
Abstract
Purpose
To evaluate the risk factors of tricuspid regurgitation (TR) after left-sided valve replacement (LSVR) and plan the initial surgical treatment of TR.
Methods
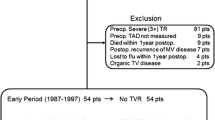
Two hundred and forty-eight patients, including 217 patients in the LSVR group and 31 patients in the LSVR+DeVega group, were followed up. A retrospective analysis was performed on 14 characteristics in the LSVR group. Variables were used to evaluate predictors of TR progression after single LSVR by either a univariate or multivariate analysis. DeVega’s tricuspid annuloplasty was evaluated on progress of TR by univariate analysis.
Results
The mean follow-up was 5.2 ± 2.9 (range, 3–16) years after surgery. In a univariate analysis, atrial fibrillation, huge left atrium, long time from onset to surgery, tricuspid rheumatic changes, preoperative +2 or +3 TR, the degradation of left ventricular ejection fraction, augmented right atrium, and single mitral valvular disease were significant risk factors for TR development. A multivariate analysis indicated that the four items mentioned above were statistically significant predictors of TR after surgery. The progress of TR in the LSVR+DeVega group was significantly less than in the LSVR group.
Conclusions
An aggressive repair of accompanying TR should be performed at the time of initial surgery in patients with a huge left atrium, atrial fibrillation, long time from onset to surgery, or tricuspid rheumatic changes. DeVega’s tricuspid annuloplasty therefore helps prevent a progression of TR.
Similar content being viewed by others

References
Sagie A, Schwammenthal E, Padial LR, Vazquez de Prada JA, Weyman AE, Levine RA. Determinants of functional tricuspid regurgitation in incomplete tricuspid valve closure: Doppler color flow study of 109 patients. J Am Coll Cardiol 1994;24:446–453.
Chopra HK, Nanda NC, Fan P, Kapur KK, Goyal R, Daruwalla D, et al. Can two-dimensional echocardiography and Doppler color flow mapping identify the need for tricuspid valve repair? J Am Coll Cardiol 1989;14:1266–1274.
Hinderliter AL, Willis PW, Long WA, Clarke WR, Ralph D, Caldwell EJ, et al. Frequency and severity of tricuspid regurgitation determined by Doppler echocardiography in primary pulmonary hypertension. Am J Cardiol 2003;91:1033–1037.
Fukuda S, Song JM, Gillinov AM, McCarthy PM, Daimon M, Kongsaerepong V, et al. Tricuspid valve tethering predicts residual tricuspid regurgitation after tricuspid annuloplasty. Circulation 2005;111:975–979.
Du ZD, Roguin N, Milgram E, Saab K, Koren A. Pulmonary hypertension in patients with thalassemia major. Am Heart J 1997;134:532–537.
Braunwald NS, Ross J, Morrow AG. Conservative management of tricuspid regurgitation in patients undergoing mitral valve replacement. Circulation 1967;35:I-63–I-69.
Duran CMG, Pomar JL, Colman T, Figueroa A, Revuelta JM, Ubago JL. Is tricuspid valve repair necessary? J Thorac Cardiovasc Surg 1980;80:849–860.
Porter A, Shapira Y, Wurzel M, Sulkes J, Vaturi M, Adler Y, et al. Tricuspid regurgitation late after mitral valve replacement: clinical and echocardiographic evaluation. J Heart Valve Dis 1999;8:57–62.
Matsuyama K, Matsumoto M, Sugita T, Nishizawa J, Tokuda Y, Matsuo T. Predictors of residual tricuspid regurgitation after mitral valve surgery. Ann Thorac Surg 2003;75:1826–1828.
Colombo T, Russo C, Ciliberto GR, Lanfranconi M, Bruschi G, Agati S, et al. Tricuspid regurgitation secondary to mitral valve disease: tricuspid annulus function as guide to tricuspid valve repair. Cardiovasc Surg 2001;9:369–377.
Tager R, Skudicky D, Mueller U, Essop R, Hammond G, Sareli P. Long-term follow-up of rheumatic patients undergoing left-sided valve replacement with tricuspid annuloplasty — validity of preoperative echocardiographic criteria in the decision to perform tricuspid annuloplasty. Am J Cardiol 1998;81:1013–1016.
Benjamin EJ, D’Agostino RB, Belanger AJ, Wolf PA, Levy D. Left atrial size and the risk of stroke and death. The Framingham Heart Study. Circulation 1995;92:835–841.
Vaziri SM, Larson MG, Benjamin EJ, Levy D. Echocardiographic predictors of nonrheumatic atrial fibrillation. The Framingham Heart Study. Circulation 1994;89:724–730.
Kizer JR, Bella JN, Palmieri V, Liu JE, Best LG, Lee ET, et al. Left atrial diameter as an independent predictor of first clinical cardiovascular events in middle-aged and elderly adults: the Strong Heart Study (SHS). Am Heart J 2006;151:412–418.
Henry WL, Morganroth J, Pearlman AS, Clark CE, Redwood DR, Itscoitz SB, et al. Relation between echocardiographically determined left atrial size and atrial fibrillation. Circulation 1976;53:273–279.
Sanfilippo AJ, Abascal VM, Sheehan M, Oertel LB, Harrigan P, Hughes RA, et al. Atrial enlargement as a consequence of atrial fibrillation: a prospective echocardiographic study. Circulation 1990;82:792–797.
Kim HK, Kim YJ, Kim KI, Jo SH, Kim KB, Ahn H, et al. Impact of the maze operation combined with left-sided valve surgery on the change in tricuspid regurgitation over time. Circulation 2005;112:I14–I19.
Vaturi M, Sagie A, Shapira Y, Feldman A, Fink N, Strasberg B, et al. Impact of atrial fibrillation on clinical status, atrial size and hemodynamics in patients after mitral valve replacement. J Heart Valve Dis 2001;10:763–766.
Cohn LH. Tricuspid regurgitation secondary to mitral valve disease: when and how to repair. J Card Surg 1994;9:237–241.
Shatapathy P, Aggarwal BK, Kamath SG. Tricuspid valve repair: a rational alternative. J Heart Valve Dis 2000;9:276–282.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Wang, G., Sun, Z., Xia, J. et al. Predictors of secondary tricuspid regurgitation after left-sided valve replacement. Surg Today 38, 778–783 (2008). https://doi.org/10.1007/s00595-007-3721-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00595-007-3721-3