Article Text

Abstract
Background Aortic valve calcification (AVC) is considered a manifestation of atherosclerosis. In this study, we investigated whether AVC adds to cardiovascular risk prediction beyond Framingham risk factors and coronary artery calcification (CAC).
Methods A total of 3944 subjects from the population based Heinz Nixdorf Recall Study (59.3±7.7 years; 53% females) were evaluated for coronary events, stroke, and cardiovascular disease (CVD) events (including all plus CV death) over 9.1±1.9 years. CT scans were performed to quantify AVC. Cox proportional hazards regressions and Harrell’s C were used to examine AVC as event predictor in addition to risk factors and CAC.
Results During follow-up, 138 (3.5%) subjects experienced coronary events, 101 (2.6%) had a stroke, and 257 (6.5%) experienced CVD events. In subjects with AVC>0 versus AVC=0 the incidence of coronary events was 8.0% versus 3.0% (p<0.001) and the incidence of CVD events was 13.0% versus 5.7% (p<0.001). The frequency of events increased significantly with increasing AVC scores (p<0.001). After adjustment for Framingham risk factors, high AVC scores (3rd tertile) remained independently associated with coronary events (HR 2.21, 95% CI 1.28 to 3.81) and CVD events (HR 1.67, 95% CI 1.08 to 2.58). After further adjustment for CAC score, HRs were attenuated (coronary events 1.55, 95% CI 0.89 to 2.69; CVD events 1.29, 95% CI 0.83 to 2.00). When adding AVC to the model containing traditional risk factors and CAC, Harrell's C indices did not increase for coronary events (from 0.744 to 0.744) or CVD events (from 0.759 to 0.759).
Conclusions AVC is associated with incident coronary and CVD events independent of Framingham risk factors. However, AVC fails to improve cardiovascular event prediction over Framingham risk factors and CAC.
Statistics from Altmetric.com
Introduction
Aortic valve calcification (AVC) is associated with increased cardiovascular (CV) morbidity and mortality.1 Although AVC is usually not considered part of the atherosclerotic process, shared pathomechanisms of heart valve calcification and coronary atherosclerosis have been discussed.2–5 Today, echocardiography is the standard imaging technique for detection of aortic valve pathologies. However, with the advent of cardiac CT, the quantification of AVC with high accuracy and reproducibility is possible without additional radiation exposure or contrast administration.6 ,7
In a multi-ethnic cohort without clinical CV disease (CVD) at baseline, CT derived assessment of AVC was associated with risks of coronary and CV events beyond those predicted by traditional risk factors, but not when coronary artery calcification (CAC) was included in the model.8 However, whether AVC adds to CV risk prediction beyond Framingham risk factors has not been evaluated in a population based setting.
In this analysis we aimed to examine the prevalence and extent of AVC as detected by CT and to determine its relationship with CV risk factors as well as CAC in participants of the population based Heinz Nixdorf Recall Study. Furthermore, we assessed its association with CV events and whether AVC adds incremental value to CV event prediction beyond established risk factors and CAC, with special attention to gender differences. These analyses may have an implication for treatment targets in primary prevention.
Methods
Study population
Details of the rationale of the Heinz Nixdorf Recall (Risk Factors, Evaluation of Coronary Calcification, and Lifestyle) Study design have been published in detail.9 ,10 Briefly, participants were selected from mandatory inhabitant lists. Between 2000 and 2003, 4814 participants aged 45–75 years were enrolled. Physician- or self-referral was not allowed to avoid selection bias.11 Established CV risk factors, but not the CAC and AVC scores, were reported to the participants. All participants provided written informed consent and the study was approved by our institutional ethics committees.
CV risk factors and questionnaires
Traditional CV risk factors were measured at index presentation, with details being previously published.9 ,10 Medical history and smoking status were evaluated at baseline examination by computer assisted interviews. Current regular use of medication, including antihypertensive or antidiabetic medication or lipid lowering drugs, was recorded in a standardised medication assessment. Resting blood pressure was measured with the subject seated, using an automated oscillometric blood pressure device (Omron, HEM-705CP-E). The mean of the second and third value of three measurements was calculated. Body mass index (BMI) was calculated as weight/height2 (kg/m2). Standardised enzymatic methods were used to determine serum total cholesterol, low density lipoprotein (LDL) and high density lipoprotein (HDL) cholesterol values. Participants were considered diabetic if they reported a physician diagnosis of diabetes, used anti-diabetic medication, or had a blood sugar value ≥200 mg/dL.9 ,10 From these risk factors, the Framingham risk score (FRS) (ie, predicted 10-year risk) was computed.12
Electron beam CT
As part of the study, subjects underwent cardiac CT for quantification of CAC. Electron beam CT scans were performed utilising a C-100 or C-150 scanner (GE Imatron, South San Francisco, California, USA) without the use of contrast media. Contiguous 3 mm thick slices to the apex of the heart were obtained at an image acquisition time of 100 ms.10 ,13 CAC was defined as a focus of at least four contiguous pixels with a CT density ≥130 Hounsfield units and quantified using the Agatston method.14
Valve calcium measurement
Consistent with accepted methodology,2 ,8 ,15 AVC was measured by using the same lesion definition as for CAC. AVC was defined as calcium deposits on the aortic cusps or nodular deposits at the coaptation points of the aortic cusp. Calcium within the aortic sinuses and aortic wall were excluded from analysis. To minimise potential bias, the readers were blinded to the clinical presentation or risk factor profile of the participants. The absence of AVC was assigned a score of 0.
Follow-up and endpoint definition
For the analyses of this paper, participants were followed up for 9.1±1.9 years. Start time of follow-up was the date of measurement of the Framingham risk variables (FRV). Time between FRV measurement date and CT scan date was 11±38 days. Annual postal questionnaires assessed the morbidity status during follow-up—that is, medication, hospital admissions, or outpatient diagnoses of CVD. In parallel, all death certificates were regularly screened. Incident CV morbidity and mortality were validated by review of hospital records and records of the attending physicians, and classified by an external endpoint committee, blinded to the risk factor status and CAC score. Endpoints for this study were based on unequivocally documented incident coronary events that met predefined study criteria.9 Myocardial infarction was defined based on symptoms, electrocardiographic signs, and enzymes (values of creatine kinase (CK-MB)), as well as troponin T or I, and necropsy as: (1) non-fatal acute myocardial infarction; and (2) coronary death.
In addition we studied stroke events, which were attributed to information provided in hospital reports, with assessment based on available physician statements and CT and MRI reports; also taken into consideration were the localisation of stroke lesions, clinical information about the presentation of stroke symptoms, and paraclinical information about associated diseases and risk factor profiles. CVD events were defined as combined endpoint including coronary events, stroke, and CV death. CV death was classified by the statistical state office based on death certificate information according to the International Statistical Classification of Disease. For all study endpoints, hospital and nursing home records including ECG, laboratory values, and pathology reports were collected. Medical records were obtained for all reported endpoints. There were no disagreements between the endpoint committee members.
Statistical analysis
Demographic data and risk factors are expressed as mean (±SD) or median and quartiles (Q1; Q3); discrete variables are given in frequency and percentages. AVC was dichotomised as present (Agatston score >0) or absent (=0). Calculations were performed for the overall population and stratified by gender. Differences in proportions were statistically evaluated using chi-square test; location measures of continuous quantities were compared using Student's t tests. Population based, age and sex related percentiles were calculated for AVC scores, using 5-year age groups. We used multivariable Cox proportional regression analysis to calculate HRs and corresponding 95% CIs for the presence of AVC, with incident coronary events, stroke and CV death as outcomes. Adjustment for potential confounders was carried out in three consecutive steps: adjustment (1) for age and gender, (2) additionally for FRS variables, and (3) model (2) + log (CAC+1). Kaplan-Meier estimates of coronary and CVD event-free time were calculated in strata defined by AVC=0 and tertiles of AVC (among those with AVC>0) as well as by a combined index according to the presence or absence of either AVC or CAC, and evaluated with a log rank of trend test, resp. a log rank test. To investigate the addictive predictive value of AVC over FRV or FRV+CAC for coronary events, stroke and CV events, Harrell's C indices, net reclassification improvement (NRI), and integrated discrimination improvement (IDI) were computed. All calculations were performed with SAS software (V.9.2, SAS Institute) and STATA/IC V.11.2 (Stata Corporation LP, College Station, Texas, USA). All analyses are to be understood as being strictly exploratory, especially as there was no adjustment for multiple testing. A value of p<0.05 indicated statistical significance.
Results
Distribution of calcification and risk factors in the study cohort
Of the 4814 participants initially recruited, 3944 (mean age 59.3±7.7 years; 53% females) were included in this analysis. The baseline characteristics of the study cohort are shown in table 1. The exclusions comprised 327 subjects who were excluded due to coronary heart disease at baseline, 11 individuals who had prior valve surgery, and 103 who had suffered prior stroke before baseline examination. In addition, baseline AVC scoring was missing in 391 subjects, and one or more covariables were missing in 38 individuals.
Baseline characteristics stratified by tertiles of aortic valve calcium and gender
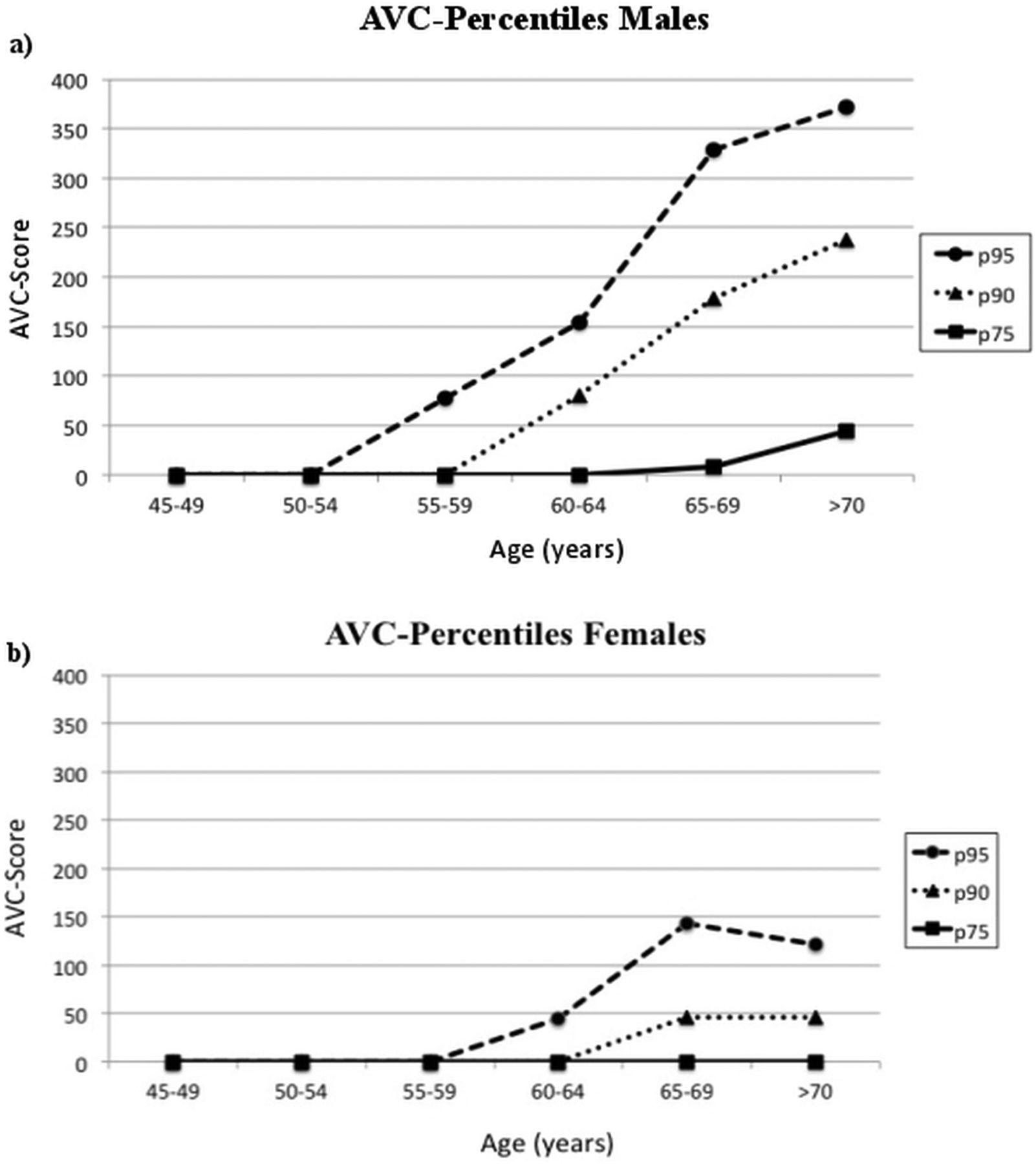
Overall 423 (10.7%) participants revealed AVC (median Agatston score 92.3, lower quartile 40.2, upper quartile 217.1) (see online supplementary table 1). Prevalence and AVC scores were higher in men compared to women (14.5% vs 7.4%, p<0.001, among those with prevalent AVC, median (Q1; Q3) 111.4 (47.6; 269.7) vs 67.0 (30.7; 145.9), for men and women, respectively). Percentiles of AVC (p75, p90 and p95) are depicted in 5-year age classes for both genders in figure 1. With increasing age, the extent of AVC increased in both sexes. Subjects with the presence and increasing extent of AVC were older, and traditional CV risk factors and CAC scores were more pronounced (all p<0.05). These findings were consistent in both sexes (table 1).

Percentiles of aortic valve calcification (AVC) (p75, p90 and p95) in 5-year age classes in (a) males and (b) females.
AVC and risk of coronary events, stroke, and CVD events
During a mean follow-up period of 9.1±1.9 years, 138 (3.5%) subjects experienced coronary events, 101 (2.6%) participants suffered stroke, and 257 (6.5%) experienced CVD events. In subjects with AVC>0 versus AVC=0 the incidence of coronary events was 8.0% versus 3.0% (p<0.001), the incidence of stroke was 4.3% versus 2.4% (p=0.02), and incidence of CVD events was 13.0% versus 5.7% (p<0.001). When stratifying by gender, men revealed higher event rates than women. Men with AVC had significantly higher frequencies of coronary events, stroke, and CVD events than men without AVC. Likewise, risks were higher in women with AVC (table 1).
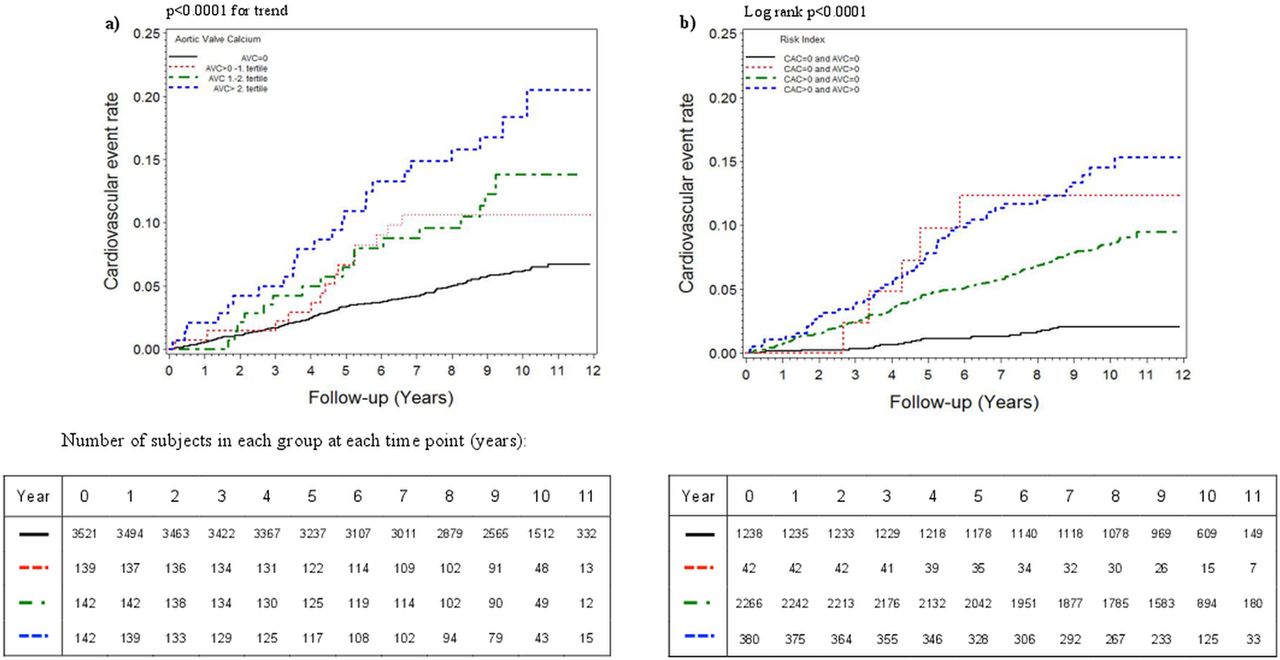
Figure 2 shows time-to-event rates for CVD events as stratified by tertiles of AVC as well as absence of AVC (see online supplementary figure 1 for coronary events as well as stroke). With increasing AVC scores both coronary and CVD events increased significantly (p<0.001). This was also found for stroke in males (p=0.03), but not in females (p=0.31). We then stratified time-to-event rates by a combined risk index consisting of the presence or absence of both AVC and/or CAC (figure 2 and online supplementary figure 1) and found that, especially in the presence of CAC, the incidence of all observed events increased significantly (p<0.001). This finding persisted after adjustment for age, gender, and traditional risk factors (table 2)⇓⇓.
Cox regression analysis for the association of a combined risk index consisting of presence of both AVC and/or CAC compared to absence of AVC and CAC with (a) coronary events, (b) stroke events, and (c) CVD events

{kind=link}
{kind=link}
Time-to-event rates for cardiovascular disease (CVD) events as stratified by tertiles of aortic valve calcification (AVC) as well as absence of AVC (a) and by a combined risk index consisting of presence and/or absence of both AVC and/or coronary artery calcification (CAC) (b).
Among 394 subjects in the high CAC category (score ≥400), those with AVC in the upper tertile were at increased hazard both of coronary events (k=53 events, HR 2.27, 95% CI 1.19 to 4.33; p=0.013) and CVD events (k=83, HR 2.26, 95% CI 1.31 to 3.88; p=0.003) as compared to those with less AVC. Both analyses are fully adjusted for FRV. The number of stroke events (k=26) in this CAC category does not suffice for likewise adjusted calculation.
After adjustment for age and sex (table 3, model 1), increasing AVC scores were a strong predictor of coronary and CVD events, but not of stroke. After adjustment for traditional CV risk factors (table 3, model 2), these risks were attenuated, but the 3rd tertile of AVC remained independently associated with coronary events (HR 2.21, 95% CI 1.28 to 3.81) and CVD events (HR 1.67, 95% CI 1.08 to 2.58). However, after further adjustment for CAC score (table 3, model 3), the HRs for all endpoints diminished substantially across AVC tertiles, demonstrating only a borderline association without reaching significance.
Cox regression analysis for the association of AVC tertiles compared to AVC=0 with (a) coronary events, (b) stroke, and (c) CVD events
Predictive value of AVC
When investigating the predictive ability in discriminating persons with events from those without, we observed no sizable improvement of Harrell's C by AVC over Framingham risk factors (coronary events: Harrell's C increased from 0.716 to 0.726, p=0.09; CVD events: from 0.722 to 0.726, p=0.099; stroke: from 0.726 to 0.728, p=0.58). Similar results were observed when AVC was added to a model with Framingham risk factors and CAC (for coronary events: from 0.744 to 0.744, p=0.89; for CVD events: from 0.759 to 0.759, p=0.99; for stroke: from 0.744 to 0.745, p=0.67) (see online supplementary figure 2). This message was confirmed after calculation of IDI and NRI for the according models and endpoints (table 4).
NRI and IDI for the combined assessment of traditional risk markers, AVC, and CAC in predicting coronary events, stroke, and CVD events
Discussion
This population based study with participants free of known coronary artery disease at baseline and at 9-year follow-up shows that calcific aortic valve disease—a measure of subclinical atherosclerosis—is associated with coronary events and stroke as well as CVD events in the general population, whereas assessment of AVC in addition to Framingham risk factors and CAC does not improve CV risk prediction.
Because of its overlap in risk factors of CVD, AVC is suspected to be associated with risk of CV events.8 The observed association of AVC with coronary atherosclerosis—namely CAC16—supports this hypothesis, as CAC is a marker of coronary atherosclerotic plaque burden17 and is a significant addition over traditional risk factors when predicting CV events.9 ,18 ,19 The association of AVC with CAC may be caused by their equal risk factors and partially similar pathophysiologic pathway.2 ,3 ,16
Our study confirms these findings as we found that AVC is associated with coronary and CVD events after adjusting for CVD risk factors; subjects with high scores of AVC had a 2.2-fold risk for a coronary event compared to those without calcification of the aortic valve. These associations were independent of age, gender, and Framingham risk factors. Furthermore, we found increased event rates in subjects who revealed both AVC and CAC in the respective highest category, with doubled hazard estimates compared to absent AVC and highest CAC.
These findings may indicate an important role of AVC in CV event prediction, in addition to CAC. Information about the extent of subclinical atherosclerosis in different vascular beds leads to better prediction of CV morbidity and mortality than estimates based solely on traditional risk factors.1 ,8 ,9 ,19–22 However, the contribution of two different measures of subclinical atherosclerosis, namely CAC and AVC, to risk prediction differs. Besides improving coronary risk stratification in addition to traditional risk factors,9 ,18 ,19 CAC seems to have a similar role for risk prediction of stroke.22 In the present study, these findings were confirmed in a comparable dimension. Likewise, an association of AVC with traditional atherosclerosis risk factors has been described in the literature,3 ,23 ,24 with an increased risk for coronary events and stroke1 ,8 after adjustment for CV risk factors. Whether AVC improves CV risk prediction beyond Framingham risk categorisation, however, has not been investigated so far. For the first time, our study investigated the predictive role of AVC burden for these endpoints in addition to CV risk factors and CAC in a population-based setting free of known coronary artery disease at baseline.
While the prevalence and extent of AVC was associated with a higher incidence of coronary events and stroke as well as CVD events, independently of traditional CV risk factors, AVC only marginally improved coronary risk prediction over Framingham risk factors. This contrasts with the ability of CAC to improve prediction of coronary risk in addition to traditional CV risk factors.9 ,18 ,19 This finding may be explained by CAC being a marker focused on coronary atherosclerosis. However, adding AVC to CV risk factors did not contribute to the prediction of stroke as well, again contrary to CAC.22 Furthermore, when including AVC in a model containing both CV risk factors and CAC, it becomes obvious that CAC outperforms AVC for the prediction of all CV event types.
We can only speculate on the reasons for the lower predictive ability of AVC compared to CAC. Risk factor influences regarding the two different vascular beds may differ considerably, with systemic hypertension and diabetes mellitus frequently noted as being most important in the development of calcific aortic valve lesions,23 ,24 but not smoking. However, generally valve atherosclerosis is encountered earlier than coronary atherosclerosis.25 Atherosclerosis is a diffuse process that may affect different vascular beds with considerable overlap between coronary, cerebrovascular and peripheral arterial disease.26 It is possible that due to its early occurrence and the high prevalence of metabolic syndrome, the prevalence of AVC limits its discriminatory predictive power.
Taking into account our results, which show that AVC is an independent predictor of coronary and CVD events, consideration for prompt medical therapy may be warranted to retard the atherosclerosis process when AVC is present. However, in daily clinical practice, echocardiography is more frequently performed in patients than cardiac CT due to reasons of availability, radiation exposure, and cost. Detection of degenerative aortic valve disease by assessing the prevalence of AVC can easily be performed by echocardiography. Walsh et al27 demonstrated that both diagnostic tools provide a high degree of accuracy and reproducibility of AVC, with a higher degree of sensitivity provided by echocardiography but with less specificity than cardiac CT.
Elevated levels of AVC not only provide evidence of advanced atherosclerosis in addition to CAC, but in the presence of elevated levels of AVC, comorbidities seem to be associated with a greater risk of coronary and CV events.
Strengths and limitations
The strength of our study is the population based design with approximately 4000 participants without selection of the cohort. Traditional CV risk factors were measured using highly standardised protocols, and AVC was quantified using a reproducible, established method.2 ,8 ,15 All measurements were conducted in a well controlled study environment with strict adherence to standards and quality control measures. The detailed information on known and candidate CV risk factors allowed an extensive control of confounding.
Since our study was performed for the primary purpose of CAC scoring, AVC was not a pre-specified variable in the Heinz Nixdorf Recall Study. Therefore CT scans were analysed retrospectively. However, the relative ease of identifying AVC during a standard CAC scan, without requiring additional scanning, is a potential advantage as it can be a good estimate of the presence and extent of overall calcific atheroma burden.8 AVC was influenced by almost all of the traditional risk factors, suggesting this may be just another manifestation of CV atherosclerosis. Second, only baseline risk factor profiles were included as covariates, and changes in profiles were not evaluated. However, participants and treating physicians were blinded to CAC [coronary artery calcification] CT results to avoid bias in decisions about medical therapy or change of lifestyle. Clinical trials, which test whether modification of therapy determined by the degree of CAC or AVC is justified by improved outcome, are needed. Because our study was conducted in a predominantly Caucasian population, generalisation to other ethnic groups remains uncertain.
Conclusion
In the general population, AVC was associated with incident coronary events and stroke independent of traditional CV risk factors. However, AVC fails to improve CV event prediction over Framingham risk factors and CAC.
Key messages
What is already known about this subject?
-
Aortic valve calcification (AVC) is associated with risks of coronary and cardiovascular events beyond those predicted by traditional risk factors. However, whether AVC adds to cardiovascular (CV) risk prediction beyond Framingham risk factors and coronary artery calcification (CAC) score has not been evaluated in a population based setting.
What does this study add?
-
In a study on a large, unselected, population based cohort, which assessed the prevalence of signs of subclinical coronary atherosclerosis, in addition to CV risk factors, AVC was associated with incident coronary and CV events independent of Framingham risk factors. However, AVC did not improve CV event prediction over traditional CV risk factors and CAC.
How might this impact on clinical practice?
-
The association of AVC with incident coronary events and stroke independent of traditional CV risk factors suggests medical therapy may be warranted to retard the atherosclerosis process when AVC is present.
Acknowledgments
We thank the Heinz Nixdorf Foundation Germany, for their generous support of this study. This study is also supported by the German Ministry of Education and Science (BMBF), and the German Aerospace Center (Deutsches Zentrum für Luft- und Raumfahrt, DLR), Bonn, Germany. We thank Professor K Lauterbach (Department of Health Economy and Epidemiology, University of Cologne, Germany) for his valuable contributions in an earlier phase of the study. We acknowledge the support of the Sarstedt AG & Co. (Nümbrecht, Germany) concerning laboratory equipment. We are indebted to all study participants and both to the dedicated personnel of the study centre of the Heinz Nixdorf Recall study and the EBT-scanner facilities and to the investigative group, in particular to U Roggenbuck, U Slomiany, EM Beck, A Öffner, S Münkel, S Schrader, R Peter, and H Hirche. Advisory board: Meinertz T, Hamburg, Germany (Chair); Bode C, Freiburg, Germany; de Feyter PJ, Rotterdam, Netherlands; Güntert B, Halli T, Austria; Gutzwiller F, Bern, Switzerland; Heinen H, Bonn, Germany; Hess O, Bern, Switzerland; Klein B, Essen, Germany; Löwel H, Neuherberg, Germany; Reiser M, Munich, Germany; Schmidt G, Essen, Germany; Schwaiger M, Munich, Germany; Steinmüller C, Bonn, Germany; Theorell T, Stockholm, Sweden; Willich SN, Berlin, Germany.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online figure 1
- Data supplement 2 - Online figure 2
- Data supplement 3 - Online table 1
Footnotes
-
Contributors All of the authors meet all of the following conditions, substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; drafting the article or revising it critically for important intellectual content; final approval of the version to be published.
-
Competing interests None.
-
Patient consent Obtained.
-
Ethics approval The study was approved by our institutional ethics committees.
-
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- PostScript