Article Text

Abstract
Background The choice of antithrombotic therapy after percutaneous coronary intervention (PCI) is heavily dependent on the relative trade-off between major bleeding (MB) and myocardial infarction (MI). However, the mortality trade-off was mostly described in Western populations and remained unknown in East Asians.
Method This was a retrospective cohort study from 14 hospitals under the Hospital Authority of Hong Kong between 2004 and 2017. Participants were patients undergoing first-time PCI and survived for the first year. Patients were stratified by the presence of MB and MI during the first year. The primary endpoint was all-cause mortality between 1 and 5 years after PCI. The secondary endpoint was cardiovascular mortality.
Results A total of 32 180 patients were analysed. After adjustment for baseline characteristics and using patients with neither events as reference, the risks of all-cause mortality were increased in patients with MI only (HR, 1.63; 95% CI 1.45 to 1.84; p<0.001), further increased in those with MB only (HR, 2.11, 95% CI 1.86 to 2.39; p<0.001) and highest in those with both (HR, 2.92; 95% CI 2.39 to 3.56; p<0.001). In both Cox regression and propensity score analyses, MB had a stronger impact on all-cause mortality than MI, but similar impact on cardiovascular mortality.
Conclusions Both MB and MI within the first year after PCI were associated with increase in all-cause and cardiovascular mortality in Chinese patients, but the impact was stronger with MB.
- percutaneous coronary intervention
- myocardial infarction
- coronary artery disease
- acute coronary syndrome
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- percutaneous coronary intervention
- myocardial infarction
- coronary artery disease
- acute coronary syndrome
Key questions
What is already known about this subject?
Major bleeding is the major trade-off from Intensification or prolongation of antithrombotic therapy after percutaneous coronary intervention.
What does this study add?
Both major bleeding and myocardial infarction were associated with increase in all-cause and cardiovascular mortality in Chinese patients.
The association was stronger with major bleeding.
How might this impact on clinical practice?
Physicians should judiciously place a higher priority on bleeding preventive strategies for Chinese or East Asian patients after percutaneous coronary intervention.
Background
Intensification or prolongation of dual antiplatelet therapy (DAPT) can reduce recurrent ischaemic events in patients undergoing percutaneous coronary intervention (PCI), but with more bleeding events as a trade-off.1–5 Major bleeding (MB) has strong associations with short and long-term mortality.6–10 In studies performed in predominantly Western populations, MB was found to be equally deleterious as myocardial infarction (MI) after PCI.8 11 12 However, East Asians have with a higher vulnerability to bleeding and lower susceptibility to ischaemic events than white patients, known as the East Asian Paradox.13–16 This trade-off between MB and MI on mortality after PCI in East Asians remained unexplored, yet such information would have crucial implication on medical decision making. Currently, there were many uncertainties in the optimal strategy on antithrombotic therapy in this most populous ethnic group.17–19 With the availability of a territory-wide PCI registry in Hong Kong, we sorted to determine relative impact of MB vs MI after PCI on all-cause mortality in Chinese patients.
Methods
Study population and design
Data from all patients who underwent first-time PCI between 1 January 2004 and 31 December 2017 from all 14 government funded hospitals that performed PCI and recorded in a territory-wide PCI registry were reviewed. Patients baseline characteristics, exposures and outcomes were retrieved from the PCI Registry and Clinical Data and Analysis Reporting System. We included all adult patients (18 years of age or older) of Chinese ethnicity who underwent first-time PCI. Exclusion criteria were patients who died before hospital discharge, had MB or MI within 30 days after PCI.
Definitions of exposure and outcome variables
Patients were stratified into four groups in a two-by-two factorial design according to the occurrence of MB and MI between hospital discharge to 365 days after PCI. MB was defined as any fatal bleeding event, bleeding that occurred in the critical sites (intracranial, intra-articular or intramuscular with compartment syndrome, intraocular, pericardial, retroperitoneal), bleeding necessitating transfusion of ≥2 units of blood product, or bleeding that caused a drop in haemoglobin of ≥0.2 g/L, in accordance to the International Society on Thrombosis and Haemostasis (ISTH).20 MI was defined according to the Fourth Universal Definition of Myocardial Infarction.21 We only included MB and MI that occurred after hospital discharge for PCI, similar to previous study.9 11 This time window was justified by the need to focus only on late events occurring in patients already stabilised post-PCI, excluding early events that are largely influenced by index clinical presentation and in-hospital interventional procedures.
The primary endpoint was all-cause mortality, as a time-to-first-event analysis between 1 and 5 years after PCI. The secondary endpoints were cardiovascular mortality, defined as death due to cardiac, cerebrovascular and peripheral vascular causes, for the same observation period.
Statistical analysis
All analyses were performed with prespecified endpoints and statistical methods. Unadjusted analyses were made using χ2 tests for categorical variables, Student’s t-test or Wilcoxon rank-sum tests for continuous variables and time-to-first event analysis for estimation of incidence rate. Cox regression analysis was performed to evaluate the independent relationship between late MB and clinical outcomes, adjusting for potential confounders selected a priori based on published data and biological plausibility. Variables adjusted were gender, age, tobacco use, diabetes mellitus, hypertension, dyslipidaemia, cerebrovascular disease, peripheral vascular disease, chronic obstructive pulmonary disease, peripheral artery disease, prior myocardial infarction, prior coronary artery bypass surgery, congestive heart failure, atrial fibrillation or flutter, chronic kidney disease (estimated glomerular filtration rate <60 mL/min/m2, baseline anaemia (haemoglobin <13 g/dL for men, <12 g/dL for women), history of cancer, acute coronary syndrome (ACS), number of epicardial arteries affected and medications on discharge (aspirin, potent P2Y12 inhibitor (ie, ticagrelor or prasugrel), anticoagulation therapy).
Sensitivity analyses
To assess for any residual confounding by treatment selection, we performed falsification testing with new diagnosis of cancer and hip fracture after PCI. It was selected based on its association with mortality but were biologically unlikely to be causally related to MB or MI.22
To assess the relative hazard of MI versus MB, we constructed a propensity score that predicted the likelihood of MB without MI versus MI without MB, using the same variables used in the primary analysis. We generated two groups of patient by 1:1 propensity-score-matching using a calliper of 0.2 times the SD of the logit of the propensity score. Then we compare the primary outcome in the propensity score matched cohort without further adjustment.
In the primary and secondary analysis, the complete case method was adopted to address missing data. To test the robustness of our results, the regression analysis was repeated with the entire cohort using the technique of multiple imputations by chained equations to account for missing data.
Exploratory analyses
We explored effect modifications of the relationship between MB and MI on all-cause mortality in predefined subgroups, using the propensity matched cohort constructed in the sensitivity analysis. Predefined subgroups examined were sex, age >65, ACS, chronic kidney disease and baseline anaemia.
Data management and statistical analyses were performed in Stata software, V.16 (StataCorp LP). A two-tailed p value of less than 0.05 was considered statistically significant. For each endpoint, Bonferroni correction was adopted to control for multiple comparison (ie, p value is considered significant only if it is less than 0.05 divided by the number of pair-wise comparison within that outcome).
Results
Patients and characteristics
Between January 2004 and December 2017, a total of 36 344 patients were considered for inclusion: 4144 were excluded due to any of the following exclusion criteria—occurrence of any post-PCI MI or MB before hospital discharge, death within 1 year after PCI, or ethnicity not Chinese. The remaining 32 180 patients were included as the cohort for imputation analysis. A total of 2076 (6.5%) patients were excluded from the complete case analysis due to missing values in any of the variables used in the Cox regression model (figure 1).

Study profile. PCI, percutaneous coronary intervention.
Among the 30 104 patients who entered the primary analysis model as complete case, 27 109 (90.0%) had neither postdischarge MI or MB, 1640 (5.4%) had MI only, 1123 (3.7%) had MB only and 232 (0.8%) had both MI and MB within the first year. Patients with MB were more commonly female, older and having comorbidities including diabetes, hypertension, cerebrovascular disease, chronic kidney disease and anaemia. Patients with MI generally had more prior MI and presenting as ACS. Table 1 shows the baseline and characteristics of the study population.
Baseline characteristics of patients stratified according to presence of myocardial infarction and major bleeding
Primary outcome
During the observation period, the crude annualised mortality rates were 2.28%, 5.77%, 8.40% and 16.25% for patients with neither event, with MI only, with MB only and with both, respectively (table 2). In adjusted analysis, compared with those with neither event, the risks of all-cause mortality were elevated in patient with MI only (HR, 1.63; 95% CI 1.45 to 1.84; p<0.001), further elevated in those with MB only (HR, 2.11, 95% CI 1.86 to 2.39; p<0.001) and highest in those with both events (HR, 2.92; 95% CI 2.39 to 3.56; p<0.001). All differences were statistically significant after Bonferroni correction for multiple comparison between all pair-wise comparison (figure 2 and table 3).
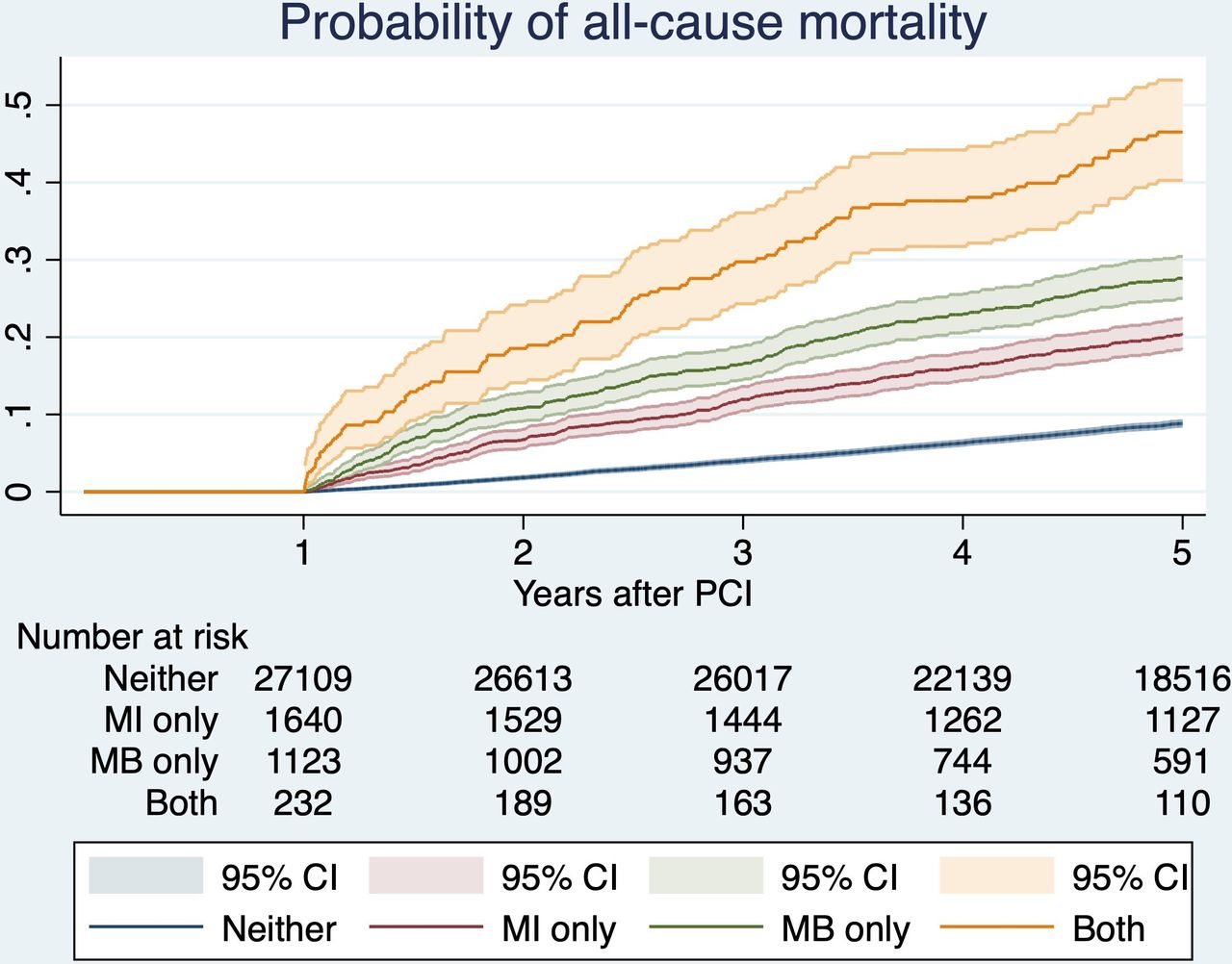
Estimated probability of the primary outcome of all-cause mortality. Patients without myocardial infarction (MB) or major bleeding (MB) within 1 year after index procedure had best survivals, and those with both had worst survivals. Patients with MB only had survivals better than those with MI only. PCI, percutaneous coronary intervention.
Unadjusted annualised risks (95% CI) of primary and secondary outcomes
Adjusted HRs of primary and secondary outcomes
Secondary outcomes
The annualised cardiovascular mortality rates were 0.66%, 2.33%, 2.25% and 6.90% for patients with neither event, with MI only, with MB only and with both, respectively (table 2). In adjusted analysis, the risks of cardiovascular mortality were lowest for patients with neither event and highest for those with both (HR, 3.72; 95% CI 2.72 to 5.08; p<0.001, compared with those with neither), while the risks were similar between those with MI only and MB only (figure 3 and table 3).

Estimated probability of the secondary outcome of cardiovascular mortality. Patients without myocardial infarction (MI) or major bleeding (MB) within 1 year after index procedure had lowest risk of cardiovascular mortality, and those with both had highest risk. Patients with MB only had cardiovascular mortality similar to those with MI only. PCI, percutaneous coronary intervention.
Sensitivity analyses
Falsification testing showed that MI and/or MB was not associated with new cancer diagnosis. The risks of new cancer diagnosis was similar for patients with MI only (HR, 1.10; 95% CI 0.86 to 1.40, p=0.451), with MB only (HR, 0.84; 95% CI 0.59 to 1.19; p=0.321) and with both (HR, 1.55; 95% CI 0.85 to 2.82, p=0.154). The pair-wise comparisons were shown in online supplemental table S1. These findings were suggestive of no significant residual confounding.
Supplemental material
Using propensity score matching, a total of 2236 (1118 pairs with each pair having one patient from the MI only group and one from the MB only group) patients were included. The baseline characteristics were well balanced between groups with standardised difference <0.1 in all baseline variables (online supplemental table S2). Compared with those with MI only, patients with MB only had a higher risk of all-cause mortality (HR, 1.23; 95% CI 1.04 to 1.46, p=0.015) but similar cardiovascular mortality (HR, 0.78; 95% CI 0.58 to 1.05; p=0.100). These findings were in agreement with the main analysis.
A total of five variables in the Cox regression model had missing data (figure 1). To address the issue with missing data, multiple imputation by chained equations was conducted. The imputed cohort included all 2076 (6.5%) patients who were excluded due to missing values in any of the variables used in the model. In the imputed dataset, the risks of all-cause mortality were significantly higher in patients with MI only (HR, 1.64; 95% CI 1.46 to 1.83; p<0.001), with MB only (HR, 2.13; 95% CI 1.90 to 2.40; p<0.001) and with both (HR, 2.89; 95% CI 2.38 to 3.51, p<0.001), consistent with the complete case cohort. The risks of cardiovascular mortality also yielded the same patterns as the complete case cohort (online supplemental table S3).
Exploratory analyses
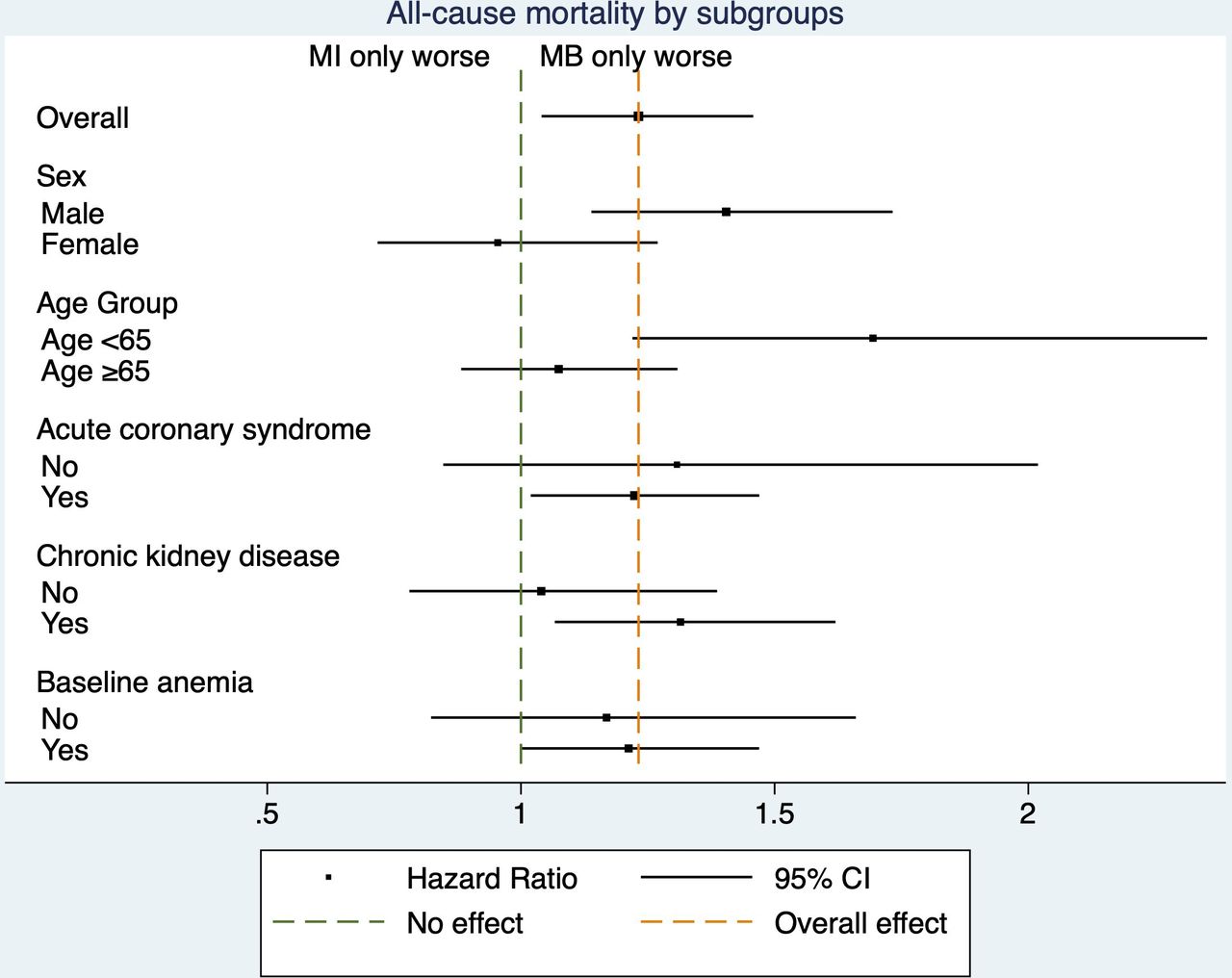
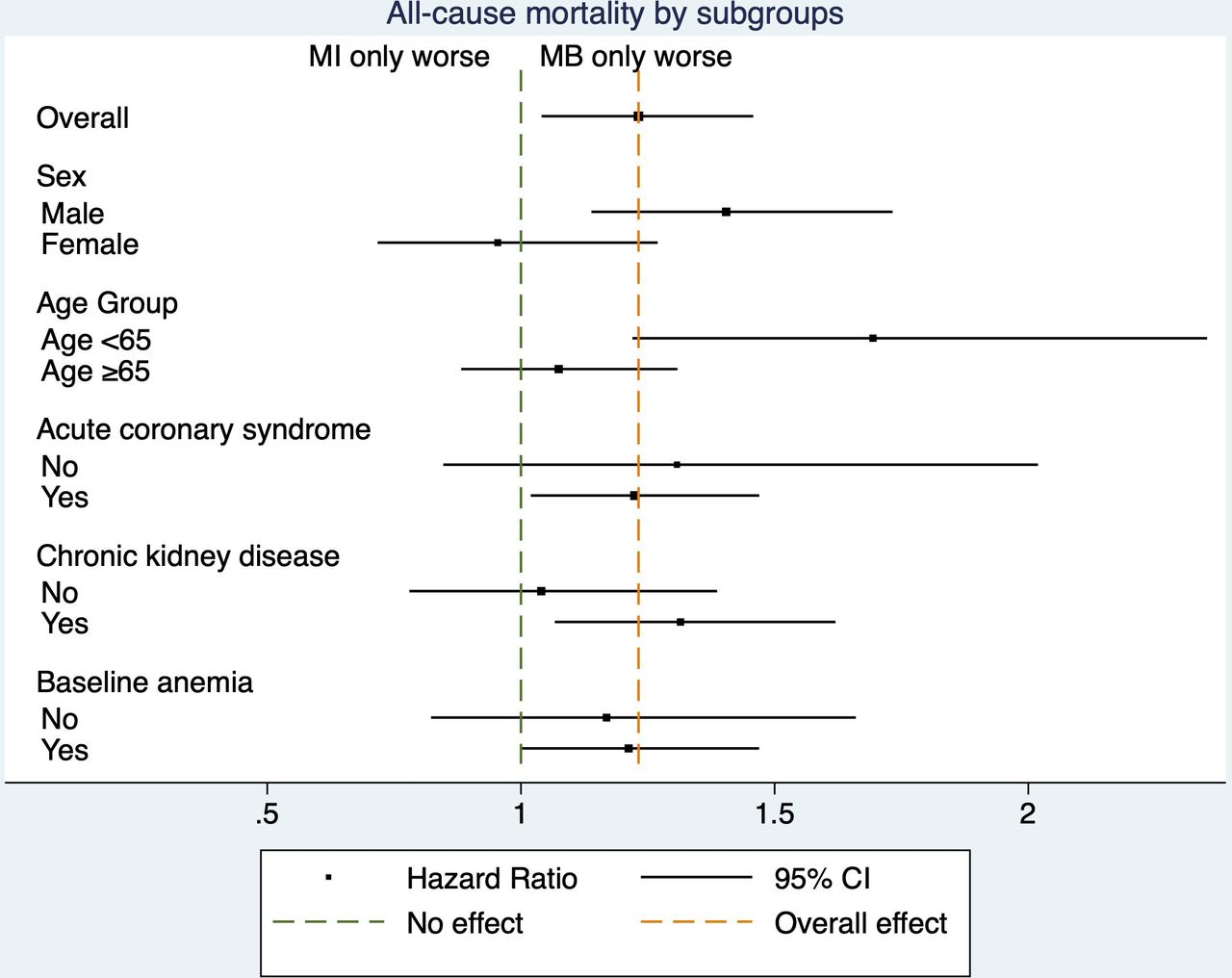
In the subgroup analysis, the effects of MB versus MI on all-cause mortality was modified by age and sex, but not by ACS, chronic kidney disease and baseline anaemia. Male sex and age <65 were subgroups that MB had a more pronounced impact on mortality compared with MI (figure 4 and table 4).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Forest plot for subgroup analysis. In the propensity matched cohort, patients with major bleeding (MB) only has higher all-cause mortality than those with myocardial infarction (MI) only. The effect was more pronounced in male and younger patients.
Subgroup analysis in the propensity matched cohort
Discussion
In this territory-wide PCI registry with exclusive Chinese patients, survivors with postdischarge MB and MI within 1 year after PCI were associated with significantly increased long-term all-cause mortality and cardiovascular mortality. Both MB and MI had incremental adverse impact on mortality, but the impact was stronger with MB.
Previous studies performed in predominantly Western populations observed that only severe MB, but not any overt MB, carries similar prognostic impact on mortality as with MI.11 12 Such observations suggest that it might be fair to pursue a more intense antiplatelet regimen to avoid an MI even at the expense of mild-to-moderate bleeding in patients with high ischaemic risk.11 They also challenge the inclusion of less severe bleeding that are more frequent but less prognostically significant into net clinical outcome in drug trials.11 However these postulations may not be applicable in East Asians. Since East Asians have different thrombotic and bleeding profiles from white patients,13–16 the ischaemia-bleeding trade-off maybe different in East Asians. Our study suggested that MB maybe prognostically more important than MI in East Asian patients, and therefore physicians may reasonably pursue a less intense antiplatelet regimen to avoid MB even at the expense of higher ischaemic risk. This differential trade-off may explain why ticagrelor was able to reduce major adverse cardiac events (MACE) and all-cause mortality compared with clopidogrel in many international randomised controlled trials (RCT),1 23 but similar findings cannot be replicated in East Asian populations.24 25 Notably, the TICA-KOREA study randomised 800 Koreans with ACS to ticagrelor or clopidogrel, and found an increase in major bleeding and fatal bleeding with ticagrelor, along with a numerically higher incidence of ischaemic events.25 Similarly, extended duration of DAPT beyond 12 months after PCI was shown to reduce MACE and mortality in international RCT, but benefits were limited to non-East Asian studies.4 26 Taken together, these patterns and our current findings strongly suggest that DAPT intensity and duration should be weighed considering the trade-off between the race-specific ischaemic versus bleeding risks of the patient. Current major international guidelines have called for more research specifically on East Asians given the paucity of data,18 19 27 and therefore our findings will be valuable to develop more precise and evidence-based guideline recommendations.
Potent P2Y12 inhibitors or addition of oral anti-coagulation therapy were shown to improve ischaemic outcomes in patients with ACS, but at a cost of excessive bleeding events.1–4 Most of these trials failed to show any mortality benefit, which in conjuncture with our findings suggested that bleeding is also detrimental to overall survival.
Our observation of a stronger mortality impact with MB than MI was different from previous studies.11 12 Apart from ethnicity, another possible explanation was the long duration of follow-up (up to 5 years). In a post-hoc analysis of 13 819 patients, mortality impact of MB was sustained over time up to 1 year after the event, whereas the mortality impact of MI rapidly dissipated and was no longer significant after 30 days.12 Therefore the excess mortality associated with MB may accrue over time more significantly than MI. Although it may be challenging to reconcile with other studies that showed an opposite temporal association of ischaemia and bleeding with mortality,28 29 these observations highlighted the importance of longer follow-up period in clinical trials assessing the trade-off between ischaemia and bleeding.
Our cohort only included survivors with (or without) MB and MI, because our objective was to evaluate the long-term impact of those events, while the short-term survival is heavily influenced by the severity and clinical management of those events. In this perspective, prevention of these events becomes the only viable strategy to improve outcomes. Since survival is considered the most valuable outcome in the patients’ perspective,30 our findings suggest that bleeding avoidance is at least equally or even more important than prevention of future ischaemic events in Chinese patients undergoing PCI. Evidence supported strategies to reduce bleeding events after PCI include shorter DAPT duration, de-escalation of potent P2Y12 inhibitors, and ulcer prophylaxis with proton pump inhibitors.31–36 Physicians should judiciously place a higher priority on employment of these strategies for Chinese or East Asian patients.
Net clinical benefit outcomes have been emerging as a popular endpoint to account for both anti-ischaemic and bleeding effect. However, this practice maybe inadequate and poses challenges to appropriately interpreting clinical trials.37 To overcome this limitation of the classic time-to-event analysis, alternative statistical approaches of ranking or weighing events according to their clinical significance can minimise imbalances from differences in direction and impact of an individual component of the endpoint.38–40 Our study could provide useful information on a more objective way to rank or weigh ischaemic and bleeding events in East Asian populations.
This study had some limitations. First, the observational nature of the study conferred risks of unmeasured confounding and bias, but we had adjusted extensively by Cox regression model for potential confounders, and the findings were consistent in multiple sensitivity analyses including propensity score models, falsification analysis and multiple imputation by chained equation. Nonetheless, the impact of MB and MI, by nature, cannot be studied in a randomised setting. Second, this study included only Chinese patients and may not be generalisable across other ethnic groups. Third, our study described the event–survival relationship in survivors only, and direct MB or MI related death during the first year of PCI was not examined. Fourth, our definition of bleeding was according to the ISTH, which slightly differ from the more commonly referenced type 3 or 5 Bleeding Academic Research Consortium (BARC). However, a type 3b BARC bleeding (requiring surgical intervention or vasoactive agents) is similarly represented in the ISTH definition of drop in haemoglobin >2 g/dL and/or blood transfusion, and therefore unlikely to change the association observed in our study.
Conclusion
In a large registry with exclusive Chinese patients, MB and MI within the first year after PCI were associated with significantly increase long-term mortality and cardiovascular mortality. Both MB and MI had incremental adverse impact on mortality, but the impact was stronger with MB.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by Institutional Review Board of the University of Hong Kong/Hospital Authority Hong Kong West Cluster UW 20-176This study is a retrospective study. Informed consent was waived. It does not contain personal and/or medical information about an identifiable individual.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @drandrewkyng
Contributors AK-YN and C-WS were responsible for the conception and design of the study. AK-YN analysed the data collected by AI, LTL and IWL. AK-YN interpreted the data. AK-YN and PYN drafted the manuscript. All authors revised and approved the final manuscript, and are accountable for the accuracy and integrity of the work. AK-YN is the guarantor who accepts full responsibility for the finished work and/or the conduct of the study, had access to the data, and controlled the decision to publish.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.