
Abstract
Present guidelines discourage the use of CT coronary angiography (CTCA) in symptomatic angina patients. We examined the relation between coronary calcium score (CS) and the performance of CTCA in patients with stable and unstable angina in order to understand under which conditions CTCA might be a gate-keeper to conventional coronary angiography (CCA) in such patients. We included 360 patients between 50 and 70 years old with stable and unstable angina who were clinically referred for CCA irrespective of CS. Patients received CS and CCTA on 64-slice scanners in a multicenter cross-sectional trial. The institutional review board approved the study. Diagnostic performance of CTCA to detect or rule out significant coronary artery disease was calculated on a per patient level in pre-defined CS categories. The prevalence of significant coronary artery disease strongly increased with CS. Negative CTCA were associated with a negative likelihood ratio of <0.1 independent of CS. Positive CTCA was associated with a high positive likelihood ratio of 9.4 if CS was <10. However, for higher CS the positive likelihood ratio never exceeded 3.0 and for CS >400 it decreased to 1.3. In the 62 (17%) patients with CS <10, CTCA reliably identified the 42 (68%) of these patients without significant CAD, at no false negative CTCA scans. In symptomatic angina patients, a negative CTCA reliably excludes significant CAD but the additional value of CTCA decreases sharply with CS >10 and especially with CS >400. In patients with CS <10, CTCA provides excellent diagnostic performance.
Similar content being viewed by others

Background
Although CT coronary angiography (CTCA) can reliably rule out coronary artery stenosis in symptomatic angina patients, the specificity is limited in these patients [1–3]. Therefore, present guidelines discourage the use of CTCA in symptomatic angina patients, as the percentage of conventional coronary angiograms (CCA) that would be replaced by CTCA is considered too limited to justify the health risk and costs associated with CTCA [4, 5]. We speculate that the influence of coronary calcification on the diagnostic performance of CTCA may in part explain the limited specificity of CTCA in symptomatic angina patients. First, the prevalence of coronary artery disease (CAD) increases with coronary CS [6]. Second, blooming artifacts caused by coronary calcification resulting in over-estimation of lesion severity may result in false positive findings [7, 8]. Previous studies on the influence of CS on the diagnostic performance of CTCA have provided contradictory evidence. As mentioned, some previous studies have reported a high number of false positive findings in patients with a high CS [7, 8]. Also, a recent large study reported that the specificity of CTCA was 86% in subjects with a CS ≤400, while it was reduced to 53% in subjects with a CS >400 [1]. However, others have reported no significant or only a limited impact of coronary calcification on the diagnostic accuracy of CTCA [9, 10].
In order to understand under which conditions CTCA might be a gate-keeper to CCA in patients with stable angina and unstable angina, we examined the relation between CS and the performance of CCTA in these patients.
Materials and methods
This cross sectional study was designed to prospectively include symptomatic angina patients who presented with stable and unstable anginal syndromes who were referred for clinically indicated CCA irrespective of CS [3]. Patients were requested to undergo an additional CTCA for research purposes besides their CCA. The study protocol was approved by the institutional review board of the Erasmus University Medical Center.
As described previously, for this multi-center multi-vendor study conducted from October 2004 until June 2006 360 patients between 50 and 70 years of age with stable angina pectoris or non-ST segment elevation acute coronary syndrome underwent a non-enhanced CT scan to determine the CS followed by a CTCA scan in addition to CCA [3]. No patients, vessels or segments were excluded from the analysis, even if image quality was poor due to extensive calcification, coronary motion or breathing artifacts. No patients with previous history of percutaneous transluminal coronary angioplasty, coronary artery bypass surgery, impaired renal function (serum creatinine >120 μmol/l), persistent arrhythmias, inability to perform a breath hold of 15 s or known allergy to iodinated contrast material, were included. The study was conducted in three university hospitals.
Patients with a heart rate exceeding 65 beats per minute (bpm) received additional beta-blockers (up to 100 mg metoprolol p.o. or up to 20 mg metoprolol i.v.). All patients received thorough breath hold instructions.
All scans were performed with 64-slice CT scanners in Center A (Sensation 64, Siemens, Forchheim, Germany), Center B (Brilliance 64, Philips Medical Systems, Best, The Netherlands) and Center C (Toshiba Multi-Slice Aquilion 64 system, Toshiba Medical Systems, Tokyo, Japan). A non-enhanced scan to calculate the total CS was performed prior to CTCA. The scan parameters of the scanners are listed in Table 1. A bolus-tracking technique was used to synchronize the start of image acquisition with the arrival of contrast agent in the coronary arteries. The effective dose of the nonenhanced scan and the CTCA was estimated from the product of the dose-length product and a conversion coefficient (k = 0.017 mSv/[mGy × cm]) for the chest as the investigated anatomical region [11].
Multiple datasets were reconstructed separately with retrospective ECG-gating in order to obtain optimal image quality for all coronary segments. The Agatston CS was calculated using dedicated software (Heartbeat-CS, Extended Brilliance Workspace, Philips Medical System, Best, The Netherlands) [12].
CTCA scans were evaluated by two experienced readers, blinded for the CCA results, for lumen stenosis >50% based on a visual estimate, using the axial images and multiplanar reformatted images. In case of disagreement, a third reader was consulted. The kappa-value for inter- and intraobserver variability was 0.70 and 0.72, respectively.
All CCAs, which were used as the standard of reference, were evaluated by a core lab of experienced cardiologists, who were unaware of the results of the CTCA. Stenoses were evaluated in the CCA projection with the worst degree of stenosis, and classified as significant if the lumen diameter reduction exceeded 50% as measured by QCA.
Descriptive statistics were used to evaluate the diagnostic performance of CS and CTCA to detect patients with significant CAD, including sensitivity, specificity, positive and negative predictive values, and positive and negative likelihood ratios. The likelihood ratio incorporates both the sensitivity and specificity of a test and provides a direct estimate of how much a test result will change the odds of having a disease. These diagnostic parameters were expressed with a 95% confidence interval (CI) calculated with binomial expansion. The diagnostic performance of CTCA was calculated for all patients combined, and for pre-defined subgroups of patients with an Agatston CS <10, between 10 and 100, between 100 and 400 and >400 [13].
A Chi-square test was performed to test for statistical significance (p < 0.05). All analyses were repeated separately for patients with stable and unstable anginal syndromes.
Prevalence of significant CAD was based on the presence of at least one significant stenosis as determined by QCA, which was considered the standard of reference.
Results
Patient characteristics are listed in Table 2. Two-hundred and forty-five (68%) of 360 study participants were male, and 233 (65%) presented with stable chest pain syndromes. The mean age was 60 ± 6 years, the mean body mass index was 27.3 ± 3.8 kg/m2 and the median Agatston CS was 213 (inter-quartile range 42–553). The prevalence of having at least one significant coronary stenosis was 68%. No significant differences in patient demographics were seen in patients presenting with stable and unstable anginal syndromes, except for a higher incidence of smokers and a higher prevalence and extent of significant CAD in the unstable angina patients.
As shown in Table 3, for all patients combined the sensitivity of CTCA to detect significant CAD was 99% (95%CI 97–100%), the specificity was 64% (95%CI 55–73%), positive and negative predictive value were 86% (95%CI 81–89%) and 97% (95%CI 90–100%), respectively. Positive and negative likelihood ratios to detect or exclude significant CAD were 2.8 (95%CI 2.2–3.5) and 0.01 (95%CI 0.00–0.05) for CTCA. Six of 37 (16%) subjects with a CS of 0, and 15 of 62 (24%) subjects with a CS <10 had significant CAD on CCA. Detection of significant CAD by CTCA was successful in all these subjects.
The estimated average effective radiation exposure was 1.2 ± 0.5 to 1.8 ± 0.9 mSv for CS and 15.5 ± 2.2 to 18.4 ± 3.2 mSv for CTCA.
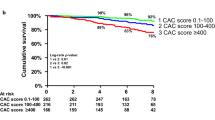
With increasing CS the prevalence of significant CAD increased steeply (Table 3). Whereas for patients with a CS <10 the prevalence of significant CAD was 24%, in those with a CS >400 it was 87%. Negative CTCA scans were associated with a negative likelihood ratio of 0.0–0.1 independent of CS (Table 3). A positive CTCA was associated with a high positive likelihood ratio of 9.4 (95%CI 4.1–22) if CS was <10. However, for higher CS the positive likelihood ratio never exceeded 3.0 and for CS >400 it decreased to 1.3 (95%CI 1.0–1.6). Also, the specificity of CTCA diminished significantly with increasing CS (Table 3). In patients with a CS <10 specificity was 89% (95%CI 76–96%). For higher CS specificity never exceeded 59% and for CS >400 decreased to 20% (95%CI 5–49%). Only 3 of 15 patients with a CS >400 and no significant CAD on CCA were evaluated as negative by CTCA. As shown in Table 4, the impact of CS on the diagnostic performance of CTCA is similar for patients with stable and unstable anginal syndromes. A CS <10 was present in 43 of 233 (18%) stable angina patients and in 19 of 127 (15%) unstable angina patients. In 43 stable angina patients and 19 unstable angina patients with CS <10, CTCA correctly identified 32 (74%) stable angina patients and 10 (53%) unstable angina patients in whom no significant CAD was present on CCA, at no false negative CTCA scans.
Discussion
In this study we set out to determine the relation between CS and the performance of CCTA in symptomatic stable and unstable angina patients in order to understand under which conditions CTCA might be a gate-keeper to CCA in such patients. We report that, in symptomatic angina patients, a negative CTCA reliably excludes significant CAD independent of CS but that the specificity and the positive likelihood ratio of CTCA decrease sharply with CS >10, and especially with CS >400. Thus, in symptomatic angina patients with a CS >10, and especially in those with a CS >400, CTCA has limited additional value in the diagnostic work-up. In the 17% of symptomatic angina patients with a CS <10, CTCA provides excellent negative and positive likelihood ratios for the detection or ruling out of significant CAD. CTCA correctly identifies the 74% of stable angina patients and 53% of unstable angina patients with a CS <10 without significant CAD in whom no CCA would be necessary, at no false negative scans.
The negative influence of CS on the diagnostic performance of CTCA was especially apparent in patients with a CS >400, in whom the specificity was only 20% (95%CI 5–49%) and the positive likelihood ratio was only 1.3 (95%CI 1.0–1.6). Ninety-nine of 114 (87%) patients with a CS >400 had significant CAD on CCA. Of the remaining 15 patients, i.e. those with a CS >400 and no significant CAD on CCA, only 3 were evaluated as negative by CTCA. Two factors may account for the latter findings. The 87% prevalence of significant CAD in patients with a CS >400 is probably the most important factor. In addition, calcium related blooming artifacts due to the limited spatial resolution of CTCA may have caused overestimation of lesion size, and thus false positive results [7, 8]. These findings are well in line with a previous study in which CTCA was of limited additional value in the diagnostic work-up of symptomatic patients with a high prevalence of significant CAD [14].
As mentioned above, previous studies on the impact of CS on the diagnostic impact of CTCA are contradictory. A previous large study reported that the specificity of CTCA was 86% in subjects with a CS ≤400, while it was 53% in subjects with a CS >400 [1]. Unfortunately, no data on the diagnostic performance of CTCA in subcategories of CS <400 were reported. Also, two other previous studies found that coronary calcification was one of the main factors leading to false positive results [7, 8]. However, Pundziute et al. reported no significant impact of a CS >400 on the diagnostic performance of CTCA in 110 patients clinically referred for CCA [10]. Also, Cademartiri et al. [9] divided 120 patients clinically referred for CCA in groups with a CS below and above the median Agatston CS of 55. He reported that the diagnostic performance of CTCA was affected only to a small extent by the CS. The prevalence of significant CAD and the CS of our population are similar to the previous studies mentioned, yet our study is a multicenter multivendor study and it has included substantially more subjects.
Interestingly, in a recent study in 664 asymptomatic individuals the prevalence of at least one significant stenosis on CTCA increased from 7.9% for patients with a CS between 1 and 100 to 14.5% for patients with a CS between 400 and 1,000 [15]. Unfortunately, no CCA data were available for this study. Thus, due to the absence of a standard of reference the diagnostic performance of CTCA for the detection of significant CAD could not be determined. The prevalence of significant CAD in the highest CS categories was significantly lower than in our study. This could be explained by the fact that the former study included asymptomatic subjects whereas we studied symptomatic angina patients.
Importantly however, CCA merely provides information on vessel lumen while CTCA also gives information on stenosis location and size, plaque burden, and plaque composition [16]. Future research is needed to determine the clinical value of this information, and specifically so in stable and unstable patients with a high CS in whom CTCA seems to have limited additional value if only the detection of significant CAD is taken into consideration.
When compared to most previous studies, the present study has included a larger number of subjects in a multicenter multivendor setting, allowing for a more reliable subgroup analysis. However, we acknowledge limitations of our study. Most importantly, in line with most previous studies, our subjects were derived from a selected population of symptomatic stable and unstable angina patients who were referred for CCA for clinical reasons. Thus our findings only apply to symptomatic stable and unstable angina patients. Future studies will need to address the value of CTCA in the diagnostic work-up of asymptomatic patients with a high CS. Secondly, in the present study 64-slice CTCA scanners were used. Future research will need to determine whether improvements in spatial and temporal resolution with new generation scanners using dual source techniques, dual energy techniques or more detector rows may improve the diagnostic performance of CTCA in patients with a high CS. Thirdly, we only studied patients between 50 and 70 years of age. The median CS for patients under 50 years of age is likely to be lower, and that of patients over 70 years of age is likely to be higher than the median CS of our population [17, 18]. As the association between CS and significant CAD varies with age [17, 18], our findings may not fully apply to subjects outside this age range. Fourthly, in line with previous studies, we excluded patients who were not in stable sinus rhythm, or did have renal insufficiency. In addition, a limited number of patients was not included for logistic reasons. Finally, the present study only focused on anatomical data. Additional research should focus on the value of the combination of CS, CTCA and functional tests such as Positron Emission Tomography and Single Photon Emission Computed Tomography in the diagnostic work-up of angina patients referred for CCA.
References
Budoff MJ, Dowe D, Jollis JG, Gitter M, Sutherland J, Halamert E, Scherer M, Bellinger R, Martin A, Benton R, Delago A, Min JK (2008) Diagnostic performance of 64-multidetector row coronary computed tomographic angiography for evaluation of coronary artery stenosis in individuals without known coronary artery disease: results from the prospective multicenter ACCURACY (Assessment by Coronary Computed Tomographic Angiography of Individuals Undergoing Invasive Coronary Angiography) trial. J Am Coll Cardiol 52:1724–1732
Garcia MJ, Lessick J, Hoffmann MH (2006) Accuracy of 16-row multidetector computed tomography for the assessment of coronary artery stenosis. JAMA 296:403–411
Meijboom WB, Meijs MF, Schuijf JD, Cramer MJ, Mollet NR, van Mieghem CA, Nieman K, van Werkhoven JM, Pundziute G, Weustink AC, de Vos AM, Pugliese F, Rensing B, Jukema JW, Bax JJ, Prokop M, Doevendans PA, Hunink MG, Krestin GP, De Feyter PJ (2008) Diagnostic accuracy of 64-slice computed tomography coronary angiography: a prospective, multicenter, multivendor study. J Am Coll Cardiol 52:2135–2144
Hunold P, Vogt FM, Schmermund A, Debatin JF, Kerkhoff G, Budde T, Erbel R, Ewen K, Barkhausen J (2003) Radiation exposure during cardiac CT: effective doses at multi-detector row CT and electron-beam CT. Radiology 226:145–152
Schroeder S, Achenbach S, Bengel F, Burgstahler C, Cademartiri F, De Feyter PJ, George R, Kaufmann P, Kopp AF, Knuuti J, Ropers D, Schuijf J, Tops LF, Bax JJ (2008) Cardiac computed tomography: indications, applications, limitations, and training requirements: report of a Writing Group deployed by the Working Group Nuclear Cardiology and Cardiac CT of the European Society of Cardiology and the European Council of Nuclear Cardiology. Eur Heart J 29:531–556
Budoff MJ, Diamond GA, Raggi P, Arad Y, Guerci AD, Callister TQ, Berman D (2002) Continuous probabilistic prediction of angiographically significant coronary artery disease using electron beam tomography. Circulation 105:1791–1796
Kuettner A, Burgstahler C, Beck T, Drosch T, Kopp AF, Heuschmid M, Claussen CD, Schroeder S (2005) Coronary vessel visualization using true 16-row multi-slice computed tomography technology. Int J Cardiovasc Imaging 21:331–337
Hoffmann U, Moselewski F, Cury RC, Ferencik M, Jang IK, Diaz LJ, Abbara S, Brady TJ, Achenbach S (2004) Predictive value of 16-slice multidetector spiral computed tomography to detect significant obstructive coronary artery disease in patients at high risk for coronary artery disease: patient-versus segment-based analysis. Circulation 110:2638–2643
Cademartiri F, Mollet NR, Lemos PA, Saia F, Runza G, Midiri M, Krestin GP, De Feyter PJ (2005) Impact of coronary calcium score on diagnostic accuracy for the detection of significant coronary stenosis with multislice computed tomography angiography. Am J Cardiol 95:1225–1227
Pundziute G, Schuijf JD, Jukema JW, Lamb HJ, de Roos A, van der Wall EE, Bax JJ (2007) Impact of coronary calcium score on diagnostic accuracy of multislice computed tomography coronary angiography for detection of coronary artery disease. J Nucl Cardiol 14:36–43
Menzel H, Schibila H, Teunen D. European guidelines on quality criteria for computed tomography. Luxembourg: European Commission Publication. No: Eur 16262 EN. 2000.
Agatston AS, Janowitz WR, Hildner FJ, Zusmer NR, Viamonte M Jr, Detrano R (1990) Quantification of coronary artery calcium using ultrafast computed tomography. J Am Coll Cardiol 15:827–832
Rumberger JA, Brundage BH, Rader DJ, Kondos G (1999) Electron beam computed tomographic coronary calcium scanning: a review and guidelines for use in asymptomatic persons. Mayo Clin Proc 74:243–252
Meijboom WB, van Mieghem CA, Mollet NR, Pugliese F, Weustink AC, van Pelt N, Cademartiri F, Nieman K, Boersma E, de Jaegere P, Krestin GP, De Feyter PJ (2007) 64-slice computed tomography coronary angiography in patients with high, intermediate, or low pretest probability of significant coronary artery disease. J Am Coll Cardiol 50:1469–1475
Ho JS, Fitzgerald SJ, Stolfus LL, Wade WA, Reinhardt DB, Barlow CE, Cannaday JJ (2008) Relation of a coronary artery calcium score higher than 400 to coronary stenoses detected using multidetector computed tomography and to traditional cardiovascular risk factors. Am J Cardiol 101:1444–1447
Leber AW, Becker A, Knez A, von Ziegler F, Sirol M, Nikolaou K, Ohnesorge B, Fayad ZA, Becker CR, Reiser M, Steinbeck G, Boekstegers P (2006) Accuracy of 64-slice computed tomography to classify and quantify plaque volumes in the proximal coronary system: a comparative study using intravascular ultrasound. J Am Coll Cardiol 47:672–677
Bellasi A, Lacey C, Taylor AJ, Raggi P, Wilson PW, Budoff MJ, Vaccarino V, Shaw LJ (2007) Comparison of prognostic usefulness of coronary artery calcium in men versus women (results from a meta- and pooled analysis estimating all-cause mortality and coronary heart disease death or myocardial infarction). Am J Cardiol 100:409–414
Hoff JA, Chomka EV, Krainik AJ, Daviglus M, Rich S, Kondos GT (2001) Age and gender distributions of coronary artery calcium detected by electron beam tomography in 35, 246 adults. Am J Cardiol 87:1335–1339
Acknowledgments
The authors have full access to all of the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. This study was funded by an investigational grant, number 945-04-263 from the Zon/MW, a Dutch governmental organization. The Zon/MW had no involvement in the design or conduct of this study; data management and analysis; or manuscript preparation and review or authorization for submission.
Open Access
This article is distributed under the terms of the Creative Commons Attribution Noncommercial License which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This is an open access article distributed under the terms of the Creative Commons Attribution Noncommercial License (https://creativecommons.org/licenses/by-nc/2.0), which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
About this article
Cite this article
Meijs, M.F.L., Meijboom, W.B., Prokop, M. et al. Is there a role for CT coronary angiography in patients with symptomatic angina? Effect of coronary calcium score on identification of stenosis. Int J Cardiovasc Imaging 25, 847–854 (2009). https://doi.org/10.1007/s10554-009-9485-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10554-009-9485-7