Article Text

Abstract
Objective To bring together patients, parents, charities and clinicians in a Priority Setting Partnership to establish national clinical priorities for research in children and adults with congenital heart disease.
Methods The established James Lind Alliance methodology was used to identify and prioritise research on the management of congenital heart disease, focusing on diagnosis, treatment and outcomes. An initial open survey was used to gather potential uncertainties which were filtered, categorised, converted into summary questions and checked against current evidence. In a second survey, respondents identified the unanswered questions most important to them. At two final workshops, patients, parents, charities and healthcare professionals agreed the top 10 lists of priorities for child/antenatal and adult congenital heart disease research.
Results 524 respondents submitted 1373 individual questions, from which 313 out of scope or duplicate questions were removed. The remaining 1060 questions were distilled into summary questions and checked against existing literature, with only three questions deemed entirely answered and removed. 250 respondents completed the child/antenatal survey (56 uncertainties) and 252 completed the adult survey (47 uncertainties). The questions ranked the highest by clinicians and non-clinicians were taken forward to consensus workshops, where two sets of top 10 research priorities were agreed.
Conclusions Through an established and equitable process, we determined national clinical priorities for congenital heart disease research. These will be taken forward by specific working groups, a national patient and public involvement group, and through the establishment of a UK and Ireland network for collaborative, multicentre clinical trials in congenital heart disease.
- heart defects, congenital
- research design
- delivery of health care
Data availability statement
Data are available in a public, open access repository. Key documents and datasets are accessible on the JLA website: https://www.jla.nihr.ac.uk/priority-setting-partnerships/congenital-heart-disease/.
This is an open access article distributed in accordance with the Creative Commons Attribution 4.0 Unported (CC BY 4.0) license, which permits others to copy, redistribute, remix, transform and build upon this work for any purpose, provided the original work is properly cited, a link to the licence is given, and indication of whether changes were made. See: https://creativecommons.org/licenses/by/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
There is a lack of evidence to inform clinical decision-making in children and adults with congenital heart disease. Priority Setting Partnerships provide an equitable mechanism for identifying and prioritising research that is important to patients, their families and clinicians, through shared decision-making.
WHAT THIS STUDY ADDS
Through an established, multistakeholder, consensus development process, this partnership determined national priorities for research in children and adults with congenital heart disease, providing a platform for conducting the research that matters most to those who may directly benefit.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
This work will provide a catalyst for collaborative congenital heart disease research in the United Kingdom. A national strategy has been developed to address the priorities, including the establishment of a UK and Ireland network for conducting multicentre studies, especially clinical trials, a national patient and public involvement group, and specific working groups focusing on one or more related priorities.
Introduction
Congenital heart disease (CHD) is the most common type of birth defect, affecting 13 children born every day in the UK,1 but only around half are detected on routine antenatal screening.2 Many children require open heart surgery or other intervention, often within the first year of life and survival continues to improve2 3; yet early morbidities remain common after surgery4 and infants have an ongoing risk of death following discharge.5 Nowadays around 97% of children born with CHD are expected to survive into adulthood6 and there are estimated to be over 250 000 adults living with CHD in the UK,7 including an emerging population with conditions that previously were rarely compatible with survival, presenting new diagnostic and therapeutic challenges. Almost all patients require lifelong follow-up in specialist clinics to manage their unresolved burden of disease8; many develop late complications related to their condition or previous procedures, and have an ongoing need for increasingly hazardous reinterventions, to treat recurrent or progressive lesions, or replace prosthetic implants such as valves, conduits or pacemakers. Uncertainty over further interventions and long-term outlook may contribute to increased levels of anxiety, depression and other mental health issues in CHD.9 While a growing number are living with CHD into their 60s and beyond, developing acquired morbidities and senescence,10 long-term survival remains reduced compared with the general population, especially in those with uncorrected, palliated, complex or cyanotic heart conditions, with heart failure the most common cause of premature death.11
There is a lack of evidence to inform clinical decision-making in children and adults with CHD. The Cochrane Library contains fewer than 20 reviews on CHD topics,12 and there is a need for high-quality, multicentre clinical trials that answer important questions to improve their daily lives and outcomes.13 The British Heart Foundation (BHF) identified that ‘we urgently need research breakthroughs to ensure survivors (of CHD) lead longer and healthier lives’.14
The James Lind Alliance (JLA) is a non-profit-making initiative, established in 2004 and coordinated by the National Institute for Health and Care Research (NIHR), to bring together patients, carers and clinicians as equals in a Priority Setting Partnership (PSP).15 Through a defined method with shared decision making,16 PSPs identify and prioritise unanswered questions for research, or evidence uncertainties, providing a platform for researchers and funders to prioritise the research that matters most to research beneficiaries. We, therefore, brought together patients with lived experience of CHD, parents, national charities and healthcare professionals in the UK to form the national Congenital Heart Disease PSP.
Methods
This process was conducted with reference to the JLA Guidebook (V.10, March 2021)16 and reported in accordance with the REPRISE guideline (see online supplemental materials).17 ,18 A steering group of stakeholders with a wide range of lived experiences or professional interests in CHD, including patients, parents, charities and healthcare professionals was formed (see the Acknowledgements section) and agreed a protocol (see online supplemental materials). The scope of the PSP was collectively defined as: ‘The management of CHD throughout life, including prior to birth, focusing on:
Supplemental material
Diagnosis, during pregnancy or after birth.
Treatment (medical therapy, catheter intervention, surgery including mechanical support and transplantation, lifestyle or psychosocial intervention).
Outcomes of the conditions and/or treatments and the impact on patients and their families, including the physical, psychological and social effects of living with CHD.’
The PSP excluded from its scope questions about non-management-related aspects of CHD, such as aetiology or non-clinical genetics, acquired heart disease, other than occurring in the context of CHD, and other comorbidities, such as non-cardiac aspects of associated syndromes.
We worked with national charities and professional bodies throughout the process, including survey dissemination and workshop recruitment (see the acknowledgements section). The project was funded by a philanthropic donation, and the funder had no influence on determining the final list of priorities. The steering group anticipated that parents may be the most engaged group, as found in a previous national prioritisation exercise19 and noted that there are more healthcare specialists working with children with CHD than with adults. To protect potential priorities for the growing population of adults living with CHD, we, therefore, split the process into parallel child/antenatal and adult tracks at the prioritisation stage. The process comprised four stages, namely: (1) initial survey to gather uncertainties; (2) data processing and evidence checking; (3) interim prioritisation surveys and (4) final priority setting workshops. The steering group met regularly via Zoom video conferencing to oversee the process.
Initial survey
A cross-sectional, self-administered, public survey was conducted using REDCap. Respondents were asked: ‘What questions would you like to see answered by future research, relating to the diagnosis, treatment or outcomes of congenital heart disease?’ and invited to pose up to three questions. To understand the profile of respondents and any gaps, demographic data were collected on age, gender, ethnicity and role: patient, parent, other relative, healthcare professional, charity,or other. Respondents were asked to provide their name and email address to allow recontact. A link to the online survey was disseminated by our partner organisations via email, newsletters and social media, and promoted via a Facebook page (congenitalPSP) and twitter handle (@congenitalPSP) using the hashtag #CHDpriorities. The project website (www.birmingham.ac.uk/congenital-psp) contained detailed information about the partnership, process, partners and steering group.
The steering group recognised that South Asian and Black communities in the UK are disproportionately affected by CHD,20 with double the incidence of severe and complex defects associated with a high infant mortality, compared with the White population.21 The proportion unable to ‘speak English well’ is higher among those of South Asian ancestry (Asian-Indian 7.4%, Asian-Pakistani 11.2%, Asian-Bangladeshi 16.2%) than those of Black ancestry (Black-Caribbean 0.3%, Black-African 3.8%).22 To facilitate engagement with this population, the survey was translated into Urdu, Bengali, Gujarati and Hindi, with input from the Centre for Ethnic Health Research, along with English, Welsh and Polish, the most commonly spoken immigrant language in the UK,22 and made available to download, print and return via a Freepost address. Posters in five languages with a quick response (QR) code link to the online survey were distributed via community networks and mosques, and the printed survey was handed out to targeted demographics during clinic appointments. The PSP Lead also appeared on Living the Life on the Islam Channel, a prime-time contemporary lifestyle television show, to promote the survey among Muslim communities.
Data processing and evidence checking
Anonymised responses were collated and tagged as relevant to children, adults or both. Submissions identified as out of scope by the steering group were removed. The remaining questions were aggregated into project-specific categories devised by the Information Specialist, in consultation with the PSP Lead. Indicative summary questions were formed from these categories by steering group members, working in clinician/non-clinician pairs (following practice sessions facilitated online during two steering group meetings); using an iterative process, similar or overlapping questions were combined to form summary questions and reworded into plain, consistent language. The steering group reviewed and approved the final list of questions.
A literature search was conducted to identify guidelines and systematic reviews published within the last 5 years (see online supplemental materials), to check whether summary questions had been fully or partially answered. They were considered to be unanswered if a there was no definitive study or systematic review evidence, or recent guidelines concluded that there was insufficient evidence. The resulting longlist of confirmed uncertainties were taken forward to one or both interim prioritisation surveys.
Interim prioritisation surveys
Two second surveys, one child/antenatal and one adult, were conducted in English using Survey Monkey, which allowed uncertainties to be presented in a random order, to avoid preferencing of questions at the top. A link to the online survey was disseminated through partner organisations and directly to those who had provided an email address in the initial survey. Respondents were asked to select all questions that were important to them, and from these, to choose up to 10 of the most important. Demographic data were collected, and respondents were asked to provide their name, email address and reasons if interested in taking part in a workshop. Completed responses were collated and ranked according to frequency of prioritisation by clinicians and non-clinicians, and the highest ranked questions by each group were taken forward.
Final priority setting workshops
Two workshops were conducted, one child/antenatal and one adult, involving patients, parents, charities and healthcare professionals. Recruitment used a targeted phased approach through survey respondents and partner organisations to seek non-clinician participation with a range of conditions/backgrounds and clinical representation with a breadth of CHD expertise from centres across the UK and Ireland, aiming for equal numbers of each. Participants were provided with the shortlist of uncertainties and a glossary (see online supplemental materials) in advance. Three experienced JLA advisors facilitated the discussions to build consensus towards the final top 10 priorities using an adapted nominal group technique.16 Participants were divided into three small groups, each containing a mix of roles, experience and location, and ensuring that patients/parents were not grouped with their direct healthcare providers. Groups worked together through three discussion and ranking exercises, interspersed with feedback from the other groups, with a whole group session to agree a final ranking, including the top 10 list for each workshop. All participants were reimbursed for travel expenses and patient/parents were paid an honorarium.
Results
The initial online steering group meeting was held on 16 March 2021, with 12 further online meetings held approximately every 6 weeks throughout the process.
Initial survey
The initial survey was open from 29 June 2021 to 15 October 2021. A total of 524 individuals completed the survey, of whom 387 (73.9%) were patients or family members (tables 1–2). Most responses were submitted online, with one paper response in English via the Freepost address but none using the translated surveys.
Roles of survey respondents and workshop participants
Demographics of patient, parent and other family survey respondents and workshop participants
Data analysis
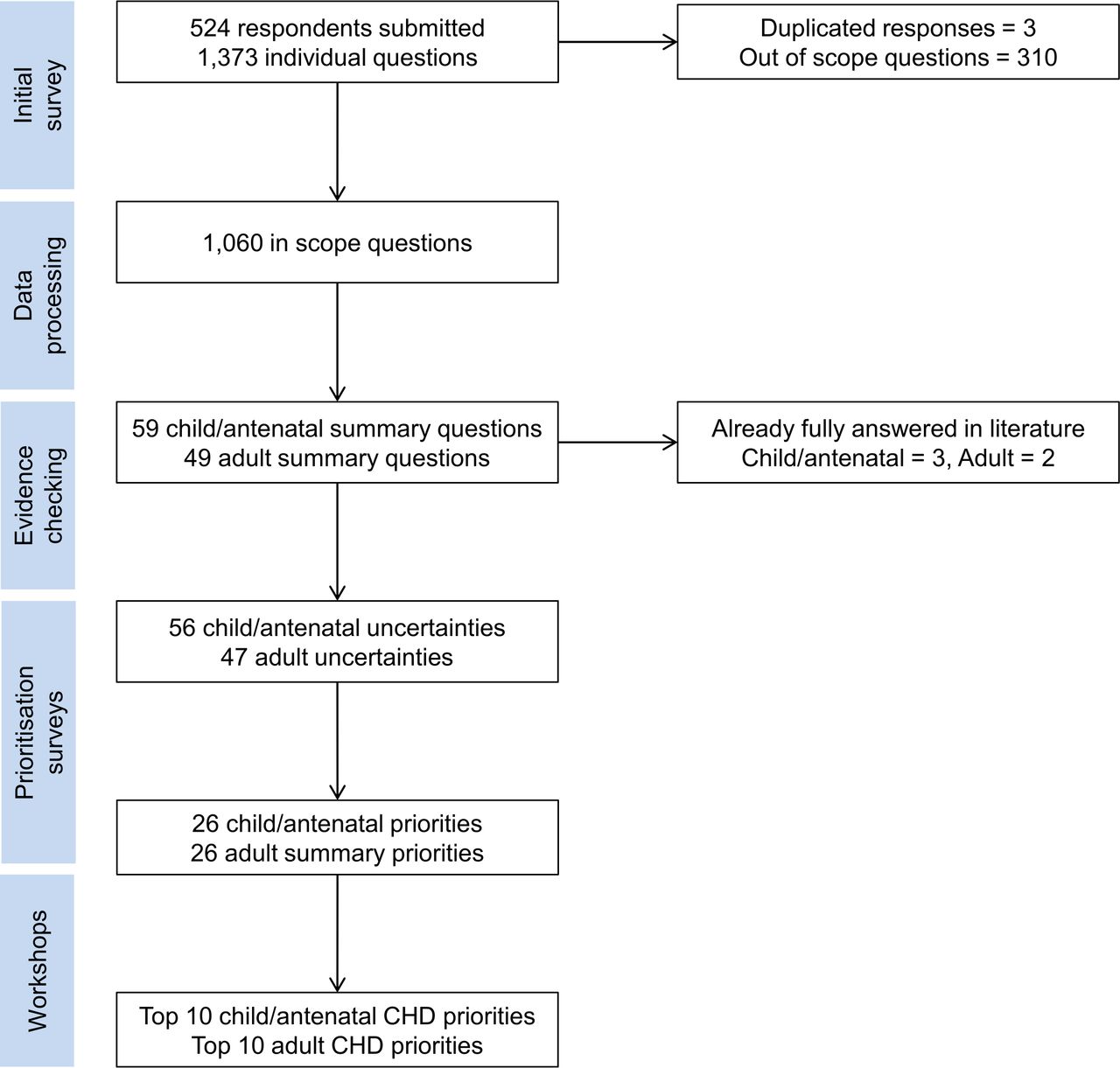
Respondents submitted 1373 questions, of which 3 were duplicated and 310 were deemed to be out of scope, mostly relating to causes of CHD (figure 1); examples of submitted questions are available on JLA website (https://www.jla.nihr.ac.uk/priority-setting-partnerships/congenital-heart-disease/). The remaining 1060 questions were reviewed by the steering group to generate 59 child/antenatal and 49 adult summary questions. These were individually checked against the existing literature; three child/antenatal and two adult questions were deemed fully answered and removed (see online supplemental materials), leaving 56 child/antenatal and 47 adult uncertainties to progress to the next stage.
{kind=link}
Flow diagram through the Priority Setting Partnership process: from submitted questions, to summary questions, to uncertainties, to priorities. CHD, congenital heart disease.
Interim prioritisation surveys
The second surveys were open from 21 March 2022 to 20 May 2022. A total of 446 (85.1%) respondents had provided a valid email address in the initial survey and were contacted directly. A total of 250 respondents completed the child/antenatal survey and 252 completed the adult survey, of whom 146 (58.4%) and 182 (72.2%), respectively, had lived experience of CHD (tables 1 and 2). The full list of questions and interim rankings is provided in online supplemental materials. The top 15 questions ranked by clinicians and/or non-clinicians were taken forward to each workshop, along with two additional questions highly ranked by both groups in the adult survey, providing 26 uncertainties for each workshop. The top ranked questions for young people, fathers and ethnic minority respondents were all included.
Final priority setting workshops
Workshops were held in person in central Birmingham, UK on 23 June 2022 and 24 June 2022. These were attended by 39 participants: 21 healthcare professionals and 18 non-clinicians, including 9 young people/adults living with CHD, 8 parents of children with CHD and 1 non-patient/parent national charity representative (tables 1 and 2). An additional 11 delegates had agreed to attend but withdrew at short notice due to new COVID-19 infection, family illness or travel disruption caused by national rail strikes. Healthcare professionals with a breadth of interests and expertise from all eleven tertiary CHD programmes in the UK and Ireland were invited, of which nine were represented at one or both workshops (see the Acknowledgements sectoion). There was excellent engagement from all participant groups, with moving personal stories and passionate informed debate; consensus was reached relatively quickly on both days, as shown by the interim small group rankings in online supplemental materials. The final top 10 national research priorities agreed at the workshops are shown in tables 3 and 4.
Top 10 national priorities for research in child/antenatal congenital heart disease (CHD)
Top 10 national priorities for research in adult congenital heart disease (CHD)
Discussion
Prioritisation of research through consultation with those affected by or caring for those with a disease ensures that it remains directly relevant to improving their lives.15 In this endeavour, we established national clinical priorities for research in children and adults with CHD by engaging with patients, parents, national charities and healthcare professionals. Our findings are important because they enable all stakeholders to focus on the questions which matter most to the end users of research and will be publicised widely to inform the direction of CHD research.
CHD is a lifelong condition, and the research priorities identified in this study reflect that journey: from antenatal screening, through reducing the frequency and impact of interventions, to treatments for advanced heart failure and life expectancy. Many encompass holistic outcomes, looking beyond early mortality to improve the quality of survivorship and reduce the impact of living with CHD. They cover a wide range of research areas including surgery, catheter interventions, intensive care, antenatal screening, psychology, cardio-obstetrics, electrophysiology, epidemiology, bioinformatics, pharmacology, technology, bioengineering and transplantation. While diverse methodologies will be required to address these priorities, including qualitative studies, database analysis and translational research, many are well suited to clinical trials. Six priorities on each list are derived from the same summary questions, triangulating and emphasising their importance to both groups, and translating into 14 distinct priorities: 4 child/antenatal-specific, 4 adult-specific and 6 throughout life.
A recent PSP was conducted in adult cardiac surgery for acquired disease23 but our PSP is the first time that the JLA process has been applied to CHD, thereby giving patients and their families an equal voice to clinicians.16 Several previous studies have identified research priorities in CHD, mostly in adults but with limited patient and public involvement (PPI). Cotts et al compiled a list of 45 questions and conducted an international survey of adult CHD providers to identify 10 priority questions, with limited input from patient groups24; unsurprisingly, the priorities were more specific and medically focused research questions. Helm et al conducted an online survey of adult patients with four specific conditions, their relatives and physicians in Germany to prioritise predetermined research topics.25 While the topics were less well defined, many were similar to the priorities we identified, including arrythmias and sudden death, pregnancy, mental health, Fontan failure, reoperations and heart failure. In the USA, Gurvitz et al reported the findings of a multidisciplinary working group composed of researchers in adult CHD and related fields, and one PPI representative, ‘recognising the importance of the patient perspective in research efforts’.26 Some of the priority topics identified were similar to our PSP, such as mechanical circulatory support/transplantation, sudden cardiac death, late outcomes of single ventricle heart conditions, mental health and pregnancy. Finally, Drury et al19 conducted a UK national study to identify research priorities in single ventricle heart conditions, involving patients, parents, healthcare professionals, researchers and charities. Priorities included prolonging the longevity of the Fontan circulation, brain development, heart failure, pregnancy, transplantation and use of new technology.
By defining national clinical priorities for research, we intend that this PSP will be transformative for collaborative CHD research in the UK.27 A national strategy has been developed to address these priorities, with endorsement from our national charity and professional partners, and includes establishing:
A UK and Ireland network for conducting multicentre studies, similar to the Paediatric Heart Network,28 focusing on clinical trials that address the priorities and have the potential to change clinical practice. It will use existing infrastructure such as the BHF Clinical Research Collaborative, NIHR Clinical Research Networks and established Clinical Trials Units with expertise in multi-centre paediatric, interventional and surgical trials.
A national CHD PPI group, composed of engaged patient, parent and charity members, who will actively contribute to the development, conduct and reporting of research.
Working groups focusing on one or more related priorities, comprising clinicians, researchers and PPI members, and overseen by the network. Their role will be to translate the priorities into specific research questions, lead project development and coordinate funding applications. NIHR recognises the importance of the JLA process and have established rolling calls across their funding programmes dedicated to studies that address priorities identified by PSPs.29
The strengths of this project include the use of a recognised, equitable and robust process for determining national research priorities, good engagement with stakeholder groups throughout the process, and broad representation of backgrounds, interests and centres at the workshops. A clear consensus between groups emerged rapidly during both workshops and the top 10 have appeal across the clinical spectrum. While there was overlap between the two lists, the top three child/antenatal priorities are paediatric-specific, while the adult-specific priorities are lower down and may have been squeezed out if conducted as a single process. Splitting at the interim prioritisation stage therefore fulfilled its role of protecting adult-specific priorities but may have inadvertently marginalised questions related to transition. While rail strikes disrupted attendance on both days, PPI attendance payments and reimbursement for expenses, in line with national standards, widened access and participation in the workshops.
There were several limitations. We explicitly focused on clinical priorities to maximise the potential for translation into clinical trials with potential patient benefit in the short term to medium term; however, by excluding non-management related uncertainties, such as causes of CHD, we dismissed the major translational impact which these more fundamental questions may have for future generations. We sought responses only from those living in the UK and working in the National Health Service, potentially limiting its international applicability. Despite extensive efforts to engage with ethnic minority communities, there were few responses by those of South Asian or Black ancestry, and only three non-White British/Irish patients or parents attended the workshops; this has been observed in other PSPs30 and will be explored in a separate paper. Similarly, fathers were relatively under-represented in both the surveys and workshops.
In conclusion, we brought together patients, their families, charities and healthcare professionals in a PSP to determine UK national priorities for research in CHD using an established shared decision-making process. This partnership provides a unique opportunity for the UK CHD community to develop collaborative research, through a national strategy to address the priorities including a network for multicentre clinical trials, a national PPI group and working groups to translate the most important questions into studies that can have an impact on patient care and improve outcomes.
Supplemental material
Supplemental material
Data availability statement
Data are available in a public, open access repository. Key documents and datasets are accessible on the JLA website: https://www.jla.nihr.ac.uk/priority-setting-partnerships/congenital-heart-disease/.
Ethics statements
Patient consent for publication
Ethics approval
As public involvement rather than participation in research, ethical approval was not required.
Acknowledgments
In memory of Michael J Cumper, a long-time advocate for improving the lives of those affected by CHD, whose knowledge, empathy, and common sense approach were of great benefit to shaping this process, and sadly passed away in July 2022.
Steering group: Patients/parents/charities: Michael Cumper (Somerville Heart Foundation), Alex Miskin, Sarah Murray, Fraser Pender, Sasha Rooprai, Jara Weinkauf, Julie Wootton (Children’s Heart Federation). Clinicians: Mr Nigel Drury (Lead, Cardiac Surgery, SCTS), Prof Katherine Brown (Intensive Care), Dr Louise Coats (Adult Congenital Cardiology), Mr Rafael Guerrero (Cardiac Surgery, SCTS), Prof John Simpson (Fetal/Paediatric Cardiology, BCCA), Prof John Thomson (Interventional Cardiology). James Lind Alliance: Katherine Cowan (Chair). Other: Dr Clare Herd (Information Specialist), Dr Giovanni Biglino (Bioinformatics), Sharmaine Afferion (Administrator).
Child/antenatal CHD workshop: Patients: Hayley Foster, Becky Little, Ellena Wood. Parents: Jon Arnold (Tiny Tickers), Claire Donnelly (Young at Heart), Mariam Gulfam, Sarah Kwasny, Sasha Rooprai. Charity: Lexie Katsaitis (Little Hearts Matter). Clinicians: Prof Frank Casey (Paediatric Cardiology, Belfast/Ireland), Prof Massimo Caputo (Cardiac Surgery, Bristol), Prof Mark Danton (Cardiac Surgery, Glasgow), Dr Rami Dhillon (Interventional Cardiology, Birmingham), Dr Kerry Gaskin (Nursing, Worcester), Dr Caroline Jones (Fetal/Paediatric Cardiology, Liverpool), Mr Tim Jones (Cardiac Surgery, Birmingham), Dr Julie Menzies (Paediatric Intensive Care Nursing, Birmingham), Andrew Nichols (Clinical Perfusion, Leeds), Kaye Walsh (Nursing, Newcastle). James Lind Alliance: Katherine Cowan, Suzannah Kinsella, Maryrose Tarpey.
Adult CHD workshop: Patients: Anise Collins, Elizabeth Connolly, Joanne Lloyd, Patrick Ridgway, Ocean Riley, Paul Willgoss (Children’s Heart Federation). Parents: Joanne Morley, Sarah Murray, Sandra Ramsey. Clinicians: Mr Chris Bond (Cardiac Surgery/Transplant, Birmingham), Dr Paul Clift (Adult Congenital Cardiology, Birmingham), Ms Carin van Doorn (Cardiac Surgery, Leeds), Sarah Finch (Nursing, Cardiff), Dr Katrijn Jansen (Adult Congenital/Transplant Cardiology, Newcastle), Dr Petra Jenkins (Adult Congenital Cardiology, Liverpool), Dr Simon MacDonald (Adult Congenital Cardiology, Cardiff), Dr Shruti Niraj (Clinical Psychology, Leicester), Dr Isma Rafiq (Adult Congenital Cardiology, Royal Brompton, London), Mr Serban Stoica (Cardiac Surgery, Bristol), Dr Lynne Williams (Non-ACHD Cardiology, Cambridge). James Lind Alliance: Katherine Cowan, Suzannah Kinsella, Maryrose Tarpey.
We are most grateful to George W Davies and family for funding and supporting this project. We thank Matthew Mangan and Shelley Parker at Birmingham Children’s Hospital Charity for facilitating and administering the funding. At the University of Birmingham, we thank Sharmaine Afferion for administering the project, and Shawn Mayall for managing the project website. We are grateful to Sophie Leonardi at the Centre for Ethnic Health Research, University of Leicester for advice on community engagement and disseminating the survey, and Nasima Miah for arranging translation. We thank the following for translation of the initial survey and posters: Bethan Simmonds (Welsh), Marta Pasikowska (Polish), Quratul-Ain Ahsan (Urdu), Shah Jalal (Bengali), Anishah Nathalia (Gujarati), and Gurpreet Santini (Hindi). We are grateful to Sophie Fitzgerald at the British Heart Foundation Young Person Support group for engaging young people with congenital heart disease in the surveys and workshops through their One Beat and Teen Heart groups. We thank Suzannah Kinsella and Maryrose Tarpey from the James Lind Alliance for facilitating the final workshops and Prof Gavin J Murphy, University of Leicester, for sharing his experience from the Adult Cardiac Surgery PSP.
We are grateful to our key partner organisations for supporting this project: The Children’s Heart Federation, Somerville Heart Foundation, British Congenital Cardiac Association (BCCA), Society for Cardiothoracic Surgery in Great Britain and Ireland (SCTS), and James Lind Alliance. We also thank our other partner organisations for publicising the surveys to their members and supporters: Little Hearts Matter, Tiny Tickers, Max Appeal, Birmingham Children’s Hospital Charity, Young at Heart, Paediatric Critical Care Society, Congenital Cardiac Anaesthesia Network, Paediatricians with Expertise in Cardiology Specialist Interest Group, Primary Care Cardiovascular Society, Society of Clinical Perfusion Scientists, Congenital Cardiac Nurses Association, British Adult Congenital Cardiac Nurse Association, British Heart Foundation Clinical Research Collaborative, and Centre for Ethnic Health Research. Finally we thank all those who responded to our surveys by posing or prioritising questions for research.
Initial survey data were collected and managed using REDCap electronic data capture tools hosted at the University of Birmingham. REDCap (Research Electronic Data Capture) is a secure, web-based application designed to support data capture for research studies, providing 1) an intuitive interface for validated data entry; 2) audit trails for tracking data manipulation and export procedures; 3) automated export procedures for seamless data downloads to common statistical packages; and 4) procedures for importing data from external sources.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @nigeledrury
Deceased 11 July 2022
Contributors NED and KC devised this Priority Setting Partnership, and NED and TJJ obtained funding. KC chaired the steering group, and all members formulated the summary questions. NED coded the electronic surveys and CPH performed the data analysis, with input from GB. All authors other than MJC were involved in writing and approval of the final manuscript. NED is acting as guarantor.
Funding This work was funded by George W Davies through a generous donation from the George Davies Charitable Trust to the Birmingham Children’s Hospital Charity. NED was funded by an Intermediate Clinical Research Fellowship from the British Heart Foundation (FS/15/49/31612).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.