-term survival (HR=1.687, p=0.040) and/or more heart failure related events (HR=1.641, p=0.019). At multivariate analysis, significant lead-induced TR was independently associated with all-cause mortality (HR=1.749, p=0.047) together with age, LVEF and percentage RV pacing.
Conclusions Significant lead-induced TR is associated with poor long-term prognosis.
- HEART FAILURE
- QUALITY OF CARE AND OUTCOMES
Statistics from Altmetric.com
Introduction
Trivial tricuspid regurgitation (TR) is a common echocardiographic finding in healthy individuals.1 However, significant TR (grade ≥2) has been shown to be associated with poor prognosis, regardless of the underlying cardiac pathology.2 Significant TR may be a primary valvular disease (due to valve lesion) or secondary to tricuspid annular dilatation and/or RV remodelling. In addition, placement of an RV (trans-tricuspid) lead has also been associated with a higher risk of TR. However, the incidence of lead-induced TR, time course and effects on long-term outcome remain unknown.3–8 Previous studies have reported the incidence of TR immediately after implantation, focusing on the potential mechanisms of valve dysfunction (perforation, impingement, adherence to the leaflets).4 ,9 However, data on the long-term incidence of TR after device implantation and, more importantly, data on the impact of significant TR on cardiac performance and clinical outcome, are still lacking. Increasing treatment with devices, with growing numbers of implanted pacemakers (PMs) and cardioverter-defibrillators (ICDs), and ageing of the population may result in an increased incidence of lead-induced TR, with important clinical consequences.10–13 Therefore, the objective of this evaluation was first, to assess the incidence of significant lead-induced TR at long-term follow-up and second, to evaluate the impact of significant lead-induced TR on cardiac performance and on long-term prognosis.
Patients and methods
Patients
Patients undergoing an ICD or PM implantation at Leiden University Medical Center between January 2002 and June 2009 were included in this analysis. Data on baseline patient characteristics, implantation procedure, device characteristics and settings, and all follow-up visits were prospectively collected in the departmental cardiology information system (EPD-Vision, Leiden University Medical Center, Leiden, the Netherlands) and retrospectively analysed. Indication for device implantation, based on international guidelines, was primary and secondary prevention of sudden cardiac death in ICD recipients, and sick sinus syndrome and advanced atrioventricular block in PM recipients.13 Owing to evolving guidelines, particularly for prevention of sudden cardiac death, eligibility for device implantation in this population might have changed over time, based on the results of landmark clinical trials.13–15
Patients with de novo implantation of pacing devices were included. Exclusion criteria were (1) previous transvenous (temporary) cardiac pacing system implantation, cardiac valve surgery, congenital heart disease or organic TR, in order to exclude other causes of TR before device implantation; (2) absence of an echocardiographic evaluation within 6 months before device implantation, in order to allow appropriate comparison of implantations before and after evaluations; (3) an echocardiographic evaluation only in the first 6 months after the procedure (mainly in relation to procedure-related complications) or only more than 1.5 years after implantation (evaluation mainly driven by a new clinical event), in order to avoid selection bias; (4) occurrence of heart failure hospitalisation or other major cardiac events in the period between the two echocardiographic evaluations, in order to exclude potential confounding factors in the comparison of TR before and after device implantation; (5) upgrades of systems to cardiac resynchronisation therapy (with or without ICD capabilities), to avoid the potential beneficial effect of resynchronisation on cardiac performance. To evaluate whether lead placement might have induced significant TR, and in order to ensure sufficient time for potential lead-related structural or functional changes to occur, only patients with a follow-up echocardiographic evaluation within 1–1.5 years after the implantation (according to standard follow-up visits) and with a minimal follow-up of 1 year after the echocardiographic evaluation were included.
Device implantation, settings and interrogations
All pacing and defibrillator systems were transvenously implanted and in all patients the RV lead was implanted in the RV apex. The PM settings were individually tailored based on the indication for cardiac stimulation. All patients were followed up every 3–6 months after implantation and devices were interrogated at the implanting centre. To evaluate the potential confounding effect of pacing on outcome, the last percentage of pacing before follow-up echocardiography was used.
Echocardiographic evaluation
Echocardiographic assessment was made with patients in the left lateral decubitus position, using a commercially available system (Vivid 7 and E9, GE-Vingmed Ultrasound, Horton, Norway). Standard 2D and Doppler images were recorded and saved in cine-loop format for off-line analysis (EchoPac, V.110.0.0, GE-Vingmed, Horton, Norway). Echocardiographic evaluation was performed according to the most recent recommendations and included quantification of LV end-diastolic and end-systolic volumes and of LVEF by biplane Simpson's method.16 ,17 LV diastolic function was evaluated according to current recommendations, using transmitral flow Doppler velocities and tissue Doppler imaging-derived mitral annular velocities.18 Transmitral early (E) and late (A) diastolic velocities and E-wave deceleration time were measured using pulsed-wave Doppler recordings at the apical four-chamber view with a 2 mm sample volume at the tips of the mitral leaflets. Peak early diastolic myocardial velocities at septal and lateral borders of the mitral annulus were measured by tissue Doppler imaging and averaged to calculate the mean early diastolic myocardial velocities (E′). The E/E′ ratio was therefore derived as a measure of LV filling pressures. Mitral regurgitation severity was graded according to a multiparametric approach, as recommended.16 In addition, left atrial volume was measured by Simpson's method and indexed to body surface area. The RV dimension was assessed by tricuspid annular diameter and RV end-diastolic area, while RV function was quantified by RV fractional area change and tricuspid annular plane systolic excursion (TAPSE).17 ,19 Right atrial (RA) diameter was also measured and RA pressure was estimated using the inferior vena cava size and collapsibility. Systolic pulmonary arterial pressure was estimated as the sum of the RA pressure and the peak pressure gradient between the right ventricle and right atrium, as measured on the TR spectral continuous-wave Doppler signal.19
TR severity was graded by a multiparametric approach, including assessment of the vena contracta width and regurgitant jet area by colour Doppler, evaluation of TR continuous-wave Doppler signal intensity and pattern of the systolic blood flow in the hepatic veins.16 ,19
Definition of significant lead-induced TR
In order to evaluate the presence and impact of a significant lead-induced TR, patients with stable TR, improved TR or clinically irrelevant deterioration of TR (grade 0 or 1) at 1–1.5 years after implantation (no significant lead-induced TR) were compared with patients with significant TR increase at follow-up reaching grade ≥2 (significant lead-induced TR).
Long-term follow-up and endpoints
Long-term follow-up was performed by chart review and telephone contact with the general practitioner. Survival data were obtained by reviewing medical records and retrieval of survival status through the municipal civil registries. The primary endpoint was all-cause mortality. The secondary endpoint was defined as the combined endpoint of all-cause mortality and heart failure related events—that is, hospitalisation for heart failure, surgical left ventricle restoration, surgical tricuspid valvuloplasty or upgrade to cardiac resynchronisation therapy (whichever comes first).
Statistical analysis
Variables are presented as mean values±SD when normally distributed, as median and IQR when non-normally distributed or as frequencies and percentages when variables were categorical or ordinal. Differences in baseline characteristics between the two groups were evaluated using the unpaired Student t test (continuous variables) and χ2 (categorical data) and Wilcoxon rank sum tests (non-normally distributed continuous variables), as appropriate. Wilcoxon matched-pairs signed-rank test was used to test the significance change in the ordinal variables at follow-up. Differences in echocardiographic variables within and between the patient groups were compared by repeated-measures analysis of variance, including interaction between group and time. Generalised estimating equations were used to compare changes in non-normally distributed echocardiographic parameters or ordinal echocardiographic parameters. Cumulative incidences with 95% CI of all-cause mortality and heart failure related events were analysed using the Kaplan−Meier method, with log-rank tests for comparison between groups. The follow-up onset was set at the moment of the follow-up echocardiographic evaluation. In addition, in patients with LVEF<40% at baseline, a subgroup analysis was performed to evaluate the impact of significant lead-induced TR on the primary and secondary endpoints. To assess whether significant lead-induced TR was associated with increased mortality and/or heart failure related events, Cox proportional hazards modelling was used. Univariate analysis was performed among clinical and echocardiographic variables at the time of the follow-up echocardiography and subsequently, all variables with a p value of <0.05 and no similarity to other parameters (in left and right ventricle dimension and function parameters), were included in the multivariable model. A p value of <0.05 was considered statistically significant. All statistical analyses were performed using IBM PASW Statistics, V.20.0 (SPSS Inc, Chicago, Illinois, USA).
Results
Patients
A total of 239 patients (184 male, mean age 60±14 years, 191 ICD devices) were included in the present analysis. Clinical and echocardiographic characteristics of the patient population before implantation are summarised in table 1. Indication for ICD was primary prevention in 119/191 (62%) patients, while indication for cardiac stimulation was sick sinus syndrome in 27 (56%) and atrioventricular block in 21 (44%) in the 48 PM patients.
Baseline clinical and echocardiographic characteristics of the patient population
Significant lead-induced TR
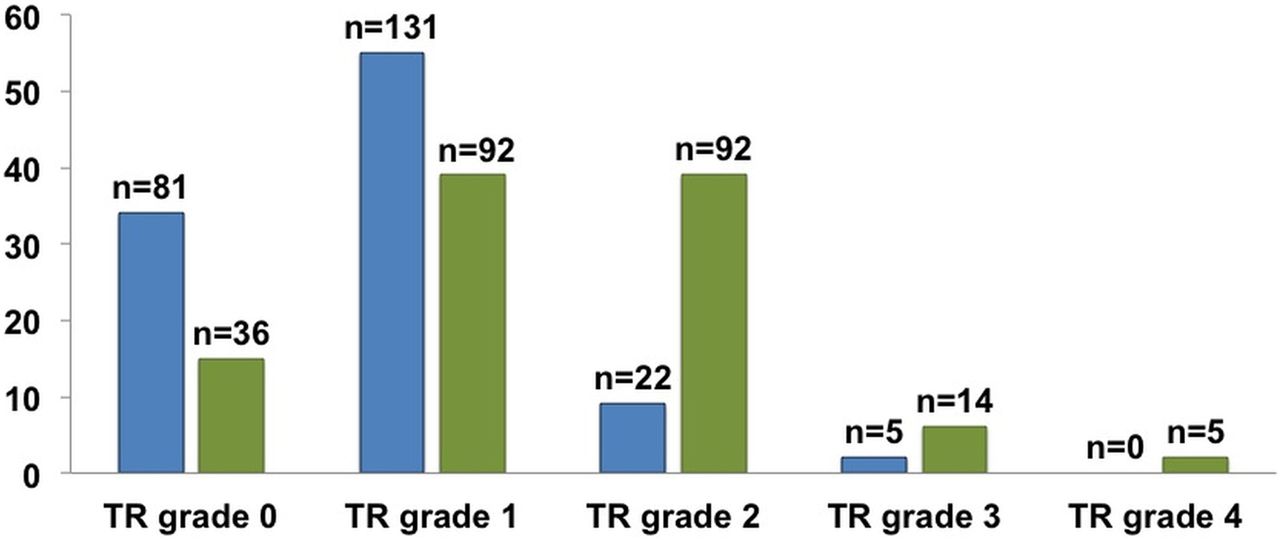
At baseline, some degree of TR (defined as grades 1–2) was present in 153 patients (64%) patients and the distribution of TR grades in the whole patient population before (and after) lead implantation is summarised in figure 1. A significant worsening of TR was observed after lead implantation in the whole population (Wilcoxon p<0.001) and, in particular, significant lead-induced TR was found in 91 (38%) patients. Preimplantation clinical and echocardiographic characteristics of patients with significant lead-induced TR and no significant lead-induced TR are compared in table 1. No significant differences were seen between the two groups, except for a trend (non-significant) towards more frequent atrial fibrillation, a higher prevalence of TR grade 1, and a higher RV fractional area change with a smaller RV end-diastolic area among patients with significant lead-induced TR.

Distribution of tricuspid regurgitation (TR) grade in the study population before (left bars in dark grey) and after (right hand bars in lighter grey) RV lead implantation.
Impact of significant lead-induced TR on cardiac performance
Echocardiographic changes after lead placement in patients with and without significant lead-induced TR are summarised in table 2. Similar changes over time in LVEF and diastolic function severity were seen between the two groups (table 2). Similar changes over time in LVEF, diastolic function and in mitral regurgitation severity were observed between the two groups (see interaction group and time p value in table 2). Although no significant changes over time in RV function (TAPSE and RV fractional area change) were seen in either group, RV size significantly increased over time only in patients with significant lead-induced TR. In addition, an enlargement of RA diameter was found in this group of patients. Finally, pulmonary pressures increased over time only in patients with lead-induced significant TR (from 33±11 to 41±15 mm Hg vs 33±12 to 33±10mm Hg (table 2).
Changes in echocardiographic variables over time (from baseline to 1–1.5 year follow-up) in patients with and without significant lead-induced TR
Impact of significant lead-induced TR on long-term prognosis
The relation between significant lead-induced TR and the primary (all-cause mortality) and secondary (all-cause mortality and heart failure related events) endpoints was evaluated over a median long-term follow-up of 58 months (IQR 35–76 months) after repeated echocardiographic evaluation.
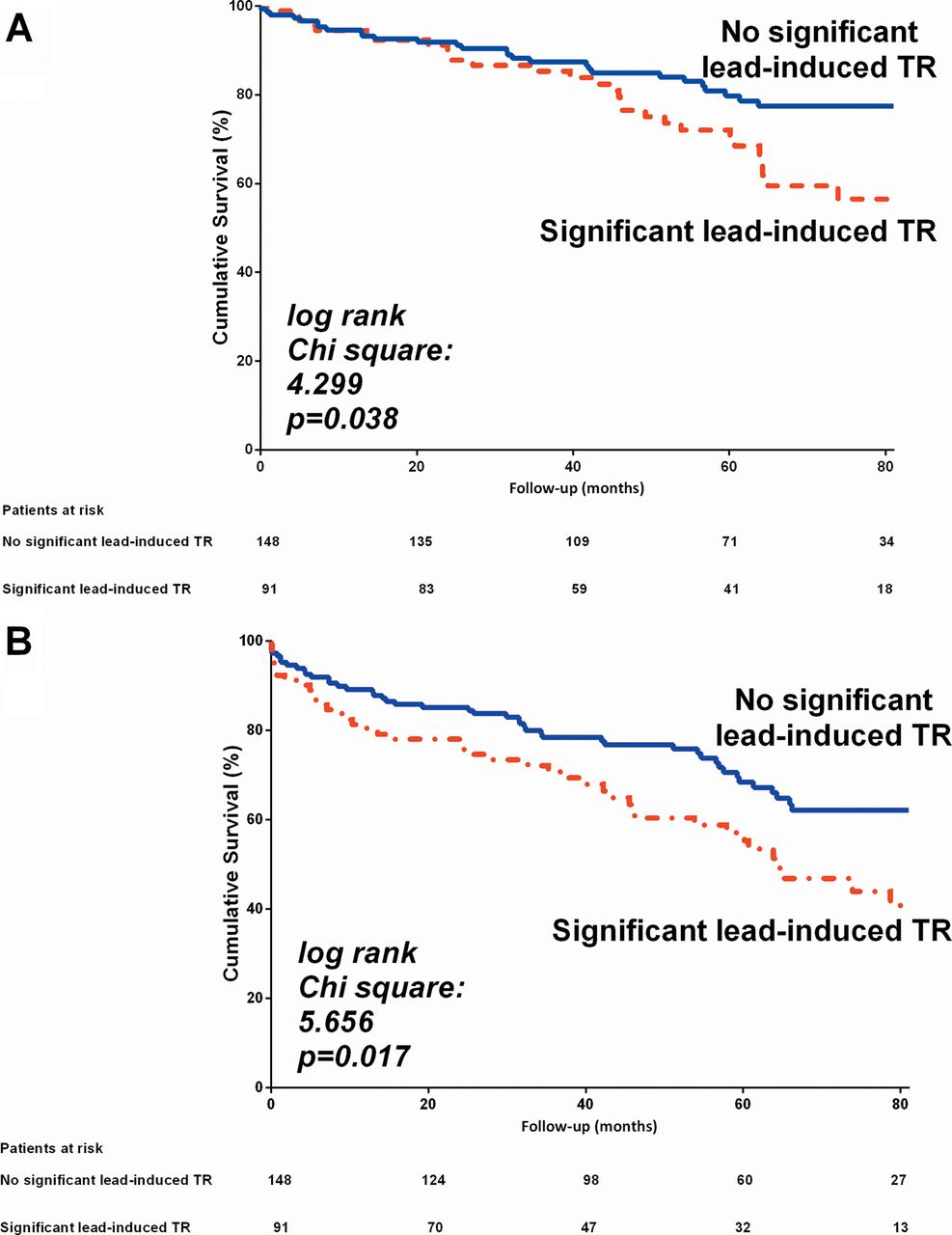
During the follow-up period, a total of 62 deaths (26%) occurred. A higher all-cause death rate (primary endpoint) was seen in patients with significant lead-induced TR (log rank p=0.038; figure 2A). In the univariate Cox proportional HR analysis, significant lead-induced TR reached a HR of 1.687 (95% CI 1.023 to 2.780, p=0.040) (table 3). After adjustment for the other clinical and echocardiographic characteristics, significant lead-induced TR was independently associated with survival (with adjusted HR=1.749 (95% CI 1.008 to 3.035), p=0.047) together with age, percentage of pacing and LVEF.
Univariate and multivariate Cox regression survival analysis for the primary endpoint (all-cause mortality)

(A) Kaplan–Meier survival curves for the time to the primary endpoint (all-cause mortality) in patients with and without significant lead-induced tricuspid regurgitation (TR) with the follow-up onset at time of the follow-up echocardiography. (B) Kaplan–Meier survival curves for the time to the secondary endpoint (all-cause mortality and heart failure related events) in patients with and without significant lead-induced TR with the follow-up onset at time of the follow-up echocardiography.
Similarly, as shown in figure 2B, the secondary endpoint (combination of all-cause mortality and heart failure related events) was observed in 90 (38%) patients. The secondary endpoint was more frequent in patients with lead-induced significant TR (log rank p=0.017). In the univariate analysis, significant lead-induced TR was associated with worse outcome with a HR=1.641 (95% CI 1.087 to 2.480, p=0.019) (table 4). In the multivariate model, significant lead-induced TR was independently associated with the occurrence of the secondary endpoint (adjusted HR=1.649, 95% CI 1.043 to 2.599, p=0.032) together with age, LVEF and mitral regurgitation.
Univariate and multivariate Cox regression survival analysis for the secondary endpoint (all-cause mortality and heart failure related events)
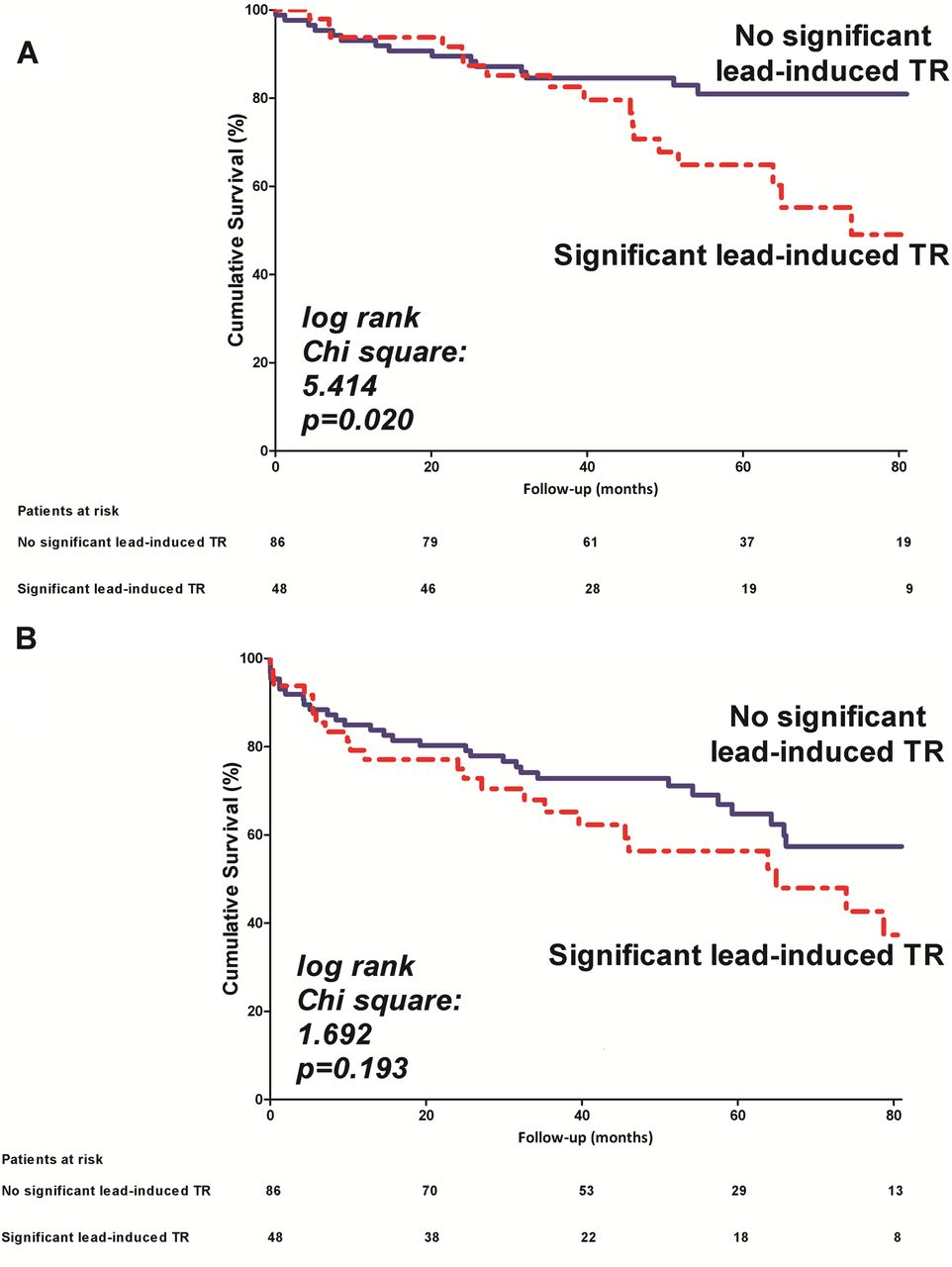
The subgroup analysis in patients with baseline LVEF<40% demonstrated that significant lead-induced TR was associated with poor survival free from the primary endpoint (HR=2.184 (95% CI 1.112 to 4.288), figure 3A) but not with survival free from the secondary endpoint (HR=1.428 (95% CI 0.832 to 2.451), figure 3B).
{kind=link}
{kind=link}
{kind=link}
Subgroup analysis in patients with LVEF <40% before device implantation. (A) Kaplan–Meier survival curves for the time to the primary endpoint (all-cause mortality) in patients with and without significant lead-induced tricuspid regurgitation (TR) with the follow-up onset at the second echocardiography. (B) Kaplan–Meier survival curves for the time to the secondary endpoint (all-cause mortality and heart failure related events) in patients with and without significant lead-induced TR with the follow-up onset at the second echocardiography.
Discussion
The main findings of this study include (1) significant lead-induced TR was observed in 38% of patients 1–1.5 years after placement of an RV lead; (2) significant lead-induced TR was associated with significant RV and right atrium enlargement, and with increased pulmonary pressures at follow-up and (3) significant lead-induced TR was independently associated with worse long-term clinical outcomes (all-cause mortality alone or combined with heart failure related events) after device implantation.
Significant lead-induced TR
The presence of a lead through the tricuspid valve apparatus has been suggested as one of the mechanisms of TR. However, only a few studies have described the incidence of lead-induced TR acutely after implantation and no data are available from the large randomised clinical trials on cardiac devices.3 ,5 ,6 Kim et al evaluated the presence of TR in 248 ICD or PM recipients shortly after implantation and found in 24% of the patients an increase of TR by >1 grade.3 In addition, this increase in TR severity was more pronounced among patients with no or trivial TR, while patients who already were grade 1–3 TR showed only modest worsening of TR. Our study, with longer term follow-up (1–1.5 years), reported a higher incidence of significant (grade ≥2) TR progression (38%), suggesting the additional role over time of chronic lead and valvular structural and functional alterations. Similarly, we observed a trend towards a higher incidence of significant lead-induced TR among patients with only trivial TR before implantation as compared with patients with significant TR. In patients with significant TR before device implantation, with dilated tricuspid annulus and/or of leaflet malcoaptation, the presence of an RV lead may not have significant additional impact on TR severity. In contrast, in patients with new-onset significant TR, an RV lead hampering proper leaflet coaptation seems to be an important pathophysiological factor.
The exact mechanism of development and progression of TR after cardiac device placement has not been fully elucidated and may result from the mechanical interference of the RV lead with the tricuspid valve3 ,4 and/or from a direct effect on TR of RV pacing.20 In this study, no significant differences were seen in baseline clinical, echocardiography and device-related (ICD vs PM) characteristics among patients who did or did not develop significant TR after implantation, underlining the challenge of finding clear predisposing preimplantation parameters associated with lead-induced TR. These results suggest that significant lead-induced TR may result from progression of a pre-existing cardiac/valvular disease and also from interaction between the RV lead and tricuspid valve apparatus.
Impact of significant lead-induced TR on cardiac performance
This study showed that patients with significant lead-induced TR at follow-up had an increase in RV and RA dimensions and an increase in pulmonary pressures, while these parameters remained unchanged in patients without significant lead-induced TR. RV function, as assessed by TAPSE and RV fractional area change, did not change significantly at follow-up in patients with significant lead-induced TR, probably owing to the facilitated ejection in a low-resistance chamber (from the right ventricle to the right atrium).
The impairment of RV performance seen in patients with significant lead-induced TR is unlikely to be secondary to a worsening of LV performance. Indeed, the overall cohort showed a slight worsening of LV size and function at follow-up, as might be expected according to the natural history of heart failure or RV chronic pacing. However, no significant differences were noted in the changes over time in LV volumes and systolic and diastolic function among patients with or without significant lead-induced TR. Furthermore, the change over time in severity of mitral regurgitation was also similar among patients with or without significant lead-induced TR.
A potential explanation for increased pulmonary pressures, and therefore progression of TR and RV dilatation, might be the occurrence of multiple subclinical pulmonary emboli secondary to RV lead thrombus formation. Supple et al described a significantly higher increase in pulmonary pressure in patients with a mobile thrombus around the leads after cardiac device implantation as compared with patients without a mobile thrombus.21 However, the increase in pulmonary pressures did not reach the cut-off value proposed by current guidelines to define pulmonary hypertension (>50 mm Hg) and therefore the diagnosis of pulmonary hypertension is not definitive in the absence of other echocardiographic parameters.18 This suggests that the development of significant TR after lead implantation plays a primary role and is one of the major determinants of the changes in RV performance.
Impact of significant lead-induced TR on long-term prognosis
Although the presence of significant TR, regardless of aetiology, is a well-known prognostic factor, data on long-term outcome in patients with significant TR after RV lead implantation have not been reported.2 Our study demonstrated the independent association between significant lead-induced TR and all-cause mortality (combined with heart failure related events or not). Other variables independently associated with long-term outcomes (primary and secondary) were age, LVEF, percentage of RV pacing and significant mitral regurgitation, which are all known determinants of the development of heart failure and increased mortality. In particular, subanalysis according to the baseline LVEF showed that significant lead-induced TR in patients with a depressed LVEF (<40%) at baseline was associated with poor prognosis. RV pacing has been previously shown to be associated with an increased risk of LV (progressive) dysfunction and heart failure events.22–24 This detrimental effect of RV pacing might be mediated by induction of LV dyssynchrony24 ,25 but also by a direct negative effect on the severity of TR, as suggested by Vaturi et al.20 However, analyses of large trials showed that implantation of an ICD, even with minimal percentage of RV pacing, was associated with an increased risk of hospitalisations for congestive heart failure and death as compared with controls.26 The exact reason for this increased risk of heart failure events has not yet been elucidated but, considering the results of our study, might also be explained by lead-induced TR. Indeed, even modest grades of TR were associated with an increased risk of all-cause mortality.
These findings emphasise the importance of echocardiographic surveillance of ICD and PM recipients, enabling anticipation of the development of heart failure. Although lead repositioning or extraction might be an option only in the short-term after implantation, other therapeutic options, such as upgrade to a biventricular pacemaker, optimisation of heart failure drugs or a surgical procedure on the tricuspid valve, might be considered in patients with significant TR and/or worsening LV function.
Several limitations of this study should be mentioned. First, the exact mechanism of lead-induced TR could not be confirmed in all patients. In addition, it remains unclear whether progression of RV remodelling is the cause or the consequence of significant TR. Moreover, the time interval between echocardiographic evaluations of 1–1.5 years was chosen to ensure identification of both acute and long-term occurrence of significant TR, but might still have underestimated the incidence of this complication, particularly because patients who died within 1 year after implantation were excluded. The mode of death was not systematically available and the impact of significant lead-induced TR on cardiovascular mortality could not be assessed. Finally, prospective studies with larger patient groups and longer follow-up are needed.
In conclusion, a significantly increased incidence of TR was seen at follow-up after implantation of an RV lead in more than 35% of ICD and PM recipients. A significant lead-induced TR was associated with an impaired RV performance and with a higher incidence of long-term mortality and heart failure events. These findings suggest the importance of echocardiographic follow-up in these patients in order to optimise patient management.
Key messages
What is already known about this subject?
-
Trivial tricuspid regurgitation (TR) is a common echocardiographic finding in healthy individuals. However, significant TR (grade ≥2) has been shown to be associated with poor prognosis, regardless of the underlying cardiac pathology.
-
Placement of an RV (trans-tricuspid) lead has been suggested as a cause of TR. However, the incidence of lead-induced TR, time course and, more importantly, data on the impact of significant TR on cardiac performance and clinical outcome remain unknown.
What does this study add?
-
This study evaluated for the first time the impact of significant lead-induced TR on cardiac performance and on the long-term prognosis. A >35% incidence of significant TR was seen at follow-up after implantation of an RV lead. Furthermore, significant lead-induced TR was associated with a significant RV and right atrium enlargement and, importantly, with a higher incidence of long-term mortality and heart failure events.
How might this impact on clinical practice?
-
The findings of this study suggest the importance of an echocardiographic follow-up in implantable cardioverter-defibrillator and pacemaker recipients in order to optimise patient management, including optimisation of heart failure treatment and eventually, tricuspid valve surgery.
Acknowledgments
Department of Cardiology of Leiden University Medical Centre received unrestricted research grants from Medtronic, Biotronik, Boston Scientific, Lantheus Medical Imaging, St Jude Medical, Edwards Life Sciences and GE Healthcare. VD received consulting fees from St Jude Medical and Medtronic.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
-
Contributors UH, DA, JT, VD, JJB and NAM were responsible for study design. UH, DA, JT, ERH and ETvdV participated in data collection. UH, RW, DA, VD and NAM analysed the data and drafted the manuscript. JJB, MJS VD and NAM critically revised the manuscript. All authors approved the final version of the submitted manuscript.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.