Article Text

Abstract
Objective Transcatheter aortic valve replacement (TAVR) improves clinical symptoms in most patients with severe aortic stenosis (AS). However, some patients do not benefit from the symptom-reducing effects of TAVR. We assessed the predictors and clinical outcomes of poor symptomatic improvement (SI) after TAVR.
Methods A total of 1749 patients with severe symptomatic AS undergoing transfemoral TAVR were evaluated using the Japanese multicentre TAVR registry. Poor SI was defined as readmission for heart failure (HF) within 1 year after TAVR or New York Heart Association (NYHA) class ≥3 after 1 year. A logistic regression model was used to identify predictors of poor SI. One-year landmark analysis after TAVR was used to evaluate the association between poor SI and clinical outcomes.
Results Among the overall population (mean age, 84.5 years; female, 71.3%; mean STS score, 6.3%), 6.6% were categorised as having poor SI. Atrial fibrillation, chronic obstructive pulmonary disease, Clinical Frailty Scale ≥4, chronic kidney disease and moderate to severe mitral regurgitation were independent predictors of poor SI. One-year landmark analysis demonstrated that poor SI had a higher incidence of all-cause death and readmission for HF compared with SI (p<0.001). Poor SI with preprocedural NYHA class 2 had a worse outcome than SI with preprocedural NYHA class ≥3.
Conclusions Poor SI was associated with worse outcomes 1 year after the procedure. It had a greater impact on clinical outcomes than baseline symptoms. TAVR may be challenging for patients with many predictors of poor SI.
Trial registration number This registry, associated with the University Hospital Medical Information Network Clinical Trials Registry, was accepted by the International Committee of Medical Journal Editors (UMIN-ID: 000020423).
- aortic valve stenosis
- transcatheter aortic valve replacement
- heart failure
Data availability statement
No data are available. The data in this research are deidentified participant data. The data, materials will not be available to researchers for purpose of reproducing the results or replicating the procedure.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known about this subject?
The independent predictors of a poor improvement in quality of life after transcatheter aortic valve replacement (TAVR) are age, frailty status, comorbidities and procedural complications.
In addition, a lesser improvement in exercise capacity is associated with an increased risk of mortality and cardiovascular events at follow-up.
What does this study add?
Focusing only on preprocedural factors, the following were particularly associated with poor symptomatic improvement (SI) after TAVR: atrial fibrillation, chronic obstructive pulmonary disease, Clinical Frailty Scale ≥4, chronic kidney disease and moderate to severe mitral regurgitation.
Poor SI, which is a simple standard for evaluating readmission for heart failure within 1 year and postprocedural New York Heart Association class, was associated with worse outcomes 1 year after the procedure and had a greater impact on clinical outcomes than baseline symptoms.
How might this impact on clinical practice?
The predictors of poor SI should be considered when deciding to proceed to TAVR as well as for preprocedure informed consent of patients and their families.
Introduction
Many studies have demonstrated survival and quality-of-life benefits for transcatheter aortic valve replacement (TAVR) regardless of the surgical risk.1–3 However, certain non-responders have poor symptomatic improvement (SI) after TAVR. Especially in the very elderly undergoing TAVR, prolonged survival alone without improvement of symptoms is an undesirable outcome. In addition, with the recently expanded indication for TAVR in lower-risk patients and for relatively active patients, a significant improvement in their symptoms is essential.
However, predicting poor SI after TAVR is challenging. Many previous studies have analysed predictors of death or readmission for heart failure (HF). Certain studies have focused on exercise capacity or quality of life before and after TAVR and have analysed predictors of their improvement.4 5 However, a few studies have focused solely on patients’ symptomatic status. The New York Heart Association (NYHA) functional classification is a grading system for HF. It focuses on exercise capacity and symptomatic status.6 7 We used the NYHA functional classification and readmission for HF to define poor SI and analysed predictors and subsequent clinical outcomes.
Methods
Study population
We obtained data from the Optimised transCathEter vAlvular Intervention-Transcatheter Aortic Valve Implantation (OCEAN-TAVI) registry from October 2013 to May 2017. The OCEAN-TAVI is a prospective, multicentre, observational registry of patients with severe aortic stenosis (AS). These patients underwent TAVR using the Edwards Sapien XT/Sapien 3 Transcatheter Heart Valve (Edwards Lifesciences, Irvine, California, USA) or the Medtronic CoreValve/Evolut R Revalving System (Medtronic, Minneapolis, Minnesota, USA) at 14 collaborating hospitals in Japan.8 The indications for TAVR were determined based on the clinical consensus of a multidisciplinary team that included cardiac surgeons, interventional cardiologists, anaesthesiologists and imaging specialists. All patients provided written informed consent prior to participation. Patients or the public were not involved in the design, or conduct, or reporting, or dissemination plans of our research.
For the purpose of our study, we included all patients with severe AS who underwent transfemoral TAVR and excluded; (1) patients with pre-procedure NYHA class (NYHA-pre) 1, (2) patients who died within 1 year of the procedure, and (3) patients whom we were unable to follow and assess their NYHA class 1 year after TAVI (NYHA-1y).
Definition
Preprocedural and postprocedural functional statuses were graded according to the NYHA functional classification.6 7 Poor SI was defined as readmission for HF within 1 year after TAVR or NYHA-1y ≥3 as the event of readmission for HF overlaps with the NYHA functional classification. Readmission for HF was defined as new-onset or gradually worsening signs and symptoms of HF requiring urgent readmission and treatment. The diagnosis of HF was left to the discretion of the clinicians in each participating hospital. Patients were divided into two groups: patients with SI after TAVR and those with poor SI. Baseline characteristics and clinical outcomes were compared between the SI and poor SI groups. The scores of the Clinical Frailty Scale (CFS) were determined by a trained medical professional according to the Canadian Study of Health and Aging grading criteria.9 10 All CFS stages were calculated by face-to-face assessments with patients and families to determine the baseline frailty status prior to TAVR. The CFS ranged from 1 (very fit) to 9 (terminally ill). Procedural outcomes and complications were defined according to the Valve Academic Research Consortium-2 criteria.11 In addition, a further subanalysis dichotomised by NYHA-pre (NYHA-pre 2 or ≥3) was performed to separate the overall population into four groups: SI with NYHA-pre 2, poor SI with NYHA-pre 2, SI with NYHA-pre ≥3 and poor SI with NYHA-pre ≥3.
Echocardiography
All patients underwent standard two-dimensional B-mode and Doppler transthoracic echocardiography before and after the procedure. Experienced echocardiographers in each hospital measured the conventional parameters and the severity of valvular regurgitation. Low-flow low-gradient (LFLG) AS was defined as a Stroke Volume Index ≤35 mL/m2 and mean aortic pressure gradient <40 mm Hg.12
Statistical analysis
All statistical analyses were performed using the Statistical Package for the Social Sciences software V.25 (SPSSA). Continuous variables were expressed as median (IQR), and categorical data were expressed as the number of cases (percentage of the total). Comparisons between the two groups, SI and poor SI, were performed using the Mann-Whitney U test for continuous covariates and the χ2 test for categorical covariates. Cumulative incidences of all-cause death or readmission for HF since the first postprocedural year were estimated using a 1-year landmark analysis via the Kaplan-Meier method. Cases of death within 1 year were excluded and the difference between groups was tested using a log-rank test. Logistic regression analysis was used to examine the univariable associations of certain variables with poor SI. Multivariable analysis, including all variables with a p value of less than 0.05, in the univariable analysis, was performed to identify the predictors of the non-responders. Statistical significance was defined as a p value of less than 0.05.
Results
After applying the exclusion criteria, we identified a total of 1749 patients who underwent transfemoral TAVR. Among them, there were 1633 patients with SI and 116 patients with poor SI. Figure 1 shows the distribution of NYHA-pre, NYHA-1y and readmission for HF within 1 year after TAVR.

Distribution of preprocedural and postprocedural New York Heart Association (NYHA-pre) classes and postprocedural readmission for heart failure (HF) each number shows the number of patients with a pair of scores for the NYHA class before and 1 year (NYHA-1y) after transcatheter aortic valve replacement (TAVR) or readmission for HF within 1 year after TAVR. The overall population was divided into two groups: symptomatic improvement (SI), (green +blue) and a poor SI (red +yellow) or four groups, with the subgroups of SI with NYHA-pre 2 (blue), SI with NYHA-pre ≥3 (green), poor SI with NYHA-pre 2 (yellow) and poor SI with NYHA-pre ≥3 (red).
The baseline characteristics of SI and poor SI are described in table 1. Significant differences were observed in haemoglobin, (11.3 (10.2–12.5) vs 10.7 (9.6–11.9) g/dL, p<0.001); serum albumin ≤3.5 g/dL (26.0% vs 37.9%, p=0.005); chronic kidney disease (CKD), (69.3% vs 87.1%, p<0.001); chronic obstructive pulmonary disease (COPD), (12.9% vs 19.8%, p=0.035); CFS ≥4 (55.8% vs 76.7%, p<0.001); peripheral arterial disease, (9.1% vs 14.7%, p=0.050); atrial fibrillation (AF), (19.9% vs 42.2%, p<0.001); brain natriuretic peptide, (247.7 (112.0–531.4) vs 369.2 (160.8–604.7) pg/mL, p<0.001); LFLG AS (8.9% vs 19.5%, p<0.001); E/e’ ratio (19.5 (15.2–25.3) vs 20.9 (16.1–28.8), p=0.065); preprocedural moderate to severe mitral regurgitation (MR), (10.2% vs 25.9%, p<0.001); preprocedural moderate to severe tricuspid regurgitation (TR), (6.2% vs 17.2%, p<0.001); and the Society of Thoracic Surgery Predicted Risk of Mortality, (6.2 (4.4–8.8) vs 7.8 (5.0–12.6), p<0.001). In patients with preprocedural moderate to severe MR, MR improved after TAVR in 106 of 167 patients with SI and 14 of 30 patients with poor SI. The percentage of MR improvement tended to be higher in SI compared with poor SI (p=0.08). The procedural characteristics and in-hospital outcomes are presented in table 2. There were no significant differences between the two groups in the type of bioprosthesis valve used. The in-hospital incidence of acute kidney injury, new pacemaker implantation and stroke was significantly higher in patients with poor SI than in those with SI. Predictors of poor SI were assessed using a logistic regression analysis and identified as follows: AF, COPD, anaemia, serum albumin ≤3.5 g/dL, CFS ≥4, CKD, LFLG AS, left ventricular ejection fraction (LVEF) ≤50%, preprocedural moderate to severe MR and preprocedural moderate to severe TR in the univariable analysis. AF, COPD, CFS ≥4, CKD and preprocedural moderate to severe MR remained as predictors after multivariate analysis (table 3).
Baseline characteristics of SI and poor SI
Procedural characteristics and in-hospital outcomes of SI and poor SI
Predictors of poor SI
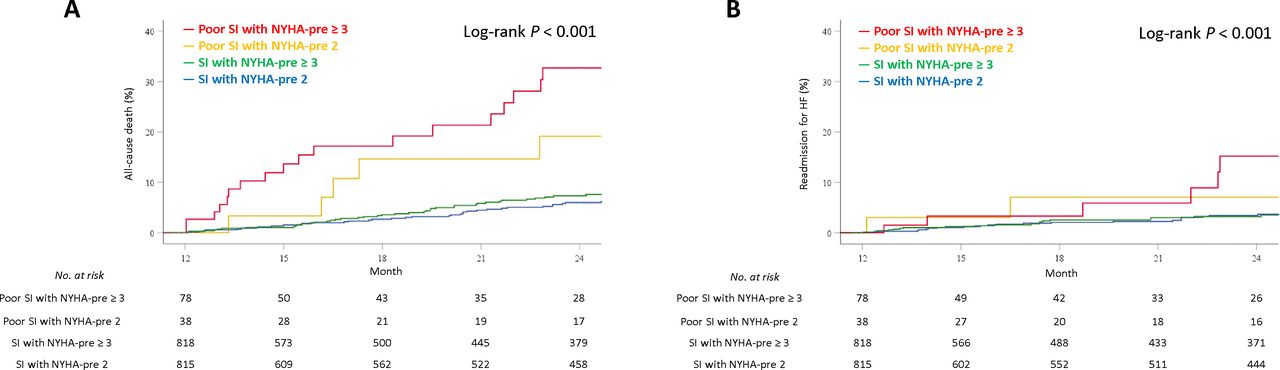
A 1-year landmark analysis of Kaplan-Meier curves according to responders and non-responders is shown in figure 2. Significant differences between the two groups were observed in the cumulative incidence of all-cause death and readmission for HF (p<0.001). After further dichotomisation by NYHA-pre, the cumulative incidences of all-cause death and readmission for HF were gradually significantly higher in the following order: SI with NYHA-pre 2, SI with NYHA-pre ≥3, poor SI with NYHA-pre 2 and poor SI with NYHA-pre ≥3 (figure 3).

Cumulative incidence of all-cause death and readmission for heart failure from the first postprocedural year according to symptomatic improvement (SI) time-to-event curves are shown from 1 to 2 years for all-cause death (A) and readmission for heart failure (B). Event rates were calculated using the Kaplan-Meier method and compared with the log-rank test.
{kind=link}
{kind=link}
{kind=link}
Cumulative incidence of all-cause death and readmission for heart failure from the first postprocedural year according to preprocedural New York Heart Association (NYHA) functional class and symptomatic improvement (SI) time-to-event curves are shown from 1 to 2 years for all-cause death (A) and readmission for heart failure (B). Event rates were calculated using the Kaplan-Meier method and compared with the log-rank test.
Discussion
We found three primary results using the Japanese multicentre TAVR registry. First, 6.6% of patients undergoing TAVR showed a poor SI. Second, AF, COPD, CFS≥4, CKD and preprocedural moderate to severe MR were associated with a poor SI. Third, a poor SI was associated with an increased risk of all-cause death and readmission for HF after TAVR.
Previous studies using the 6 min walk test (6MWT), the Kansas City Cardiomyopathy Questionnaire overall summary (KCCQ-OS) or the event of readmission for HF showed that independent factors associated with poor improvement of these outcomes were age, female sex, AF, COPD, CKD, diabetes mellitus, peripheral vascular disease, prior stroke, permanent pacemaker before TAVR, low-gradient AS, major or life-threatening bleeding and the occurrence of new-onset anaemia.4 5 13 Our results were similar to those of previous studies in that AF, COPD and CKD were also found to be independent predictors of poor SI. A meta-analysis showed that pre-existing AF was an independent predictor of all-cause mortality in patients undergoing TAVR.14 We have previously reported that pre-existing AF increased the risk of all-cause death and readmission for HF after TAVR in comparison with new-onset AF or sinus rhythm.15 COPD was associated with not only short-term and long-term mortality, but also with no improvement in functional status.16 17 COPD causes symptom to some extent even in patients with severe AS. Previous studies have reported that CKD is associated with worse outcomes in patients with AS undergoing TAVR.18–20 As CKD is a risk factor for worsening HF due to cardiorenal syndrome,21 CKD was associated with a poor SI in this study.
In our analysis, high CFS and preprocedural moderate to severe MR were found to be predictors, whereas previous reports did not identify these factors to be associated with a poor SI. In previous studies using the 6MWT or KCCQ-OS, a preprocedural short distance of 6MWT and a lower score on the KCCQ-OS were predictors of no improvement in these categories after TAVR.4 5 Furthermore, a recent study reported that frailty was associated with a deterioration in the quality of life 1 year after TAVR.22 Given that CFS represents the patient’s functional status similar to the 6MWT, KCCQ-OS or frailty score, we believe our finding that CFS was associated with a poor SI is consistent with prior studies. In this study, preprocedural moderate to severe MR was associated with a poor SI. Even though some previous studies have reported that MR, especially functional MR, decreased after TAVR,23–25 the residual MR may have contributed to left-sided HF, resulting in a poor SI.
Staging classification of AS based on the extent of cardiac damage has prognostic implications for clinical outcomes after aortic valve replacement.26 According to the classification, AF and moderate to severe MR are higher stage findings, compared with low LVEF and diastolic dysfunction. In this study, it was reasonable that higher stage findings of AF and preprocedural moderate to severe MR were independent predictors, while LVEF ≤50% and E/e’ ratio ≥14 (which estimates diastolic dysfunction) were not.
Poor improvement in exercise capacity has been reported to lead to an increased risk of mortality and cardiovascular events at follow-up.4 Similarly, in this study, a poor SI was found to have a significantly higher risk of all-cause death and readmission for HF afterward. It is interesting to note that SI with NYHA-pre ≥3 had a better outcome than poor SI with NYHA-pre 2. This suggests that SI is more important than baseline symptoms for predicting clinical outcomes.
Most patients with AS expect that TAVR will improve their symptoms. However, a dissociation between patient expectations and the predictions of physicians is a real possibility. Therefore, it is essential for both patients and physicians to discuss the expected outcomes after TAVR in the preprocedural informed consent meeting. This is where these predictors of poor SI are considered carefully. With the expanded indication of TAVR to a lower-risk subset of patients, TAVR could be considered as the first-line treatment choice for patients with AS. This would be not only for the improvement of hard endpoints (mortality and readmission for HF), but also for the improvement of other soft endpoints (symptom, quality of life, functional and cognitive performance). These issues are emerging as important challenges for TAVR. Further studies are required to precisely analyse the predictors of a poor SI, including patients with AS at a lower risk.
This study has several limitations. First, the NYHA class, which we used in the definition of a poor SI, is a subjective classification and physicians from each hospital evaluated the NYHA class. Actually, there was centre based bias among participating hospitals (online supplemental figure l). We did not include more objective measures, such as the 6MWT or the KCCQ-OS. Second, the overall patient population was elderly. Therefore, the study’s applicability to younger patients may be limited. Third, this study includes early learning curve patient dataset and more than half of all patients were implanted the older Sapien XT or Corevalve. These may have affected the results. Fourth, echocardiographic parameters were site-reported and not adjudicated in a single-core laboratory. Fifth, there were some missing data for NYHA-1y. Finally, in the 1-year landmark analysis, we did not use data from 1 year after TAVR, but the preprocedural data. The gap between them was not considered. These factors may have biased our results.
Supplemental material
Conclusion
Using the Japanese multicentre TAVR registry, baseline AF, COPD, CFS ≥4, CKD and moderate to severe MR may be one of the predictors of poor SI after TAVR. A poor SI was associated with an increased risk of all-cause death and readmission for HF from 1-year postprocedure. It had a greater impact on clinical outcomes than baseline symptoms. TAVR for patients with many predictors of a poor SI may be challenging.
Data availability statement
No data are available. The data in this research are deidentified participant data. The data, materials will not be available to researchers for purpose of reproducing the results or replicating the procedure.
Ethics statements
Patient consent for publication
Ethics approval
The study protocol was developed in accordance with the guidelines of the Declaration of Helsinki and was approved by the ethics committee of each participating hospital.
Acknowledgments
The authors thank the investigators and institutions that participated in the OCEAN-TAVI registry.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors Study conception, design, analysis and interpretation, drafting of the manuscript: NY, TS, TI, AA, HT and KH. Critical revision of the manuscript for important intellectual content: HS, KF, TN, KM, MY, NT, FY, SS, MT, HU, KT, YW, MY and KH. Responsible for the overall content as the guarantor: KH.
Funding The OCEAN-TAVI registry is supported by Edwards Lifesciences, Medtronic, Boston Scientific, Abbott Medical and Daiichi-Sankyo Company.
Competing interests MY, NT, TN, SS, KM, MT, HU, YW and KH are clinical proctors for Edwards Lifesciences and Medtronic. HS and KT are clinical proctors for Edwards Lifesciences.
Provenance and peer review Not commissioned; externally peer reviewed.