Article Text

Abstract
Objective To examine risk factors for cardiac-related postacute sequelae of SARS-CoV-2 infection (PASC) in community-dwelling adults after acute COVID-19 infection.
Methods We performed a cross-sectional analysis among adults who tested positive for COVID-19. Outcomes were self-reported cardiac-related PASC. We conducted stepwise multivariable logistic regression to assess association between the risk factors (existing cardiovascular disease (CVD), pre-existing conditions, days since positive test, COVID-19 hospitalisation, age, sex, education, income) and cardiac-related PASC.
Results In a sample of 442 persons, mean (SD) age was 45.4 (16.2) years, 71% were women, 13% were black, 46% had pre-existing conditions, 23% had cardiovascular (CV) risk factors and 4% had CVD. Prevalence of cardiac PASC was 43% and newly diagnosed cardiac conditions were 27%. The odds for cardiac-related PASC were higher among persons with underlying pre-existing conditions (adjusted OR (aOR): 2.00, 95% CI: 1.28 to 3.10) and among those who were hospitalised (aOR: 3.03, 95% CI: 1.58 to 5.83).
Conclusions More than a third of persons with COVID-19 reported cardiac-related PASC symptoms. Underlying CVD, pre-existing diseases, age and COVID-19 hospitalisation are possible risk factors for cardiac-related PASC symptoms. COVID-19 may exacerbate CV risk factors and increase risk of complications.
- COVID-19
- epidemiology
- pericarditis
- risk factors
- coronary artery disease
Data availability statement
Data are available upon reasonable request. Deidentified data available upon reasonable request and following Johns Hopkins Medicine IRB data sharing permit (Phone: 410-502-2092, E-Mail: jhmeirb@jhmi.edu). Please contact the corresponding author (oogungb3@jh.edu) for additional information about the data request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Infection with SARS-CoV-2 virus may lead to persistent cardiac symptoms indicative of cardiac injury. COVID-19 may exacerbate cardiovascular disease (CVD) and pre-existing diseases.
WHAT THIS STUDY ADDS
Little is known about cardiac-related postacute sequelae of SARS-CoV-2 infection (PASC) in community-dwelling people. This study provides more evidence on PASC symptoms and cardiac conditions. Underlying CVD, pre-existing diseases, older age and COVID-19 hospitalisation may be risk factors for persistent PASC symptoms.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
These results highlight the need for concerted efforts to optimise primary care for cardiac PASC patients and prevent future complications.
Introduction
As of April 2022, there were 493 million COVID-19 cases worldwide and 80 million in the USA, resulting in nearly 6 million deaths globally and roughly a million in the USA.1 Postacute sequelae of SARS-CoV-2 infection (PASC) is a new and sometimes debilitating health condition in people with prior COVID-19.2 PASC is defined by the National Institutes of Health as the persistence of symptoms or sequelae beyond 3 weeks of SARS-CoV-2 infection onset.3 While these persistent symptoms are common among hospitalised patients, significantly less research has been conducted among non-hospitalised patients with ‘mild’ symptoms. PASC can potentially increase the risk of cardiovascular disease (CVD) and disability.4 Several health systems offer post-COVID clinics, but clinical care modalities guidelines, including public health strategies, to address PASC syndrome are grossly inadequate. This study presents results from COVID-19-infected community-dwelling adults. The study aimed to examine persistent cardiac-related symptoms in patients after acute COVID-19 illness.
Methods
The cardiac PASC study is an ongoing prospective study that began in 2021. This nested substudy includes a cross-sectional study of baseline data of adults enrolled in the Johns Hopkins COVID-19 Hopkins Opportunity for Participant Engagement (HOPE) Registry.5 6 This centralised database contains information on participants interested in COVID-19 studies at Johns Hopkins University. HOPE Registry participants are predominantly from the Baltimore–Washington, DC, metropolitan area who had COVID-19 testing at any Johns Hopkins health system sites.
Study sample
Participants from the HOPE Registry were eligible for the current study if they were: (1) at least 18 years old, (2) had ever tested positive for COVID-19, ascertained through electronic medical record (EMR) test records of positive SARS-CoV-2 reverse transcriptase PCR tests, (3) currently enrolled in the HOPE Registry, (4) provided informed consent and (5) willing to participate in the study. Exclusion criteria were: (1) adult participants who are unable to provide informed consent and (2) pregnant persons (ascertained through self-report). We invited participants to join the study in weekly batches through automated invitations generated in REDCap.
Sampling
This study used stratified sampling. The HOPE Registry has an over-representation of non-Hispanic white individuals (80%); therefore, we used stratified sampling by race and ethnicity to oversample non-white adults and obtain a sample reflective of the US race/ethnicity distribution. After applying eligibility criteria to HOPE Registry participants, we obtained a sample frame stratified by race/ethnicity with seven strata (race: white, black/African American, Asian, American Indian/Alaska Native, other races; ethnicity: Hispanic, non-Hispanic). We employed disproportionate sampling within the strata for black/African American, Asian, American Indian/Alaska Native, other races and Hispanic people, inviting 100% of them to join the study. We used proportional simple random sampling for non-Hispanic white stratum, inviting 60% of them to join the study (figure 1).

Flow diagram demonstrating inclusion and exclusion of participants in the study. aAmerican Indian or Alaska Native. bBlack or African American. cOther, unknown, prefer not to answer. dHispanic, Latino or Latina or Spanish origin. PACS, postacute sequelae of SARS-CoV-2 infection.
Recruitment
The invitations contained information about the study and survey entry links that were unique to each participant and could not be shared. Participants’ enrolment period was from November 2021 to January 2022. With a 70% survey response rate, we included 442 individuals in these analyses (figure 1). On survey completion, participants received a US$10 digital gift card in compensation through an automated process in REDCap.
Data collection and measurement
The baseline surveys asked about sociodemographic characteristics, COVID-19 testing, exposure, vaccinations, pre-existing conditions, persistent heart-related symptoms, cardiac conditions, fatigue and overall health. The baseline survey took 10–15 min. In addition, we ascertained COVID-19 testing date through EMR test records in the HOPE Registry.
Pre-existing cardiovascular (CV) risk factors, CVD and other conditions
We assessed pre-existing CVD by asking participants: “Before the COVID-19 pandemic (or before March 12, 2020), have you been diagnosed with any of the following? 1. hypertension, 2. High cholesterol, 3. coronary artery disease, 4. chronic ischemic disease, 5. heart failure, 6. valvular heart disease, 7. atrial fibrillation, etc.” Participants were encouraged to list other diagnosed CVD previously not listed, including other pre-existing conditions, such as stroke, diabetes mellitus, kidney disease, cancer, etc.
PASC symptoms and newly diagnosed cardiac conditions
At the time of survey administration, there were few validated tools for assessing PASC symptoms. Thus, we developed questionnaires on PASC symptoms based on symptoms reported in systematic reviews.7 8 We asked participants to indicate whether they had received any new cardiac diagnoses.
FACIT Fatigue Scale
We used the Functional Assessment of Chronic Illness Therapy (FACIT) Fatigue Scale (V.4), a short, 13-item tool that measures individuals’ fatigue levels during their usual daily activities over the past week. Total scores ranged from 0 to 52; lower scores indicated severe fatigue,9 and we also dichotomised the sum score using a recommended cut point of 34.10
Global health (PROMIS) Scale
We administered the Patient-Reported Outcomes Measurement Information System (PROMIS) Scale Global Health V.1.2, a 10-item scale representing the following 5 core health domains: physical health, pain, fatigue, mental health, social health and overall health.11 For the analysis, we obtained two sum scores. The General Mental Health Score for mental health was calculated from items 2, 4, 5 and 10; the General Physical Health Score for physical health was calculated from items 3, 6, 7 and 8. In addition, item 1 on general health and item 9 on the ability to carry out social activities were analysed as single items and not included in the sum score. Higher scores indicated better global mental/physical health.
Outcomes
Cardiac-related PASC, the primary outcome of this study, was defined as the presence of at least one cardiac PASC symptom≥3 weeks after a positive COVID-19 test. Symptoms included sharp or sudden chest pain, tachycardia or higher than normal pulse rate, feeling faint or heart palpitations.12 Due to the non-specificity of fatigue symptoms, we excluded fatigue from our definition of cardiac-related PASC. We calculated time since infection as the interval between the date of the COIVD-19 test and the survey consent date. We also assessed new diagnoses of CVDs through self-report based on participants’ answers to the question: “Since testing positive for COVID-19, has your healthcare provider newly diagnosed you with any of the following?” We computed the FACIT fatigue outcome as a sum score of the FACIT Fatigue Scale; the physical, mental and social functioning were computed from the Global Health PROMIS Scale.
Patient and public involvement
Patients or the public were not involved in the design, conduct, reporting, or dissemination plans of our research.
Statistical analysis
We performed a cross-sectional analysis of baseline data from an ongoing cohort study of persons who had tested positive for COVID-19. Following a missing data analysis, observations for the outcome variable determined to be missing at random were excluded from the final analysis (figure 1). Sample characteristics were visually summarised and assessed to identify distributions, outliers and missing data patterns. We reported categorical variables in frequencies and percentages and continuous variables in mean and SD or median (IQR or range) depending on the normalcy of distribution. Sociodemographic characteristics were summarised and stratified by cardiac-related PASC symptoms at enrolment outcome. The prevalence of the most reported cardiac-related PASC symptoms was summarised. Using test of proportions, we compared the prevalence of these symptoms at the 2 weeks post acute COVID-19 and on enrolment. A bivariate analysis was performed to examine what predictor variables were most associated with current reports of PASC and cardiac-related PASC symptoms.
Report of cardiac-related PASC symptoms≥3 weeks after positive COVID-19 test, current report of PASC symptoms, report of underlying CV symptoms and report of pre-existing conditions were examined as dichotomous variables (yes/no). We examined the association between underlying CV risk factors/CVD, and other pre-existing conditions and reports of cardiac-related PASC symptoms in crude logistic regression models. We then performed adjusted logistic regression analyses, including age, gender, race, education, household income and time since COVID-19 infection as covariates. Subsequently, we performed stepwise multivariable logistic regression with backward selection to assess the association between underlying CVD or risk factors and report of current cardiac-related PASC symptoms to permit statistical selection of the best predictor variables. We considered predictors with p<0.2 for inclusion in the stepwise multivariable logistic regression performed for the outcomes of this study.
We assessed the association between fatigue and cardiac-related PASC symptoms. We derived a sum score based on the FACIT Fatigue Scale and, using summary statistics techniques; we summarised the total sum score stratified by current cardiac-related PASC symptoms. We then dichotomised the sum fatigue score into two categories (severe fatigue/less severe fatigue), using the recommended 34-point cut point.10 We performed multivariable logistic regression analyses for the relationship between fatigue and cardiac-related PASC symptoms. We obtained sum scores for mental and physical health functioning separately and assessed for differences in means scores using t-tests by report of cardiac-related PASC symptoms.
To further examine the temporal presentation of cardiac-related PASC symptoms, time since COVID-19 infection was divided into categories of 6 months (ie, 0–5 months, 6–11 months, 12–17 months and ≥18 months), and we plotted the prevalence of current cardiac-related PASC symptoms for each of these time bins. We also reported the prevalence of newly diagnosed conditions after recovery from COVID-19, stratified by time since infection (dichotomised into<18 months and≥18 months). P<0.05 was considered statistically significant. Data analyses were conducted in Stata I/C V.16.1, and R V.2021.09.0 (R project or statistical computing).
Results
As of November 2021, 1997 adults with previous COVID-19 infection from the HOPE Registry were eligible for this study and survey invitations were sent to 717 of them After accounting for incomplete outcomes responses and missing data, we included 442 (88%) of 505 participants in the analyses (figure 1). Table 1 shows sociodemographic characteristics stratified by cardiac-related PASC symptoms. At enrolment, the mean (SD) age was 45.4 (16.2) years, 71% were women, 13% were black and 29% had underlying CV risk factors (23%) and CVD (4%). In the sample, 43% reported current cardiac-related PASC symptoms; only 12% reported being hospitalised for COVID-19, and median (IQR) time since infection was 12.4 (10.0–15.2) months. About 10.5% were unvaccinated, and among those who had received at least one dose of the COVID-19 vaccine (400, 90.5%), 56.7% had received a booster dose.
Sociodemographic characteristics stratified by report of current cardiac-related PASC symptoms (N=442)
Prevalence of cardiac-related PASC symptoms
Almost 52% of the sample (228/442) had cardiac-related PASC symptoms 3 weeks or more after acute infection; 43% reported symptoms at enrolment (figure 2). Heart palpitations were the most reported symptom (22.6% vs 14.5%, p0.05), followed by tachycardia (20.6% vs 12.9%, p<0.05). Feeling faint was also common (18.6% vs 10.9%, p<0.05), followed by persistent chest pain (14.3%) and acute chest pain (12.4% vs 8.6%, p=0.062). Between the immediate postinfection period (beyond 2 weeks of recovery) and at survey administration, most symptoms improved (mean of 12 months for time since infection). Fatigue (42.3%), joint pain (26.7%), muscle pain (24.2%), shortness of breath (20.4%) and exercise intolerance were also common (17.7%).

Prevalence of cardiac-related post acute sequelae of SARS-CoV-2 infection symptoms, comparing beyond 2 weeks post acute COVID-19 and at survey administration (N=442).
Risk factors for cardiac-related PASC symptoms
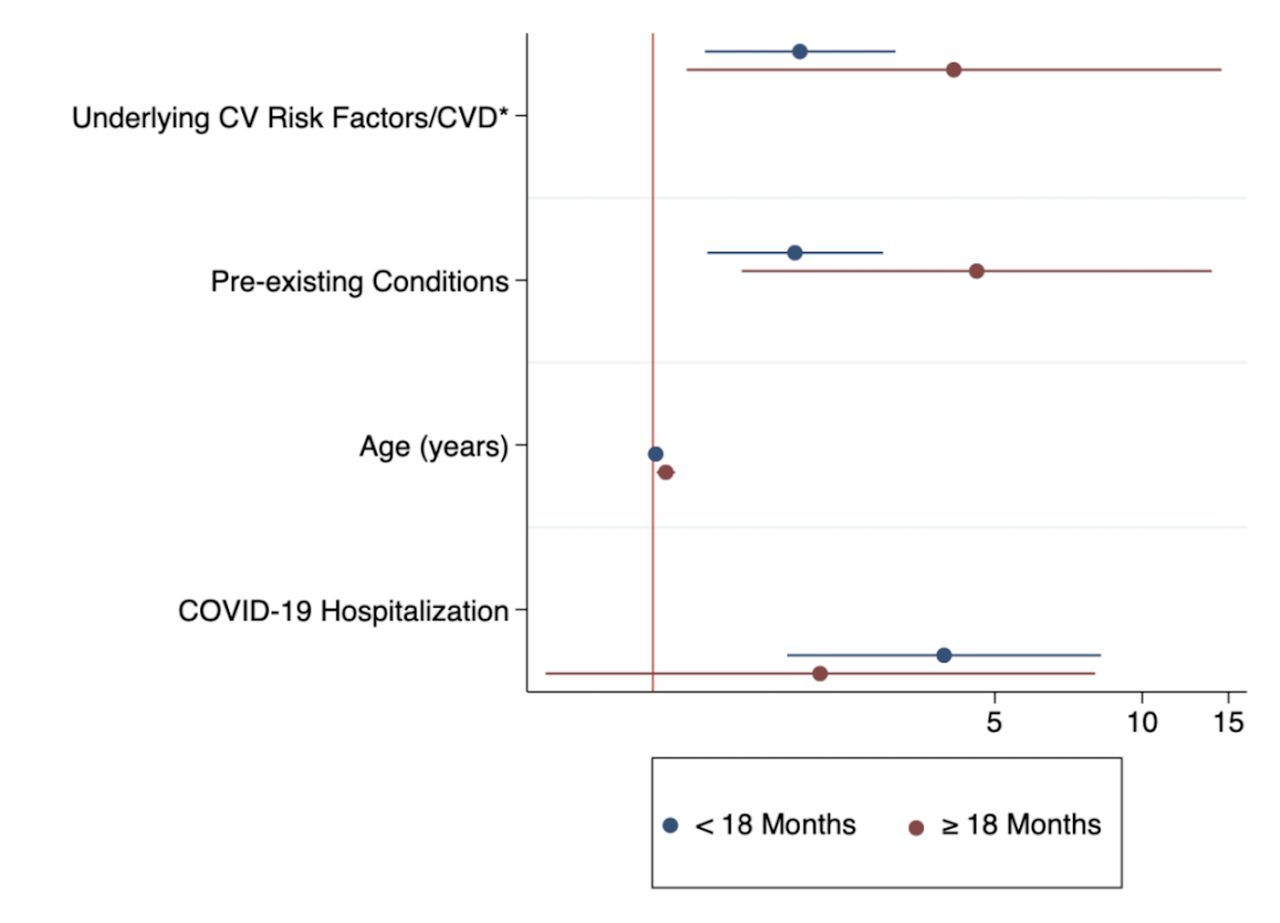
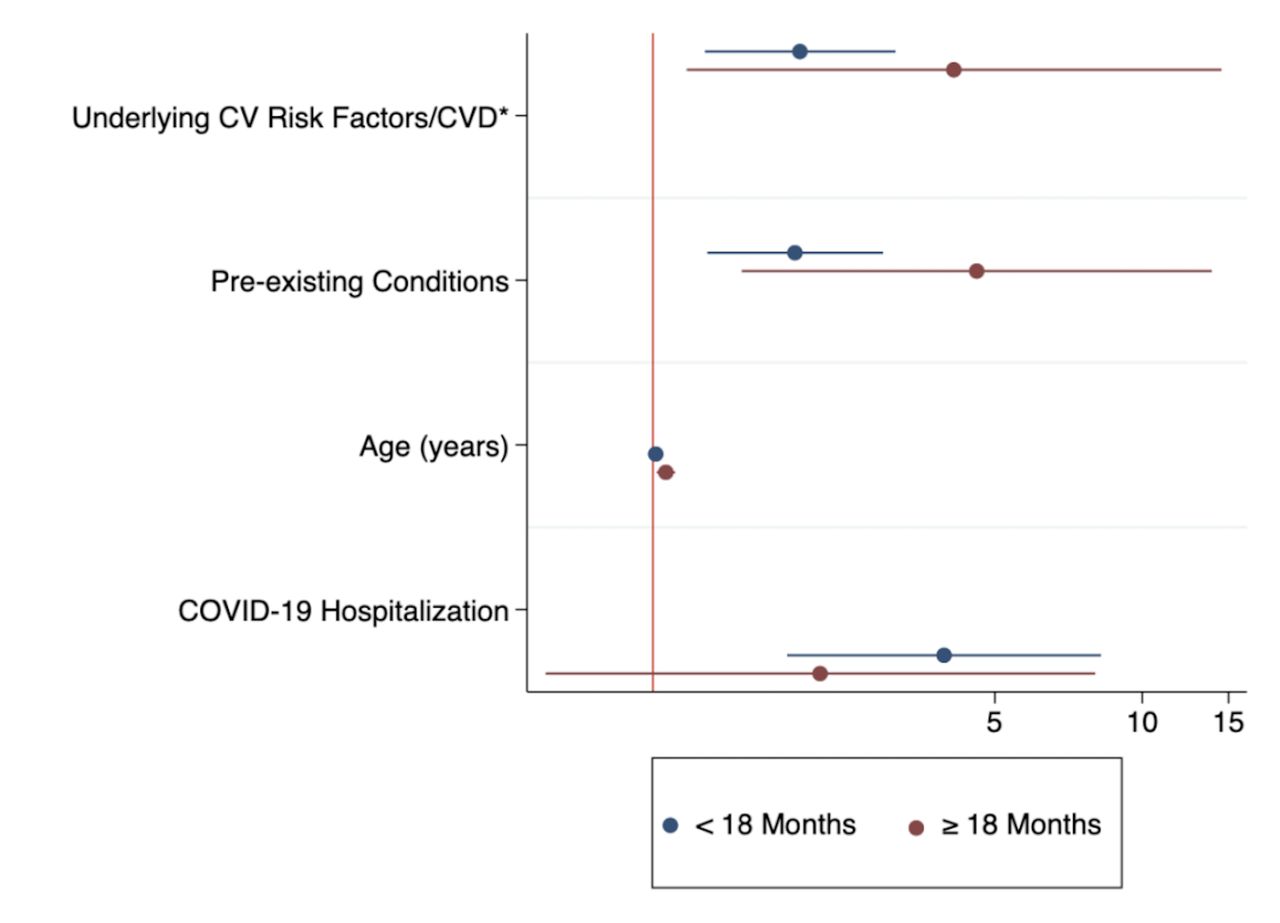
Univariable analyses showed a statistically significant association between underlying CVD, pre-existing conditions, age, COVID-19 hospitalisations and cardiac-related PASC symptoms (figure 3). PASC prevalence by time since COVID-19 infection (0–5 months, 6–11 months, 12–17 months, and 18 months) showed a high prevalence after 12 months of recovery (online supplemental figure 1).
Supplemental material
{kind=link}
{kind=link}
{kind=link}
Univariate analysis for factors associated with current cardiac-related PASC symptoms, stratified by months since positive test (<18 months vs ≥18 months). *CV risk factors included hypertension and dyslipidemia; CVD included coronary artery disease, heart failure, atrial fibrillation, chronic ischaemic heart diseases, myocardial infarction, valvular heart disease, etc. CV, cardiovascular; CVD, cardiovascular disease.
Table 2 shows univariate and multivariable logistic regression results. After adjusting for race, income, education and days since a positive test in the final stepwise model, the odds of cardiac-related PASC symptoms were two times higher in persons with CVD (aOR: 2.01, 95% CI: 1.27 to 317), and in persons with existing pre-existing conditions(aOR: 2.00, 95% CI: 1.28 to 3.10). Every one-year increase in age was associated with increased odds of reporting cardiac-related PASC (aOR: 1.02, 95% CI: 1.01 to 1.03). Persons hospitalised for COVID-19 were more likely than those who were never hospitalised for COVID-19 to report cardiac-related PASC symptoms (aOR: 3.03 95% CI: 1.58 to 5.83).
Association between risk factors and self-report of cardiac-related PASC symptoms
Newly diagnosed cardiac conditions and risk factors
After recovering from acute COVID-19, 26.9% (119/442) of individuals reported a new cardiac condition; 20% had newly diagnosed hypertension, 24% had tachycardia and 13% had postural orthostatic tachycardia syndrome (POTS) (online supplemental table 1). Persons who had a ≥18 months recovery from acute COVID-19 infection were more likely to report diagnosis of tachycardia (p<0.05) and myocarditis (p<0.05).
Supplemental material
Fatigue and global health functioning
The most common symptom was fatigue (42.3%). The overall mean fatigue score was 26.4 (±13.0); persons with cardiac-related PASC were more likely to report fatigue (−13.11, 95% CI: –15.25 to –10.98, p<0.001). Using the recommended 34-point cut-off point,10 88% of the participants reported experiencing fatigue. Those with present cardiac-related PASC symptoms were more likely to report fatigue (aOR: 9.32, 95% CI: 5.54 to 15.66) than those without. This was also evident for persons who were hospitalised (aOR: 4.06, 95% CI: 2.12 to 7.78). We assessed global functioning using the PROMIS Global Health Scale; the mean mental health score was lower among those reporting cardiac-related PASC symptoms at enrolment (−1.90, 95% CI: −2.27 to –1.53, p<0.001). Persons reporting cardiac-related PASC symptoms had lower physical health functioning (−1.44, 95% CI: −1.87 to –1.01, p<0.001).
Discussion
The spectrum of cardiac-related PASC—particularly in community-dwelling persons with acute COVID-19 infection not requiring hospitalisation—and its CV implications remains unclear. In our study, more than a third of persons with COVID-19 reported probable cardiac-related PASC symptoms with a mean time since infection of 12 months, highlighting the virus’s longer-term impact. More than a quarter reported new-onset cardiac risk factors and diseases post-acute COVID-19 infection. Heart palpitations, tachycardia, fainting and chest pain were common PASC symptoms. Older age, CV risk factors and CVD, and acute COVID-19 infection were risk factors for cardiac-related PASC symptoms. People with probable cardiac-related PASC symptoms reported increased fatigue, decreased physical and mental functioning, and lower quality of life.
We found cardiac-related PASC to be prevalent, with significant symptoms lasting for months post infection. Cardiopulmonary symptoms have been reported in up to 89% of non-hospitalised patients following acute COVID-19 infection.13 Our findings revealed that non-hospitalised persons have persistent symptoms. About 52% reported probable cardiac-related PASC symptoms after 3 weeks following positive COVID-19 test; 43% reported persistent cardiac-related PASC symptoms 12 months post acute infection. This is similar to other studies that found persisting effects of COVID-19, including an elevated risk for CVD 12 months after acute infection.2 14 15 According to a recent American College of Cardiology report, it remains unclear whether there are major distinctions in the underlying mechanisms, evaluation or management comparing cardiac-related PASC symptoms in the immediate postacute period and symptoms extending beyond 12 months.16
The high prevalence of cardiac-related PASC and CVD in our study was observed in a relatively young population (sample mean age: 45.4 years). This is consistent with previous studies that have documented several cardiac abnormalities assessed on transthoracic echocardiography in patients diagnosed with PASC, under 55 years, with no prior history of CVD.17 18 However, our findings also showed increasing age was associated with reports of cardiac PASC. This is consistent with other findings showing a higher incidence of PASC with older age.19 20 Possible explanations for this include lower levels or reduced expression of ACE2 and upregulation of angiotensin II proinflammatory signalling with older age, which becomes exaggerated in the presence of the SARS-CoV-2 and increases the risk of greater COVID-19 severity and death with advancing age.21 Additionally, age is known to be associated with deterioration in CV functionality; older adults are already at higher risk of CV risk factors and CVD,22 thus, COVID-19 and its sequelae may play a role in multiplying the magnitude of this risk or accelerating the symptomology. The underlying mechanisms of older age and PASC are still poorly understood and an important literature gap.
Over a quarter of research participants reported new CV risk factors and cardiac conditions such as hypertension after COVID-19 infection. This finding should be interpreted with caution due to the variability in clinical presentation of cardiac-related PASC. Among 73 455 non-hospitalised patients in the US Department of Veterans Affairs health services, there was a high risk of incident CVD beyond 30 days of infection (hypertension, HR: 15.18 (95% CI: 11.53 to 18.62); cardiac dysrhythmias, HR: 8.41 (95% CI: 7.18 to 9.53)); circulatory signs and symptoms, HR: 6.65 (95% CI: 5.18 to 8.01); chest pain, HR: 10.08 (95% CI: 8.63 to 11.42); coronary atherosclerosis, HR: 4.38 (95% CI: 2.96 to 5.67); and heart failure, HR: 3.94 (95% CI: 2.97 to 4.80)).23 The most reported newly diagnosed conditions in our study were tachycardia, hypertension and POTS. There is growing evidence of POTS diagnoses following COVID-19; a cross-sectional study of COVID-19 survivors reported a 19% prevalence of POTS diagnosis in 802 survivors.14 These results have significant implications for people with PASC and for already strained health resources, systems and workers.24 This emphasises the need for coordinated, transdisciplinary approaches to management, including population-level and individual-level interventions to support recovery.
CV evaluation and diagnostic methods for PASC patients would be advantageous, especially for patients who were not hospitalised for COVID-19. Mobile heart rhythm tracking devices, Holter ECG monitoring for arrhythmias and abnormal pulse reactions, and heart rate assessments are non-invasive outpatient diagnostic techniques to characterise symptomatic tachycardia and other cardiac symptoms associated with PASC.25 There is a need for specific recommendations and policies to help with diagnosis and management of PASC, particularly considering the anticipated fiscal impact of PASC on population productivity. As mechanisms for enduring cardiac injury postacute COVID-19 are poorly understood, additional investment in under-resourced communities most hit by COVID-19 infections and PASC is critical.4
Our findings have important clinical implications. The strong association observed for underlying CV risk factors and diseases, pre-existing conditions, increasing age and previous COVID-19 hospitalisation imply that persons within this profile may benefit from additional diagnostic evaluation and early interventions. These findings also provide further insight on CVD and PASC, which may facilitate clinical judgement and identification of patients who may benefit from imaging and comprehensive CV diagnostic procedures.16 Results from this study will inform risk stratification processes to identify persons at risk for CVD complications resulting from COVID-19 in the community. Investment in cardiac-related PASC research is vital for informing new therapy methods. Also needed are coordinated efforts to optimise primary care for people with cardiac PASC and prevent CV events and consequences.15 Several tertiary medical centres have postacute COVID-19 clinics, but referrals are not readily available, further underscoring the importance of investing in primary care for equitable PASC care.4 This includes the need for population-level strategies to address the rising burden of CVD attributable to COVID-19.
Limitations
Lack of temporality is a major limitation in our observational study; hence, causal inference cannot be ascertained. Another limitation is that our data were based on self-report with non-ascertainment of reported CVD diagnoses or reported symptoms through EMR chart review. Nevertheless, self-report is an acceptable method of data collection in epidemiological studies and may be used as a proxy in the absence of EMR data.26 Additionally, echocardiography and detailed cardiac imaging, which allows for assessment of ventricular function and wall motion abnormalities were not performed.We also note that uncertainty regarding the mechanistic link between the reported cardiac PASC symptoms and COVID-19 infection as another limitation. Selection bias is another potential limitation since we recruited participants from the HOPE Registry, which had an over-representation of white adults. We addressed this by employing stratified sampling technique by race/ethnicity strata, to obtain a sample reflective of the US race/ethnicity distribution.
Our study has several strengths. First, the majority of our sample includes non-hospitalised patients and community-dwelling persons with PCR-confirmed COVID-19 diagnoses, unlike many other studies based on hospitalised patients. Also, we recruited participants interested in joining COVID-19 studies from a COVID-19 registry with a response rate of 70%. Additionally, we provided information on cardiac-specific symptoms by evaluating all cardiac PASC symptoms as a group, rather than as individual symptom outcomes.
Conclusion
In conclusion, among the sample of community-dwelling adults diagnosed with COVID-19, we estimated the burden of possible cardiac-related PASC symptoms to be 43%, and the diagnosed cardiac conditions, including hypertension was around 27%. Our findings suggest that underlying CVD, pre-existing conditions, older age and COVID-19 hospitalisation, may be risk factors for persistent cardiac-related PASC symptoms. Hence, COVID-19 may play an important role in worsening the prognosis of existing CVD and pre-existing conditions and in increasing the risk of complications.
Data availability statement
Data are available upon reasonable request. Deidentified data available upon reasonable request and following Johns Hopkins Medicine IRB data sharing permit (Phone: 410-502-2092, E-Mail: jhmeirb@jhmi.edu). Please contact the corresponding author (oogungb3@jh.edu) for additional information about the data request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants. Ethical approval for the present study was obtained from the Johns Hopkins Medicine Institutional Review Board (IRB00299548). Participants gave informed consent to participate in the study before taking part.
Acknowledgments
We would like to thank the cardiac PASC study participants. We also thank Cassie Lewis-Land, Scott Carey, Mike Sherman and the Institute of Clinical and Translational Research Recruitment Innovation Team for technical support during data collection.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors OO contributed to the inception of the study, development of study ideas, study design acquisition and linkage of data, undertook the data analysis, wrote the first draft of the paper. YC-M, PMD, WSP and CRDH contributed to the inception of the study, development of the study ideas, study design, advised on the interpretation of the results and drafting of the paper. JEF and NAG contributed to the study design and advised on the analysis, advised on the interpretation of the results and drafting of the paper. YC-M, PMD, WSP, CDH, JEF and NAG critically reviewed the paper. OO is responsible for the overall content as guarantor. All authors have approved the submitted version. The corresponding author attests that all listed authors meet authorship criteria and that no others meeting the criteria have been omitted.
Funding This work was supported in part by National Heart, Lung and Blood Institute (6793-02-S017) as part of the NIH Community Engagement Alliance Against COVID-19 Disparities. YC-M is supported by the American Heart Association Health Equity Research Network Project: Prevention of Hypertension, Grant number: 882415, National Institute of Minority Health and Health Disparities (1P50MD017348-018183) and the National Institute of Nursing Research (P30NR018093). OO is supported by the Johns Hopkins School of Nursing discovery and innovation fund, the P.E.O. International Peace Scholarship and the NLN Nursing Education Scholarship Fund. NAG receives COVID-19-related research funding from Bentivoglio Family Fund and Post-acute COVID-19 Syndrome Discovery Fund of the Johns Hopkins University, and the Johns Hopkins Specialized Center for Research Excellence in Sex Differences (U54AG062333) and The Foundation for Gender-Specific Medicine. JEF receives COVID-19 related research funding from the Johns Hopkins Center for AIDS Research (JHU CFAR) RADx-UP funded through the NIH (3P30AI094189-10S1), and the Community Collaboration to Combat Coronavirus (C-Forward)—Provost Award—Johns Hopkins University COVID Community Research Initiative.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.