Article Text

Abstract
Objective: To determine the clinical effect of dietary supplementation with low-dose ω-3-polyunsaturated fatty acids on disease activity and endothelial function in patients with systemic lupus erythematosus.
Methods: A 24-week randomised double-blind placebo-controlled parallel trial of the effect of 3 g of ω-3-polyunsaturated fatty acids on 60 patients with systemic lupus erythematosus was performed. Serial measurements of disease activity using the revised Systemic Lupus Activity Measure (SLAM-R) and British Isles Lupus Assessment Group index of disease activity for systemic lupus erythematosus (BILAG), endothelial function using flow-mediated dilation (FMD) of the brachial artery, oxidative stress using platelet 8-isoprostanes and analysis of platelet membrane fatty acids were taken at baseline, 12 and 24 weeks.
Results: In the fish oil group there was a significant improvement at 24 weeks in SLAM-R (from 9.4 (SD 3.0) to 6.3 (2.5), p<0.001); in BILAG (from 13.6 (6.0) to 6.7 (3.8), p<0.001); in FMD (from 3.0% (−0.5 to 8.2) to 8.9% (1.3 to 16.9), p<0.001) and in platelet 8-isoprostanes (from 177 pg/mg protein (23–387) to 90 pg/mg protein (32–182), p = 0.007).
Conclusions: Low-dose dietary supplementation with ω-3 fish oils in systemic lupus erythematosus not only has a therapeutic effect on disease activity but also improves endothelial function and reduces oxidative stress and may therefore confer cardiovascular benefits.
Statistics from Altmetric.com
Among the clinical challenges of systemic lupus erythematosus (SLE) one of the most compelling is the high incidence of atherosclerosis in young women. In 1976, Urowitz et al,1 reported the bimodal mortality pattern that occurs in SLE, with early deaths attributable to active disease and infection, and late deaths (comprising 45%) attributed to cardiovascular disease (CVD). This finding has been confirmed by numerous subsequent epidemiological studies providing further evidence for accelerated and premature atherosclerosis in SLE.2–4
Many studies have also confirmed the presence of subclinical vascular disease in SLE using ultrasound measurement of carotid plaque,5 isotope myocardial perfusion scanning6 and coronary calcification on computed tomography.7 We have previously shown that subclinical endothelial dysfunction and impaired large and small arterial compliance exists in patients with SLE, which may in part be due an alteration in microvascular haemodynamics.8 9
Pioneering studies in Greenland Eskimos almost 30 years ago suggested that ingestion of ω-3-polyunsaturated fatty acids (n-3 PUFAs) conveyed protection against CVD.10 A recent meta-analysis of n-3 PUFAs in coronary artery disease indicated overall benefit in the reduction of non-fatal myocardial infarction, fatal myocardial infarction and sudden death.11 Furthermore n-3 PUFAs have been shown to improve endothelial function in disease states associated with atherosclerosis.12–17
In murine models of SLE, modulation of fatty acid metabolism by increasing n-3 PUFAs intake can result in a therapeutic effect.18–21 High-dose (20 g daily) n-3 PUFAs has been shown to improve clinical features of SLE and our group has also previously shown a reduction in SLE disease activity with low-dose n-3 PUFAs.22
To test the hypothesis that supplementation with n-3 PUFAs in patients with SLE will not only provide a therapeutic effect but will also confer vascular protection through an improvement in endothelial function and reduction in oxidative stress, we undertook a randomised double-blind placebo-controlled dietary intervention trial.
PATIENTS AND METHODS
Patients
Patients fulfilling the ACR criteria for the diagnosis of SLE23 were recruited from the lupus research group at Queen’s University Belfast (QUB). This database contains the details of over 350 patients with SLE from throughout Northern Ireland. A total of 126 of these patients fulfilled the inclusion and exclusion criteria for this study and were then invited by post to participate. The patients with SLE were then studied consecutively as each patient consented to be involved.
Patients were excluded if they had any of the following: diabetes mellitus; hypertension (defined as greater than 140/80 mmHg on three separate readings); significant pulmonary, hepatic or renal disease (defined as organ involvement requiring high-dose corticosteroids or immunosuppressant therapy); typical angina or myocardial infarction; cerebrovascular disease or history of transient ischaemic attack; use of antihypertensive, oral hypoglycaemic or lipid lowering agent (in the last 3 months); glucocorticoids equivalent to greater than 10 mg prednisolone daily; all pregnant or lactating women. The choice of these exclusion criteria was to ensure that any effect of fish oils in SLE would not be missed by including confounding factors (diabetes, hypertension, glucocorticoids) that are known to influence endothelial function.
All subjects gave written informed consent to take part in the study, which was approved by the QUB Local Research Ethics Committee and conducted according to the Declaration of Helsinki. All subjects were asked to stop all vitamin and mineral supplements, including fish oils, at least 6 weeks before commencing the study.
Plan of study
The patients were randomised to take Omacor (Solvay Pharmaceuticals, Brussels, Belgium) or placebo for a total of 24 weeks. Randomisation occurred off-site by an independent body (Victoria Pharmaceuticals, Belfast, Northern Ireland). The Omacor was four capsules per day, providing 1.8 g eicosapentanoic acid (EPA) and 1.2 g docosahexanoic acid (DHA). The placebo was four identical capsules per day containing olive oil to provide a similar calorie intake.
Assessments
Patients were assessed at baseline, week 12 and week 24. The patients were asked to abstain from food, alcohol, nicotine and caffeine containing products for the 12 h preceding attendance for study. All clinical assessments and vascular measures were performed by the same researcher (SW) who was blinded to study medication. In all patients, a detailed clinical interview was conducted to ascertain presence of conventional cardiovascular risk factors. An electrocardiogram and full screening blood tests were performed, including plasma homocysteine concentration, fasting lipid profile, serum antinuclear antibody levels, anti-dsDNA antibodies, anticardiolipin antibodies and complement C3 and C4 levels. The assays used standardised conditions employed in recent SLE studies in Belfast.8 22 Disease activity was assessed using SLAM-R (Systemic Lupus Activity Measure-Revised)24 and British Isles Lupus Assessment Group index of disease activity for SLE (BILAG)25 in which we assigned the numerical values 4, 3, 2, 1, 0 to correspond to the alphabetical scores A, B, C, D and E respectively.
Organ damage was assessed using the American College of Rheumatology/Systemic Lupus International Collaborating Clinics (ACR/SLICC) score.26 Compliance was assessed by capsule return and measurement of platelet membrane fatty acids.
Platelet assays
Platelets were isolated and prepared as previously described.27
Platelet 8-isoprostanes
Platelet production of 8-epi prostaglandin F2α (8-epi PGF2α) was measured as previously described.28
Platelet membrane fatty acids
The fatty acid composition was determined with a gas chromatograph (Finnigan Trace GC Ultra, Thermo Electron Corporation, Milan, Italy) with a flame ionisation detector on a 30 m × 0.32 mm internal diameter, fused silica column (Famewax, Restek Corporation, Pennsylvania, PA, USA). The fatty acids were identified by comparison with commercial standards (Marine oil FAME mix, Restek, Corp.) and quantified by peak area. The chromatograms were analysed using Chrom-card software (Thermo Electron Corporation, Milan, Italy), on a PC connected to the GC by a serial cable. The relative amounts for each peak were reported as a percentage of the total peak area.
Vascular measures
Flow-mediated dilation (FMD) of the right brachial artery and diastolic shear stress (DSS) during reactive hyperaemia were measured as previously described in detail.8 In brief, the brachial artery was scanned longitudinally in the anteromedial plane 2–10 cm above the antecubital fossa. A resting scan was taken for 2 min. A tourniquet located on the forearm immediately below the antecubital fossa was inflated to 50 mmHg above the patients’ systolic blood pressure for 4.5 min. Brachial artery diameter measurements were recorded for 2 min after cuff release. The subject then rested for at least 10 min before measuring endothelium independent dilation (EID), 3 min after 500 μg sublingual glyceryl trinitrate (GTN). Pulsed Doppler velocity waveforms were recorded for 15 s immediately after cuff release using a carrier frequency of 6.0 MHz, an insonation angle of 70° and a 1.5 mm gate range in the centre of the artery. Hyperaemic DSS was obtained from the following equation: DSS = 8×μ×(MDV/DBL),29 where μ = blood viscosity, MDV = mean diastolic velocity and DBL = brachial artery baseline diameter.
Outcome measures
The primary outcome was endothelial function as measured by FMD. The secondary outcomes were disease activity (SLAM-R and BILAG) and platelet 8-isoprostanes.
Statistics applied
Sample size was based on primary outcome of FMD. Under an assumption of a true 5% differential change in FMD between the two groups and a SD of 6.5% then using a 5% significance level and a two-tailed hypothesis indicated that we needed 27 recruits per group to achieve 80% power. Sixty patients were recruited to allow for a 10% drop-out rate. All statistical analysis was performed using SPSS version 14.0. Differences at baseline between groups were tested using independent samples t-test. Parametric variables are presented as mean value (SD) and differences from baseline at 12 and 24 weeks were tested using the paired samples t-test. Non-parametric results are expressed as median and range, and differences from baseline at 12 and 24 weeks were tested with the Wilcoxon signed-rank test with statistical significance set at p<0.05. The correlations between variables were determined using Pearson’s correlation coefficient and Spearman’s correlation coefficient for parametric and non-parametric variables respectively, with statistical significance set at p⩽0.01 to account for the Bonferroni principle. All analysis was based on intention-to-treat.
RESULTS
Subjects
Sixty patients with SLE were studied. Four subjects failed to complete the study, one on placebo due to personal issues, and three on fish oils due to gastrointestinal disturbance. As can be seen from table 1 there were no significant differences in the physical characteristics or drug treatments between the two groups. During the 24-week study period, eight patients in the fish oil group had an alteration to their medication (three discontinued non-steroidal anti-inflammatory drugs, two had prednisolone dose decreased, one commenced hydroxychloroquine 200 mg/day, one commenced HRT and one commenced an over-the-counter cod-liver oil preparation). In the placebo group, six patients had an alteration to their medication (two discontinued non-steroidal anti-inflammatory drugs, two commenced hydroxychloroquine 200 mg/day and two commenced glucosamine 1500 mg/day). In the patients with SLE randomised to the fish oils, there was a significantly higher erythrocyte sedimentation rate than in the placebo group (33.8 (30.3) mm/h versus 19.3 (14.0); p = 0.02), but there were no significant differences in disease activity (SLAM-R and BILAG) or organ damage (SLICC) between the two groups.
Of the 56 subjects who completed the study, 21 (38%) took all of the capsules, the remaining subjects took greater than 90% of the capsules. Compliance was also assessed by the change in platelet membrane fatty acid composition.
Platelet membrane fatty acids
In the fish oil group there was a significant decrease in the percentage arachidonic acid (AA) in the platelet cell membrane at 24 weeks (baseline percentage AA, median (range), 15.8 (0.4–23.4), versus 24-week percentage AA, 9.9 (0.5–20.0), p = 0.001); a significant increase in the percentage docosahexaenoic acid (DHA) in the platelet cell membrane at 24 weeks (baseline percentage DHA, 1.2 (0.2–2.7) versus 24-week percentage DHA, 1.4 (0.3–3.2), p = 0.044), and a significant increase in the percentage eicosapentanoic acid (EPA) in the platelet cell membrane at 24 weeks (baseline percentage EPA, 0.6 (0.1–3.0) versus 24-week percentage EPA, 1.4 (0.2–3.0), p = 0.012. There were no significant changes in the platelet membrane fatty acids in the placebo group.
Platelet 8-isoprostanes
There was a significant reduction at 24 weeks in 8-isoprostane levels in the fish oil group (baseline, median (range), 177 pg/mg protein (23–387) versus 24 weeks, 90 pg/mg protein (32–182), p = 0.007) and also a significant reduction in 8-isoprostane level at 24 weeks in the placebo group (baseline, median (range), 147 pg/mg protein (3–426) versus 24 weeks, 128 pg/mg protein (3.0–376), p = 0.027.
Effect of fish oils on systemic lupus erythematosus disease activity
As can be seen from table 2, in the fish oils group there was a significant reduction in triglycerides (TG) at 24 weeks, baseline mean (SD), 1.1 (0.4) mmol/l versus 24 weeks, 0.8 (0.3) mmol/l, p = 0.001. There was no significant change in the other laboratory measurements in the fish oil or placebo group.
In the fish oil group there was a significant reduction in SLAM-R at 12 weeks and 24 weeks; baseline, mean (SD), 9.4 (3.0) versus 12 weeks 7.4 (3.1), p = 0.009 and versus 24 weeks 6.3 (2.5), p<0.001. There was no significant difference in SLAM-R with placebo (fig 1). Within the SLAM-R, there was a significant reduction in the individual scores at 12 weeks for constitutional symptoms and joints and at 24 weeks there was a significant reduction in constitutional symptoms, integument, neuromotor and joint scores, as shown in fig 1.

In the fish oil group there was a significant reduction in BILAG at 12 weeks and 24 weeks; baseline, mean (SD), 13.6 (6.0) versus 12 weeks 9.1 (4.0), p = 0.001 and versus 24 weeks 6.7 (3.8), p<0.001. There was no significant difference in BILAG with placebo (fig 2). Within the BILAG, there was a significant reduction in the individual scores at 12 weeks for general symptoms, musculoskeletal and cardiorespiratory and at 24 weeks there was a significant reduction in general symptoms, cutaneous, musculoskeletal, cardiorespiratory and vasculitis scores as shown in fig 2. There was a strong positive correlation between SLAM-R and BILAG at week 24 in the fish oil group, rs = 0.71; p<0.001. There was no correlation between SLAM-R or BILAG and platelet membrane fatty acids or 8-isoprostanes.

Vascular measures
Conventional cardiovascular measures
There were no significant differences in systolic blood pressure, diastolic blood pressure or heart rate in the fish oils group. As shown in table 2, in the placebo group, both systolic and diastolic blood pressures were significantly reduced at 24 weeks; systolic 124.4 (14.8) mmHg versus 119.2 (13.8) mmHg, p = 0.05 and diastolic 74.0 (8.5) mmHg versus 71.1 (10.7) mmHg, p = 0.04.
Flow-mediated dilation
There was no significant difference in brachial artery diameter at week 12 or week 24 in either group, (median (range) brachial artery diameter (cm), placebo at baseline, 0.35 (0.28–0.51), at week 12, 0.34 (0.29–0.51); p = 0.79, at week 24, 0.34 (0.26–0.50); p = 0.25 and fish oil group at baseline 0.35 (0.27–0.47), at week 12, 0.35 (0.26–0.48); p = 0.60, at week 24, 0.35 (0.26–0.49); p = 0.57.
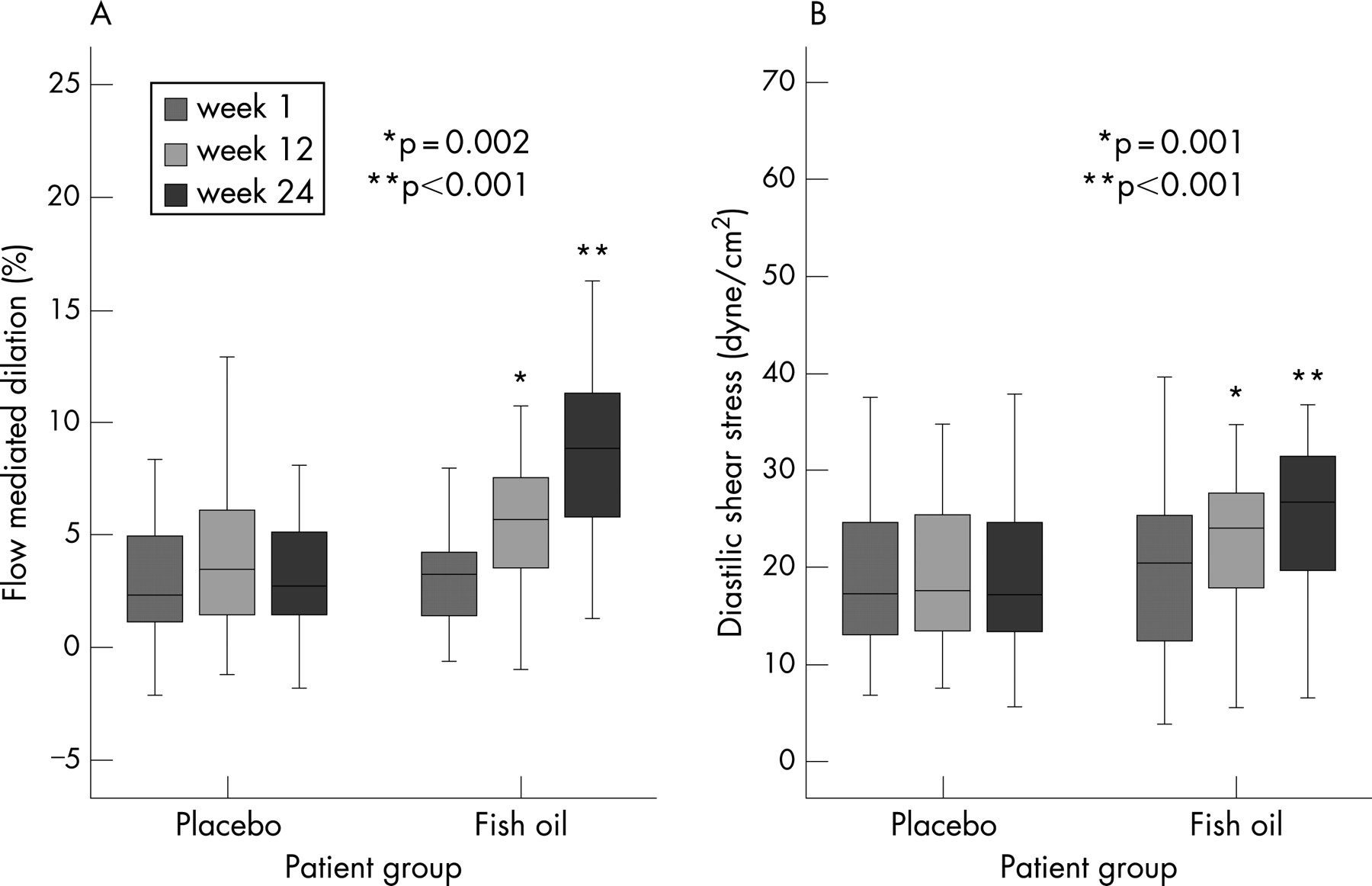
FMD was significantly increased from baseline at week 12 and week 24 in the fish oil group; median (range), baseline FMD 3.0% (−0.5 to 8.2) versus 12 week FMD 5.7% (−1.0 to 10.8); p = 0.002 and versus 24 week FMD 8.9% (1.3 to 16.9); p<0.001. There was no significant change in FMD at 12 or 24 weeks in the placebo group (fig 3).
There was no significant difference in endothelium independent dilation (percentage EID) in response to GTN in either group at week 12 or week 24 (median (range) percentage EID, placebo at baseline, 16.4 (6.0–31.4), at week 12, 16.8 (8.7–29.9); p = 0.84, at week 24, 17.0 (5.9–29.4); p = 0.19 and fish oil group at baseline 15.1 (7.0–23.1), at week 12, 14.2 (5.7–24.7); p = 0.82, at week 24, 13.9 (5.8–22.0); p = 0.31.
DSS was significantly increased from baseline at week 12 and week 24 in the fish oil group; median (range), baseline DSS 21.2 dyne/cm2 (4.0–40.1) versus 12-week DSS 24.2 dyne/cm2 (5.7–35.8); p = 0.001 and versus 24-week DSS 26.1 dyne/cm2 (6.7–37.2); p<0.001. There was no significant change in DSS at 12 or 24 weeks in the placebo group (fig 3).
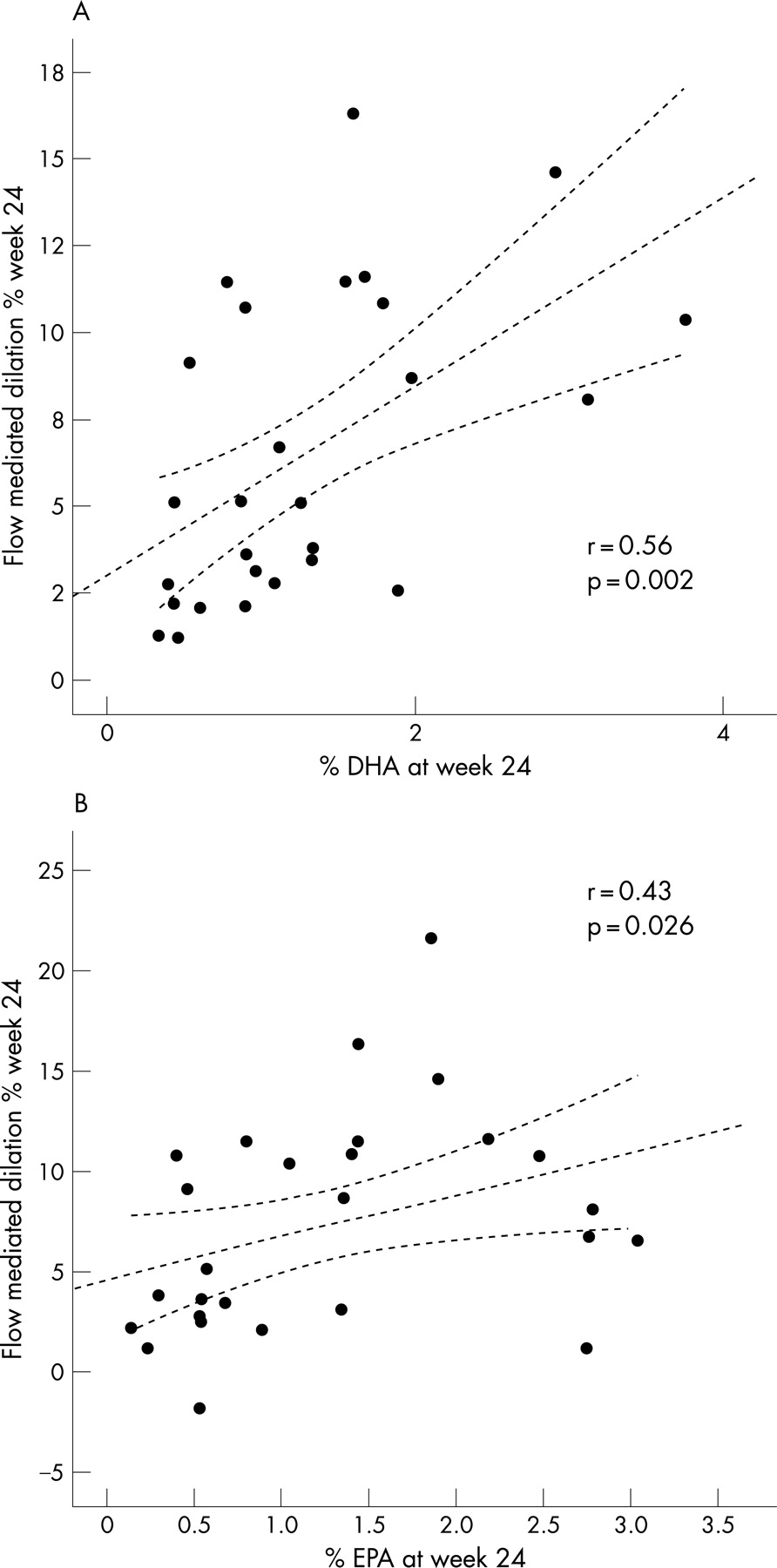
At 24 weeks, in the fish oil group, there was a significant positive correlation between percentage DHA and percentage EPA in the platelet cell membrane and FMD; percentage DHA and FMD, rs = 0.56; p = 0.002 (fig 4); percentage EPA and FMD, rs = 0.43; p = 0.026 (fig 4). There was no correlation between FMD and 8-isoprostanes or TG level.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
DISCUSSION
This is the first study in patients with SLE to show that supplementation with n-3 PUFAs improves endothelial function and confirms their beneficial effects on disease activity and oxidative stress.
Previous studies in SLE have shown a beneficial effect of n-3 PUFAs. However, many of these studies employed animal models18–21 or used high-dose n-3 PUFAs30–33 (up to 20 g/day), which would be difficult for patients to consume on a regular basis or to achieve through dietary means. This study confirms the finding of a previous study by our group that showed low-dose n-3 PUFAs have beneficial effects on disease activity in patients with SLE.22
The key link between n-3 PUFAs and inflammation is the production of eicosanoids. Eicosanoids, which include prostaglandins, thromboxanes, leucotrienes and other oxidised derivatives, are generated from AA. They are primarily involved in regulating the intensity and duration of the inflammatory response.34 Increased consumption of EPA and DHA results in increased proportions of these n-3 PUFAs in inflammatory cell phospholipids,35 as shown in this study. The incorporation of EPA and DHA into human inflammatory cells occurs in a dose–response fashion and is partly at the expense of AA. As there is less substrate available for synthesis of eicosanoids from AA, fish oil supplementation in the human diet has been shown to have profound effects on normal eicosanoid metabolism.
We studied the effects of n-3 PUFAs on the fatty acid composition of platelet cell membranes and platelet 8-isoprostanes. Platelets contain all the key sources for superoxide (O2−) and nitric oxide (NO) production found in endothelial cells and they contain the key regulatory enzymes, receptors and co-factors known to influence O2− and NO production. Most importantly platelets are capable of responding to both intracellular and extracellular stimulatory and inhibitory processes influencing this production thus enabling platelets to be employed as accessible ex vivo models for endothelial cells for the measurement of free radicals and oxidative stress.
Although their action in antagonising AA metabolism is a key anti-inflammatory effect of n-3 PUFAs, these fatty acids have several other anti-inflammatory effects that might result from altered eicosanoid production or might be independent of this. Studies have shown that in sufficient quantities, dietary fish oil results in decreased leucocyte chemotaxis,36 decreased production of reactive oxygen species37 38 and proinflammatory cytokines,36 39 and decreased adhesion molecule expression40.
The marker of oxidative stress, 8-isoprostane, was significantly reduced by the n-3 PUFAs, but was also reduced in the placebo group. Supplementation studies of fish oil have reported 30–50% decreases in the production of reactive oxygen species (superoxide or hydrogen peroxide) by stimulated human neutrophils,37 and human monocytes.38 These studies have used similar doses of fish oil to this study (3.1–8.4 g/day EPA plus DHA). Studies using lower doses of n-3 PUFAs (0.55–2.3 g/day) failed to demonstrate effects on reactive oxygen species by either neutrophils or monocytes,41 indicating a potential minimum dose of n-3 PUFAs may be required to influence reactive oxygen species.
Olive oil was the main constituent of the placebo, to provide a similar calorific intake to the n-3 PUFAs. Numerous studies have shown the beneficial effect of a Mediterranean diet rich in olive oil on cardiovascular risk factors.42 In the patients with SLE there was a reduction in blood pressure in the placebo group, a finding similar to the recent study by Bondia-Pons et al,43 who reported a lowering of systolic blood pressure with moderate consumption of olive oil in healthy European men. Furthermore, the reduction in platelet 8-isoprostanes in the placebo group confirms the previous finding of a lowering of urinary 8-isoprostanes with olive oil.44
Unsurprisingly there was a significant reduction in TGs with n-3 PUFAs, as Omacor is currently licensed in the UK for the treatment of hypertriglyceridaemia. The reduction in TGs could account for some of the findings in the fish oil group, but all of the patients with SLE had normal TG levels and there was no correlation between TGs and FMD, thus any effect of the lowered TGs can be assumed to be minimal. Fish oils most likely have pleiotropic effects in conjunction with a lowering of TGs, analogous to the observed pleiotropic effects of statins and their cholesterol lowering action.
With the advent of refined and validated indices of disease activity in SLE, assessing the response to a therapeutic intervention in these patients is more comparable between studies. In this study both the SLAM-R and BILAG significantly improved with n-3 PUFAs. Within these scores the greatest effect was apparent in constitutional symptoms, integument, musculoskeletal and neuromotor scores. Symptoms related to these areas are the most frequent and often the most recalcitrant to treatment in patients with SLE, and yet even in this group of patients with SLE with “mild” disease, a beneficial effect with n-3 PUFAs was still observed.
There was no difference in the laboratory measures of disease activity (erythrocyte sedimentation rate, complement components C3 and C4, and dsDNA antibody titre), a similar finding to previous studies in humans.22 45 The clinical value of laboratory indices in predicting a disease flare in SLE has been questioned, as individuals with identical serological pictures can present with a different severity of SLE.46
The calculated DSS in the brachial artery after reactive hyperaemia significantly increased in the fish oil group, with a consequent increase in NO-mediated brachial artery dilation and hence FMD. ω-3 PUFAs augment endothelium-dependent relaxation in porcine coronary arteries and also reduces contractile responses evoked by noradrenaline and AA in the rat aorta.47 In addition, exposure of cultured endothelial cells to EPA potentiates the release of NO in response to receptor agonists such as purines and kinins.48 Clinical studies have previously shown an improvement in endothelial function in disease states associated with atherosclerosis with n-3 PUFA supplementation.12–17 In these studies the degree of endothelial function correlated with the concentration of EPA and DHA incorporated into the cell membranes. A similar finding was observed in this study, with a positive correlation observed between percentage EPA and percentage DHA in the platelet cell membrane and the degree of FMD. The relationship was much stronger with DHA than EPA, and when applying the Bonferroni principle, the correlation between FMD and EPA would not be significant. A similar finding was reported by Mori et al49 who found that DHA significantly improved forearm blood flow in response to acetylcholine, but EPA had no effect. It has been suggested that EPA and DHA do not act synergistically to improve all aspects of vascular function but have different beneficial and also detrimental effects.49 It may be the relative amounts of EPA and DHA within the supplement that determines what vascular improvement is observed; however, this requires further study.
One potential mechanism by which n-3 PUFAs potentiate endothelial function is through an alteration in eNOS interaction with caveolin. In unstimulated endothelial cells, eNOS is targeted to specific microdomains in the plasma membrane termed caveolae, where eNOS is associated with a specific scaffold protein caveolin, resulting in inhibition of the enzyme activity.50 Stimulation of the binding of calmodulin to eNOS results in dissociation of the enzyme from caveolin, thereby activating eNOS.51 It has been demonstrated that n-3 PUFAs, through a calcium-independent mechanism can activate eNOS through the translocation and dissociation of the enzyme from caveolin in endothelial cells in situ.52
By exerting strict exclusion criteria these results will be less generalisable to clinical practice, but as this is the first study to evaluate the effect of fish oils on endothelial function in SLE detecting an intervention effect was the first priority and therefore confounding factors were kept to a minimum.
This is the first study to show a beneficial effect of low-dose dietary n-3 PUFAs on vascular function and disease activity in SLE. Further prospective, long-term, dose-ranging studies are required to ascertain the role of n-3 PUFAs on cardiovascular outcomes in patients with SLE.
Acknowledgments
This study was supported by a Wellcome Trust Clinical Research Fellowship and a Research Grant from Lupus UK.
REFERENCES
Footnotes
Funding: This study was funded by The Wellcome Trust and Lupus UK.
Competing interests: None.