Article Text

Abstract
Objective A novel artificial intelligence-based phenotyping approach to stratify patients with severe aortic stenosis (AS) prior to transcatheter aortic valve replacement (TAVR) has been proposed, based on echocardiographic and haemodynamic data. This study aimed to analyse the recovery of extra-aortic valve cardiac damage in accordance with this novel stratification system following TAVR.
Methods The proposed phenotyping approach was previously established employing data from 366 patients with severe AS from a bicentric registry. For this consecutive study, echocardiographic follow-up data, obtained on day 147±75.1 after TAVR, were available from 247 patients (67.5%).
Results Correction of severe AS by TAVR significantly reduced the proportion of patients suffering from concurrent severe mitral regurgitation (from 9.29% to 3.64%, p value: 0.0015). Moreover, pulmonary artery pressures were ameliorated (estimated systolic pulmonary artery pressure: from 47.2±15.8 to 43.3±15.1 mm Hg, p value: 0.0079). However, right heart dysfunction as well as the proportion of patients with severe tricuspid regurgitation remained unchanged. Clusters with persistent right heart dysfunction ultimately displayed 2-year survival rates of 69.2% (95% CI 56.6% to 84.7%) and 74.6% (95% CI 65.9% to 84.4%), which were significantly lower compared with clusters with little or no persistent cardiopulmonary impairment (88.3% (95% CI 83.3% to 93.5%) and 85.5% (95% CI 77.1% to 94.8%)).
Conclusions This phenotyping approach preprocedurally identifies patients with severe AS, who will not recover from extra-aortic valve cardiac damage following TAVR and whose survival is therefore significantly reduced. Importantly, not the degree of pulmonary hypertension at initial presentation, but the irreversibility of right heart dysfunction determines prognosis.
- aortic valve stenosis
- transcatheter aortic valve replacement
- echocardiography
Data availability statement
Data are available upon reasonable request. The data underlying this article will be shared on reasonable request to the corresponding author. All requests for raw and analysed data and related materials, excluding programming code, will be reviewed by the Ethics Committee at Technical University of Munich, Germany. Any data and materials that can be shared will be released via a Material Transfer Agreement.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What is already known on this topic
We have previously proposed a machine learning framework that enables to assign patients with severe aortic stenosis (AS) to distinct clusters based on their echocardiographic and haemodynamic characteristics—this novel phenotyping approach differs from previous approaches for risk stratification, because it does neither hypothesise a linear sequence of accumulated pathologies caused by severe AS (potentially ignoring the aggravating impact of comorbidities), nor does it stratify patients into low-risk and high-risk cohorts in accordance with a single variable’s dichotomy (prone to oversimplification).
What this study adds
We hereby present cluster-related echocardiographic follow-up data in order to illustrate the trajectory of cardiopulmonary recovery or further decline after transcatheter aortic valve replacement (TAVR).
Importantly, TAVR elicited favourable effects on left heart haemodynamics and significantly ameliorated pulmonary artery pressures, but structural and functional alterations of the right heart persisted in patients assigned to clusters with a high prevalence of chronic obstructive pulmonary disease and atrial fibrillation and/or flutter, ultimately resulting in distressing survival rates.
How this study might affect research, practice or policy
This study proposes a comprehensible classification system for patients suffering from multiple comorbidities besides severe AS and also gives an outlook on how the extra-aortic valve cardiac damage in distinct patient phenotypes will evolve after TAVR.
Since right-sided cardiac damage including severe tricuspid regurgitation persists after TAVR and ultimately limits prognosis, our study emphasises the need for additional treatments such as transcatheter tricuspid valve interventions.
Ideally, patients with severe AS would be treated before the occurrence of irreversible damage—future studies investigating the benefit of earlier TAVR strategies are therefore awaited with great anticipation.
Introduction
Patients with severe aortic stenosis (AS) typically present with significant clinical heterogeneity, owing to the extent of disease progression, prevalence of comorbidities and possibly also due to genetic predisposition.1 Placing the AS severity in the contextual anatomical and functional variability of cardiac and pulmonary circulatory impairments therefore holds the promise to refine both diagnostic and prognostic resolution. Recently, Généreux et al proposed a staging classification to grade the extra-aortic valve cardiac damage subsequent to severe AS by hypothesising a sequential order of accumulated pathologies such as left ventricular dysfunction, mitral regurgitation (MR) and left atrial enlargement, pulmonary hypertension (PH) and ultimately right heart failure.2 Distinguishing the five stages of disease progression among the patients’ collective of the PARTNER trial, the authors could demonstrate that rising stages as assessed prior to transcatheter aortic valve replacement (TAVR) translated into increased mortality. Physicians yet commonly encounter a disparity between AS-induced haemodynamic burden and extra-aortic valve cardiac damage, as a plethora of potentially unmodifiable comorbidities such as chronic obstructive pulmonary disease (COPD) can also result in PH and eventually right heart failure. A novel classification system based on unsupervised agglomerative, hierarchical clustering in conjunction with an artificial neural network (ANN) was therefore established to comprehensively capture the complexity of cardiopulmonary impairments, without inferring causality nor hypothesising a sequential progression of accumulated pathologies upstream of the causative AS.3
Importantly, both PH and right heart dysfunction can persist in a substantial number of cases after TAVR.4–7 Moreover, postprocedural decline of right ventricular function and/or worsening of tricuspid regurgitation (TR) despite correction of AS are associated with a dismal prognosis.8 9 Obviously, it does not require sophisticated skills to assign a poor prognosis to patients with worsening cardiac status after intervention. For refined prognostic assessment, however, the trajectory of right heart function towards recovery or further decline must ideally be predicted prior to TAVR, but no study has adequately addressed this issue to date.
The aim of this study was therefore to shed light on the trajectory of cardiopulmonary impairments after TAVR in accordance with the previously established classification system based on unsupervised clustering.3 Ideally, this artificial intelligence-based phenotyping approach could serve the paramount aim to preprocedurally identify patients, who will suffer from persistent right heart dysfunction after TAVR and who will hence decease earlier unless specifically treated.
Methods
Study population
This is a retrospective cohort study drawing on prospectively and systematically collected echocardiographic and haemodynamic data from patients with severe AS. Enrolled patients underwent TAVR for severe AS at two tertiary centres in Munich, Germany, between January 2014 and December 2020. Patients were included in the registry only after written informed consent was received. Since this study aimed to analyse the extent of extra-aortic valve cardiac damage subsequent or parallel to severe AS in depth, only patients with both, preprocedural echocardiography and right heart catheterisation, obtained prior to TAVR, were included in this study. Follow-up echocardiography was routinely performed 6 months after TAVR, unless specific interests (eg, diagnostic evaluation of cardiac decompensation) justified an earlier or repeated investigation. As an elderly patient population was studied, postprocedural 2-year all-cause mortality was defined as a clinically meaningful primary outcome measure. Survival data (lastly requested in January 2022) were obtained from the German Civil Registry in case of patients being registered in Germany (96.7%), or from general practitioners, hospitals and practice cardiologists for patients from foreign countries. Planned and conducted in conformity with the Declaration of Helsinki, this study was approved by the local ethics committee.
Statistical analysis
All statistical analyses were performed using R statistical software (R V.3.6.3; R Foundation for Statistical Computing, Vienna, Austria; see online supplemental table 1 for a complete list of employed R packages).
Supplemental material
Categorical variables are presented as numbers and/or frequencies (%), and continuous variables are given as means±standard deviation (SD) and 95% confidence interval (CI). χ2 or Fisher’s exact test were used to evaluate the association between categorical variables, and Kruskal-Wallis test in combination with pairwise Wilcoxon test with correction for multiple testing (Benjamini-Hochberg method) was used for comparison of continuous variables, as appropriate. Pairwise comparisons of preprocedural and postprocedural data among clusters were calculated by paired samples Wilcoxon test.
For analysis of collinearity, Pearson’s correlation coefficients were calculated.
Survival was illustrated using the Kaplan-Meier method, and a Cox proportional hazards model was further used to estimate hazard ratios (HR) between identified clusters.
The methodology for unsupervised clustering of patients and subsequent training of an ANN has been extensively described elsewhere.3 In summary, the previous work performed a two-step experiment with the paramount goal of establishing a man-machine interaction-based phenotyping approach for patients undergoing TAVR for severe AS as follows:
In a first step, we aimed to detect clinically meaningful phenotypes with regard to 2-year all-cause mortality by applying unsupervised agglomerative clustering to preprocedurally obtained echocardiographic and right heart catheterisation data (unsupervised machine learning experiment).
Since the first experiment was designed to segregate patient subsets as distinct cardiac phenotypes, but the clustering approach would not allow to assign any future patient to the just defined clusters, we additionally employed an ANN for prospective patient-to-cluster assignment (supervised machine learning experiment). Those variables from preprocedural echocardiography and right heart catheterisation, which proved most suited for the clustering approach, also served as input parameters for the ANN.
To compare our unsupervised agglomerative, hierarchical clustering approach with an established model of sequential disease progression, the staging classification from Généreux et al2 was modified by partitioning patients into four stages of disease progression based on the extent of extra-aortic valvular cardiac damage. Prior to allocating patients into one of these four stages, missing values required for classification were imputed by an established random forest algorithm,10 but were not used hereinafter again.
A p value ≤0.05 was considered to indicate statistical significance.
Results
Follow-up echocardiography from 247 out of 366 patients (67.5%) allows to construct representative trajectories for postprocedural recovery or further decline of cardiac function in accordance with cluster assignment
The clustering approach as well as the emerging cluster-related phenotypes have already been described by our group previously.3 In brief, four clusters with distinct echocardiographic and haemodynamic characteristics—possibly evolved under the contributing influence of comorbidities such as COPD and atrial fibrillation—were unravelled (graphical abstract, tables 1 and 2):
Supplemental material
Patients in cluster 1 (n=164) presented with preserved cardiac function (left ventricular ejection fraction (LVEF): 57.2±6.36 (95% CI 56.3 to 58.2)%) and normal pulmonary artery pressures (mean pulmonary artery pressure (mPAP): 21.2±6.54 (95% CI 20.2 to 22.2) mm Hg).
In contrast, patients in cluster 2 (n=66) featured elevated pulmonary artery pressures (mPAP: 34.2±7.76 (95% CI 32.2 to 36.1) mm Hg) but a still preserved right ventricular systolic function (tricuspid annular plane systolic excursion (TAPSE): 21.3±3.52 (95% CI 20.4 to 22.2) mm) and a low rate of severe TR (2 out of 66 patients; 3.03%).
Left heart failure (LVEF: 42.4±15.7 (95% CI 37.6 to 47.1)%), severe PH (mPAP: 46.9±8.54 (95% CI 44.3 to 49.5) mm Hg) and right heart dysfunction (TAPSE: 16.1±4.57 (95% CI 14.7 to 17.5) mm) characterised patients in cluster 3 (n=45). A "classical" low-flow, low-gradient AS was found in 21 out of 45 patients (46.7% vs 6.10%, 4.55% and 28.6% in clusters 1, 2 and 4, respectively; p value: 6.1×10–13). Moreover, 24.4% of patients from cluster 3 were diagnosed with COPD (in comparison to 8.54%, 15.2% and 15.4% in clusters 1, 2 and 4, respectively; p value: 0.0376).
Interestingly, patients from cluster 4 (n=91) showed mild postcapillary PH (mPAP: 27.5±9.15 (95% CI 25.6 to 29.4) mm Hg), yet dilatation of all heart chambers, biventricular dysfunction (LVEF: 47.3±12.2 (95% CI 44.7 to 49.9)%; TAPSE: 16.8±4.46 (95% CI 15.9 to 17.8) mm), and a high prevalence of both MR and TR (12.1% and 14.3%, respectively). Besides a high prevalence of atrial fibrillation and/or flutter (75.8%), patients from cluster 4 also presented with highest age at diagnosis (81.3±6.73 years vs 79.6±5.96, 78.1±6.91 and 79.8±8.73 years in clusters 1, 2 and 3, respectively; p value: 0.0068).
Demographic and clinical characteristics in accordance with cluster assignment
Comparison of preprocedural echocardiographic and haemodynamic characteristics in accordance with cluster assignment
Concomitant to elevated pulmonary artery pressure levels and impaired right heart systolic function, right ventricular to pulmonary artery coupling expressed as TAPSE/sPAP ratio was significantly reduced in patients from clusters 3 and 4 (table 2, online supplemental figure 1).
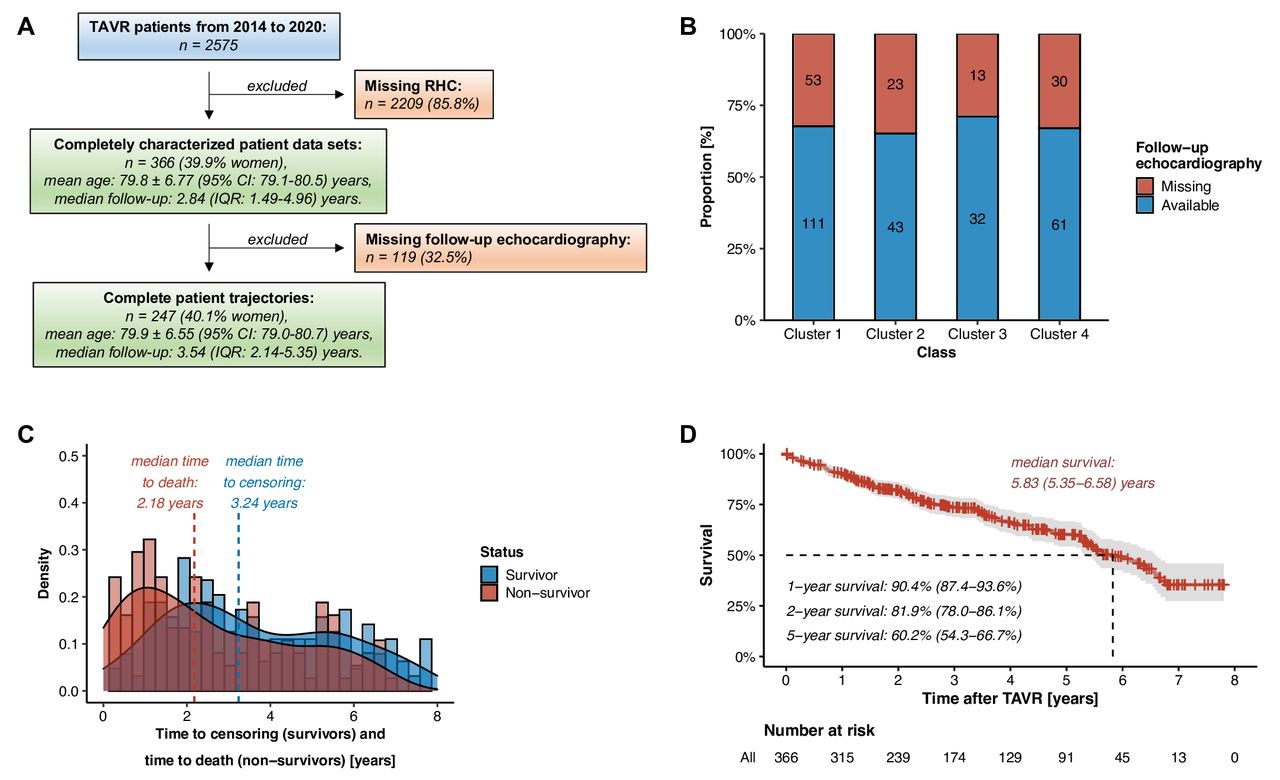
Among the initial patient cohort of 366 patients with complete echocardiography and right heart catheterisation data obtained prior to TAVR (see the previous work demonstrating the representative character of this study population), follow-up echocardiography was available for 247 patients (67.5%) (figure 1A). Importantly, equal proportions of follow-up echocardiography were found among the clusters (figure 1B), and also the time from TAVR to follow-up echocardiography was statistically indifferent among the clusters (mean time from TAVR to follow-up echocardiography: 147±75.1 (95% CI 138 to 157) days; online supplemental figure 2). On a median follow-up time of 2.84 years (interquartile range 1.49 to 4.96 years), 135 deaths among 366 patients were recorded. Fifty percent of deaths occurred within 2.18 years after TAVR (figure 1C). Median survival among the 366 patients from the initial cohort ranged at 5.83 (95% CI 5.35 to 6.58) years (figure 1D).
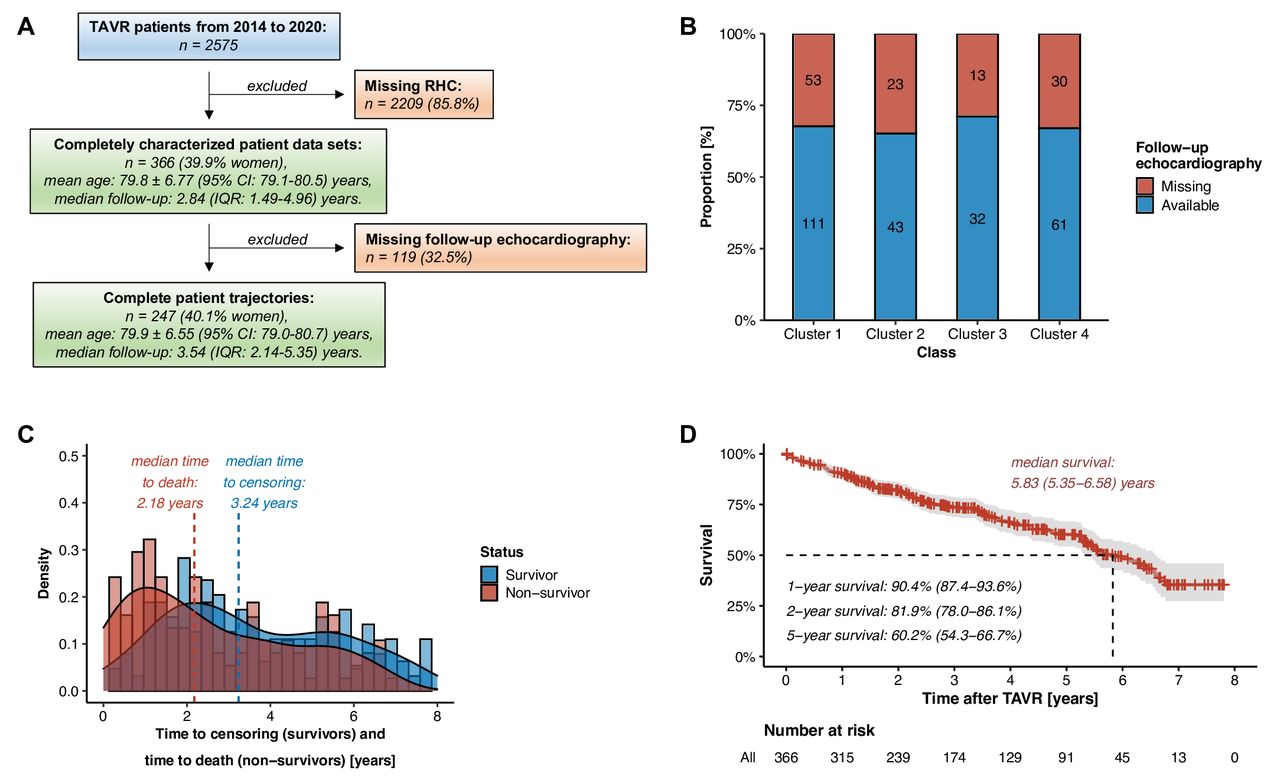
General information about the study population from recruitment to follow-up. (A) Flow chart for patient recruitment. (B) Proportion of patients with valid follow-up echocardiography data among clusters. (C) Density plot illustrating time to death and time to censoring for the entire study population. (D) Kaplan-Meier survival plot for the entire study population. IQR: interquartile range; RHC, right heart catheterisation; TAVR, transcatheter aortic valve replacement.
Correction of severe AS by TAVR exerts beneficial effects on concurrent severe MR and reduces pulmonary artery pressures, but right heart dysfunction and severe TR cannot be reversed
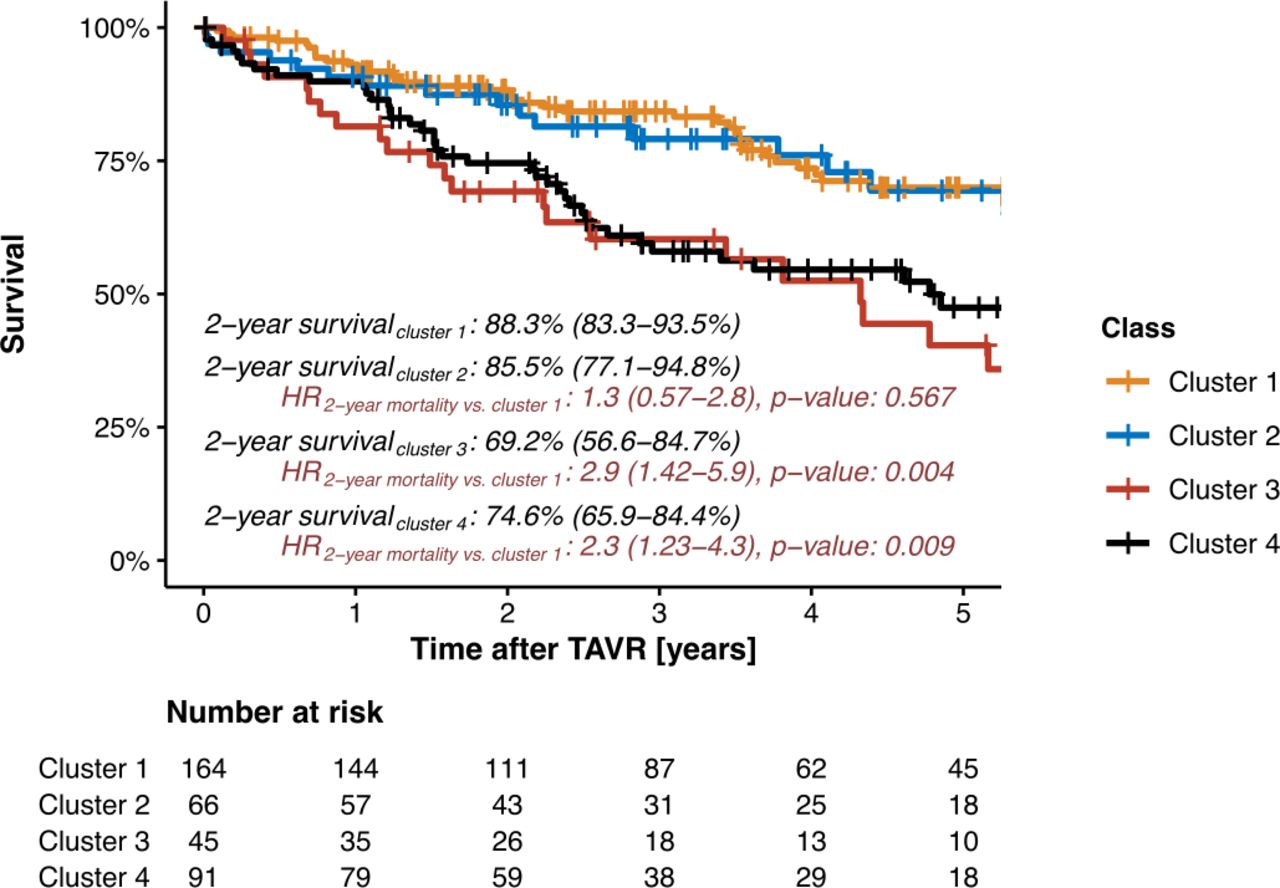
Irrespective of cluster assignment, follow-up echocardiography revealed that correction of AS reduced the prevalence of concurrent severe MR (MR prevalence preprocedural: 9.29% vs MR prevalence postprocedural: 3.64%, p value: 0.0015) and ameliorated the backward transmission of elevated left-sided filling pressures to the pulmonary circulation as expressed in a reduction of echocardiographic estimations of systolic pulmonary artery pressures (sPAP; sPAPpreprocedural: 47.2±15.8 (95% CI 45.4 to 49.1) mm Hg vs sPAPpostprocedural: 43.3±15.1 (95% CI 41.2 to 45.4) mm Hg, p value: 0.0079) (table 3). However, no general improvements of right heart function or structure could be observed. This is of particular importance for patients in clusters 3 and 4: at follow-up, these patients presented with impaired right ventricular systolic function (TAPSE: 15.9±4.47 (95% CI 14.3 to 17.5) mm and 17.6±4.25 (95% CI 16.5 to 18.7) mm, respectively) and with a persistently high prevalence of severe TR (31.2% and 14.8%, respectively) (table 4, figure 2). Finally, patients from clusters 1 and 2 with little or no persistent cardiopulmonary impairments showed a 2-year survival of 88.3% (95% CI 83.3% to 93.5%) and 85.5% (95% CI 77.1% to 94.8%; HR for 2-year mortality vs cluster 1: 1.3 (95% CI 0.57 to 2.8), p value: 0.567), respectively, while 2-year survival in patients from clusters 3 and 4 with irreversible right-sided cardiac damage ranged at 69.2% (95% CI 56.6% to 84.7%; HR for 2-year mortality vs cluster 1: 2.9 (95% CI 1.4 to 5.9), p value: 0.004) and 74.6% (95% CI 65.9% to 84.4%; HR for 2-year mortality vs cluster 1: 2.3 (95% CI 1.2 to 4.3), p value: 0.009), respectively (graphical abstract, figure 3).
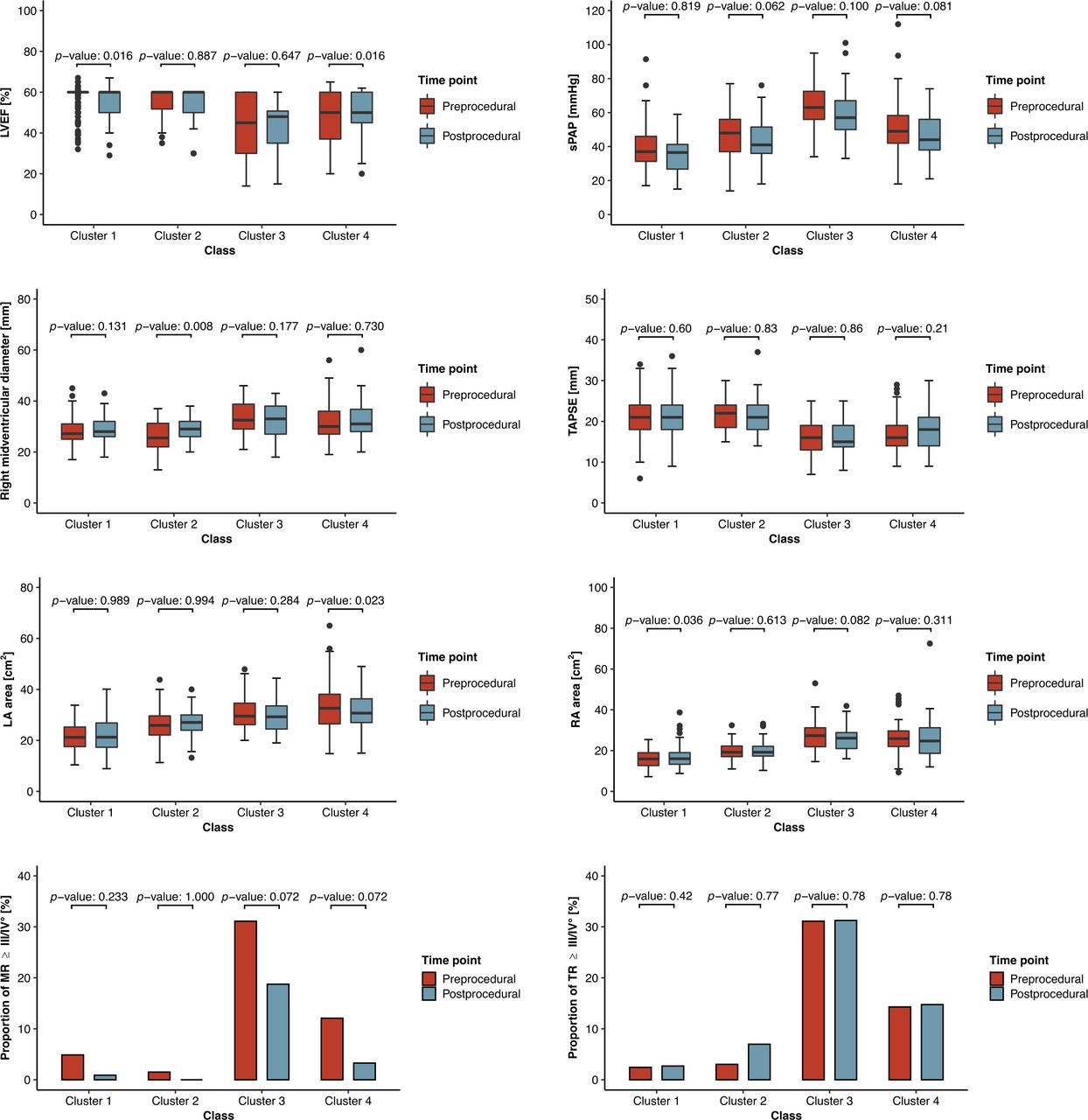
Comparison of echocardiographic parameters before and after TAVR in accordance with cluster assignment. LA area, left atrial area; LVEF, left ventricular ejection fraction; MR, mitral regurgitation; RA area, right atrial area; sPAP, systolic pulmonary artery pressure; TAPSE, tricuspid annular plane systolic excursion; TAVR, transcatheter aortic valve replacement; TR, tricuspid regurgitation.

Kaplan-Meier survival plot in accordance with cluster assignment. TAVR, transcatheter aortic valve replacement.
Comparison of echocardiographic follow-up data before and after TAVR
Comparison of echocardiographic follow-up data in accordance with cluster assignment
Comparative analysis: right heart dilatation and severe TR persist after TAVR as confirmed by a sequential staging classification of extra-aortic valve cardiac damage
Acknowledging that absence of evidence does not necessarily imply evidence of absence regarding right heart recovery after TAVR, patients were additionally stratified according to a staging classification of extra-aortic valve cardiac damage assuming a sequential progression of accumulated pathologies upstream of the causative severe AS (figure 4A). Only 4.64% of the 2928 data points required for allocating patients according to the sequential staging classification were initially missing and therefore had to be imputed (online supplemental figure 3). Interestingly, severity of dyspnoea expressed as NYHA classes worsened with rising stages of extra-aortic valve cardiac damage (online supplemental table 2). Moreover, the incidence of atrial fibrillation and/or flutter increased with rising stages (from 18.4% in stage 0 to 66.7% in stage 3). Almost all patients being allocated to stage 0 with no or little extra-aortic valve cardiac damage derived from cluster 1 (69 out of 76 patients (90.8%)) (figure 4B), and their 2-year survival after TAVR ranged at 87.2% (95% CI 79.8% to 95.4%) (figure 4C). Stage 1 comprised patients with functional and structural alterations restricted to the left heart, and their 2-year survival after TAVR ranged statistically indifferent to that from stage 0 at 86.1% (95% CI 77.1% to 96.2%). Interestingly, patients from cluster 2 with predominantly postcapillary PH were mainly allocated to stage 2 (50 out of 66 patients (75.8%)), and 2-year survival from patients in stage 2 was also statistically indifferent to that from stage 0 (82.7% (95% CI 75.7 to 90.3%)). Most patients (126 out of 366 patients (34.4%)) were allocated to stage 3 (figure 4B). Importantly, patients in stage 3 presented with impaired right ventricular function (TAPSE: 16.0±4.95 (95% CI 15.1 to 16.9) mm), right atrial enlargement (right atrial area: 24.6±8.73 (95% CI 23.0 to 26.2) cm2) and high prevalence of severe TR (26.2%) (online supplemental table 3), and their 2-year survival was lower than that from patients in stage 0 (76.4% (95% CI 69.1% to 84.5%); HR for 2-year mortality compared with stage 0: 2.0 (95% CI 0.96 to 4.3), p value: 0.062). Surprisingly, those patients were heterogeneously recruited from cluster 1 (25 patients (19.8%)), cluster 2 (11 patients (8.73%)), cluster 3 (31 patients (24.6%)) and cluster 4 (59 patients (46.8%)). Follow-up echocardiography revealed that both the prevalence of concurrent severe MR and sPAP levels were reduced following TAVR to varying degrees across all stages (figure 5). Moreover, a significant improvement in right ventricular systolic function expressed as TAPSE in patients allocated to stage 3 could be observed (figure 5, online supplemental table 4), but neither right atrial enlargement nor the high prevalence of severe TR from patients in stage 3 was reversed.

Comparative assessment of extra-aortic valve cardiac damage-associated survival in accordance with the modified staging classification from Généreux et al. (A) Sequential staging classification modified from Généreux et al2 based on the extent of extra-aortic valve cardiac damage. (B) Chord diagram to relate patient allocations from unsupervised clustering and from the modified sequential staging classification of extra-aortic valve cardiac damage in patients with severe AS. (C) Kaplan-Meier survival plot in accordance with the modified sequential staging classification. AS, aortic stenosis; LA area, left atrial area; LVEF, left ventricular ejection fraction; MR, mitral regurgitation; RA area, right atrial area; sPAP, systolic pulmonary artery pressure; TAPSE, tricuspid annular plane systolic excursion; TR, tricuspid regurgitation.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Comparison of echocardiographic parameters before and after TAVR in accordance with the modified staging classification from Généreux et al. LA area, left atrial area; LVEF, left ventricular ejection fraction; MR, mitral regurgitation; RA area, right atrial area; sPAP, systolic pulmonary artery pressure; TAPSE, tricuspid annular plane systolic excursion; TAVR, transcatheter aortic valve replacement; TR, tricuspid regurgitation.
Discussion
Our proposed artificial intelligence-based phenotyping approach identifies patients with severe AS and inevitably failing right hearts, hence refining prognostic assessment prior to TAVR
Refined prognostic assessment for patients with severe AS requires a comprehensive view that captures the complexity of both aortic and extra-aortic valve cardiac damage, because survival inevitably depends on the recovery of the cardiopulmonary system after TAVR. However, standard classification systems are either restricted to a hypothesis-driven selection of a few (dichotomised) parameters typically regarded in isolation or assume a sequential progression of accumulated pathologies upstream of the causative AS, potentially ignoring the aggravating impact of comorbidities or genetic predisposition. This is particularly problematic, because a plethora of contributors to right heart dysfunction, including coronary artery disease and subsequent myocardial ischaemia as well as COPD and secondary PH, will persist despite correction of severe AS and hence limit the expected benefit of TAVR. We have therefore previously proposed a machine learning framework consisting of an unsupervised clustering approach in conjunction with an ANN that facilitated to distinguish four clusters of prognostically informative phenotypes among patients with severe AS.3 This artificial intelligence-based phenotyping approach (graphical abstract) does neither hypothesise a linear sequence of accumulated pathologies (thus it incorporates the aggravating impact of comorbidities), nor does it stratify patients into low-risk and high-risk cohorts in accordance with a single variable’s dichotomy (thus it reduces the risk of oversimplification). We hereby provide cluster-related echocardiographic follow-up and updated survival data, revealing that the right heart function and structure does not recover after TAVR, and that patients preprocedurally assigned to clusters with persistent right heart dysfunction demonstrate a significantly increased mortality.
Does concurrent TR represent a clinical target for ancillary treatment beyond TAVR, or is PH as the linking pathology between left-sided and right-sided heart disease the true culprit driving mortality in patients from cluster 3?
Correction of AS by TAVR and anticipated improvement of left heart haemodynamics resulted in a significant reduction in the proportion of patients suffering from concurrent severe secondary MR (table 3). Interestingly, pulmonary artery pressures as estimated by echocardiography were also ameliorated, but the effect size expressed as levels of statistical significance varied among the clusters (figure 2). Patients assigned to cluster 3, who were characterised by the highest prevalence of COPD (24.4%), still presented with significantly elevated sPAP levels of 59.4±16.8 (95% CI 53.1 to 65.8) mmHg. Concomitant to the merely reduced pressure burden imposed from the pulmonary circulation to the right heart, severe TR was still diagnosed in 10 out of 32 patients (31.2%; compared with 31.1% before TAVR) from cluster 3 at follow-up, indicating that TAVR did not restore tricuspid valve integrity. It is well established that severe TR in patients undergoing TAVR is associated with poor prognosis9 11 12; however, it is difficult to determine whether TR itself causally drives mortality or whether it simply serves as a marker for PH and right ventricular decompensation.13 A recent study identified 3.4% of patients with TAVR as potential candidates for transcatheter tricuspid valve interventions (TTVIs),14 but larger prospective studies are mandatory to address the question where TR is a clinically meaningful target and where it represents an epiphenomenon.15 This differentiation is important because successful TTVI and concomitant reduction of regurgitant blood flow to the low-pressure right atrium acutely force the right ventricle to eject blood into the high-pressure pulmonary circulation. A remodelled pulmonary circulation in terms of elevated pulmonary vascular resistance levels in combination with impaired right ventricular systolic function unable to compensate for the abruptly increased afterload burden (both conditions met in patients from cluster 3) would threaten to accelerate cardiac deterioration following TTVI. Considering that long-standing PH and subsequent right ventricular dilatation ultimately result in exacerbation of TR through a combination of tricuspid annulus dilatation and papillary muscle displacement, Fortuni et al proposed to relate the TR vena contracta width to the tricuspid annulus diameter to define a TR proportionality concept for better patient selection.16 Fortuni et al hypothesised that in patients with disproportionate TR, the extent of valvular insufficiency is disproportionally larger than the degree of ventricular dilatation and is probably related to additional alterations of the valvular and subvalvular apparatus. Therefore, patients with disproportional TR would probably benefit from TTVI, whereas TTVI in cases of proportional TR would possibly expose patients to the risk of futile procedures.
sPAP levels at follow-up echocardiography were similar between clusters 2 and 4, but patients in cluster 4 were further coined by the unhappy triad of (1) atrial fibrillation and/or flutter, (2) right atrial enlargement and (3) severe TR, demonstrating that the right heart damage in patients with severe AS can be uncoupled from the pulmonary circulation
Current European Society of Cardiology guidelines suggest an evidence-based treatment algorithm for patients with pulmonary arterial hypertension, including drugs which elicit a favourable effect on haemodynamic parameters such as endothelin-1 receptor antagonists, prostanoids and phosphodiesterase type 5 inhibitors.17 Unfortunately, there is no evidence for a beneficial effect of pulmonary arterial hypertension-specific drugs for the management of patients with PH due to left heart disease. Indeed, the opposite may even be true: Bermejo et al demonstrated that treatment with phosphodiesterase type 5 inhibitor sildenafil for 6 months in patients with persistent PH after successful correction of left-sided valvular heart disease was associated with unfavourable clinical outcomes (death, hospital admission, worsening functional class, global symptom burden) as compared with placebo.18 Therefore, timely correction of the causative left-sided valvular heart disease appears as the only treatment option in these patients. Our follow-up data suggest that the timing of intervention in patients from cluster 2 was just in time, reflected by a significant reduction in PH levels and by a survival rate similar to that from reference cluster 1 (graphical abstract, figure 3). At the same time, sPAP levels as determined by follow-up echocardiography were similar between clusters 2 and 4 (44.1±14.4 (95% CI 39.2 to 49.0) mm Hg in cluster 2 vs 46.4±13.3 (95% CI 42.7 to 50.0) mm Hg in cluster 4), but survival differed significantly. This finding emphasises that structural alterations such as right ventricular and atrial dilatation with concomitant development of severe TR can occur in some patients without the driving force of severely elevated pulmonary artery pressures, hence challenging the validity of the hypothesised sequential progression of accumulated pathologies caused by severe AS in a real-world scenario. The significantly elevated prevalence of atrial fibrillation and/or flutter, ageing and possibly also genetic predisposition might have contributed to irreversible right atrial dilatation in patients from cluster 4, ultimately sustaining a vicious circle of arrhythmia, right atrial dilatation and worsening of TR.19
Where have all the patients gone who have previously been reported to show right heart recovery after TAVR?
It intuitively makes sense to cardiovascular practitioners that patients with recovering right heart function and structure after TAVR live longer than patients with persistent right heart dysfunction, and the compelling evidence that some patients do indeed improve in right heart function after TAVR cannot be ignored.7 8 20 Pairwise comparison of preprocedural and postprocedural echocardiography data yet demonstrated that there exists no general improvement of right heart diameters or function after TAVR (table 3). Depending on the classification method applied (unsupervised clustering or sequential staging), we have identified a subgroup of patients with ameliorating right heart dysfunction after TAVR, that is, patients allocated in stage 3 according to the sequential classification system. Even though those patients displayed an improved TAPSE during echocardiographic follow-up (but still ranging at a low level of 17.2±4.90 (95 CI 16.1 to 18.2) mm), other indices of right heart failure such as right ventricular dilatation and severe TR persisted, culminating in a distressing mortality rate. Possibly, a statistical phenomenon referred to as regression to the mean additionally accounted for that seeming improvement of TAPSE as observed in patients in stage 3, further emphasising the need for a refined classification system that preprocedurally stratifies patients into phenotypically and prognostically distinct patient groups.
The trained ANN embedded into a code to project a future patient into a multidimensional matrix could serve as a prototype of an online-based decision support tool
Importantly, the future of medicine is not about the competition of artificial intelligence against humans, but real-life medical practice will be coined by collaborative setups, where oversight-providing humans receive assistance from artificial intelligence.21 Since our ANN tested on an internal validation cohort demonstrated an excellent performance to detect patients from high-risk clusters 3 and 4 (100.0% and 85.2% sensitivity, as well as 95.9% and 95.1% specificity, respectively),3 we decided to export our trained ANN and to embed it into a code that allows future patient-to-cluster assignment (graphical abstract). Currently regarded as a prototype, our classification model based on unsupervised clustering in conjunction with an ANN could serve as an online-based decision support tool in the future. This would open the avenue for other cardiologists to stratify their patients according to our classification system, whenever echocardiographic and haemodynamic data obtained prior to TAVR are available. Moreover, our comprehensive approach sheds light on distinct pathophysiologies underlying high-risk clusters 3 and 4, which would not have become apparent, if both clusters were aggregated in one group coined by right ventricular (RV) dysfunction. It might be true that, for the moment, the prognosis between patients from high-risk clusters 3 and 4 is indifferent, but this may change with the emerge of TTVI as a promising therapeutic option for patients from cluster 4 with less severely elevated pulmonary artery pressures.
On the controversy of earlier interventions to prevent irreversible damage in patients with severe AS
Even though 2-year survival rates from patients in clusters 3 and 4 ranged at low levels (69.2% (95% CI 56.6% to 84.7%) and 74.6% (95% CI 65.9% to 84.4%), respectively), their survival was still better compared with conservatively managed patients featuring 2-year survival rates below 50%.22 Thus, it can be said that the beneficial effect of TAVR in patients from clusters 3 and 4 was limited compared with patients from clusters 1 and 2, but for sure it was not in vain. In the contemporary ‘one-size-fits-all’ practice of medicine, the timing of intervention mainly focuses on the aortic valve and on the occurrence of symptoms. This is because it was previously argued that intervention is not needed until symptoms supervene, because the risk of sudden cardiac death would be less than the risk of surgical aortic valve replacement. Considering the progress in safe transcatheter techniques on the one hand and the irreversibility of extra-aortic valve cardiac damage in patients from clusters 3 and 4 on the other hand, our findings emphasise the need for trials assessing the effect of even earlier intervention, possibly even before patients with severe AS become symptomatic. Two large ongoing trials (EARLY TAVR and EVoLVeD) comparing TAVR with surveillance in asymptomatic patients with severe AS will hopefully enlighten us, maybe also addressing the question ‘When is late too late to repair a damaged heart?’.
Limitations
We acknowledge as a limitation that follow-up echocardiography was available for only 67.5% of patients. We can only speculate on the reasons for missing follow-up echocardiography, such as the rural structure in Bavaria, Germany, where patients would need to travel long distances to reach the hospital for follow-up echocardiography, which is particularly problematic in elderly, immobile patients. Moreover, some patients might have died between TAVR and follow-up echocardiography, even though the general survival rate of 90.4% at 1 year after TAVR (figure 1D) indicates that this explanation is applicable only to a minority of patients. Most importantly, we have no selection bias in our data, as (1) equal proportions of patients were examined by follow-up echocardiography and (2) the time between TAVR and follow-up echocardiography was also equally long among clusters (figure 1B and online supplemental figure 2).
No systematic, cluster-related deterioration of right heart function was observed during follow-up, but an initially poor function was at least preserved in patients from this study. This stands in contrast to previous studies reporting a worsening right heart function in approximately 10% of patients after TAVR.6 7 However, patients from those studies underwent echocardiographic follow-up within 1 month after TAVR, while patients from this study underwent echocardiographic follow-up between day 30 and day 365 after TAVR. Our analysis therefore excluded patients, who deceased immediately after the procedure and hence never showed up for follow-up echocardiography, and it is very likely that those were high-risk patients with poorest (and potentially worsening) right heart function. To control for this selection bias, Kaplan-Meier survival estimates were calculated for all patients from the respective clusters, confirming the high mortality in clusters 3 and 4. In other words, excluding those patients from cluster-related survival analysis, who did not undergo echocardiographic follow-up (maybe because they have died in the meantime), would have fatally resulted in overestimation of survival after TAVR.
As a further limitation, right ventricular dysfunction was assessed by echocardiography alone, because it is widely available and easily reproducible. However, TAPSE as a parameter for right ventricular systolic function measures right ventricular motion only at the basal level, which is particularly problematic when pathological remodelling has already occurred.23 Three-dimensional or strain measurements as more sophisticated methods could have further refined echocardiographic right ventricular functional assessment.
Moreover, echocardiographic assessment of sPAP levels, as performed to compare pulmonary haemodynamics during follow-up, carries several pitfalls for underestimation in patients with severe TR.24 25 Prioritising data quality over data quantity for the initial unsupervised clustering experiment, we had therefore decided to rely on right heart catheterisation data as the gold standard to assess PH, even though current guidelines recommend to restrict right heart catheterisation to the minority of patients, where initial evaluation of AS severity is inconclusive.26 As a consequence, 85.8% of patients from the bicentric registry were initially excluded for the unsupervised clustering experiment, but the representative character of our patient subset was maintained.3 Such a seemingly harsh decision to exclude the majority of patients was necessary, because the partially unsupervised algorithms underlying our phenotyping approach needed reliable data, and because a flawed algorithm trained on flawed data such as underestimated sPAP levels could ultimately result in medical malpractice if ever implanted into clinical reality. In the future, we envision to replace invasive haemodynamics with artificial intelligence-enabled prediction of mPAP levels using echocardiographic parameters as input data as already demonstrated on patients with severe TR undergoing TTVI.25
Furthermore, this study was restricted to all-cause mortality, because an elderly patient population with multiple comorbidities approaching the end of life was analysed. Considering that severe cardiac dysfunction will also lead to impairment of other organs through reduced arterial perfusion and severe venous congestion, it is not surprising that renal function was reduced in patients from high-risk clusters 3 and 4 (table 1). Apart from being more vulnerable to any new insult such as infections as the leading cause of non-cardiac death among patients with TAVR,27 patients from high-risk clusters 3 and 4 with highest prevalence of atrial fibrillation and/or flutter could have also died from stroke or gastrointestinal bleeding, but we did not distinguish between causes of death.
Conclusions
Due to innovative algorithms and improved computing power, machine learning technology appears on the edge of evolving from theory to becoming a mainstream application in clinical practice. Converging human and artificial intelligence, this phenotyping approach succeeded to preprocedurally identify patients with severe AS, who will not recover from extra-aortic valve cardiac damage following TAVR and whose survival is therefore significantly reduced. Importantly, not so much the degree of PH at initial presentation, which can be ameliorated by TAVR, but the irreversibility of right heart dysfunction determines prognosis. Considering that a plethora of (unmodifiable?) comorbidities can contribute to right heart dysfunction, future studies are needed to shed light on potential targets to improve survival in patients assigned to high-risk clusters 3 and 4 with persistent right heart dysfunction.
Data availability statement
Data are available upon reasonable request. The data underlying this article will be shared on reasonable request to the corresponding author. All requests for raw and analysed data and related materials, excluding programming code, will be reviewed by the Ethics Committee at Technical University of Munich, Germany. Any data and materials that can be shared will be released via a Material Transfer Agreement.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by the Ethics Committee at Technical University of Munich, Germany (ID: 314/16 S). Participants gave informed consent to participate in the study before taking part.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors ML, KLL and CK are responsible for the overall content as guarantors, meaning that they accept full responsibility for the work and/or the conduct of the study, had access to the data, and controlled the decision to publish.
Conception and design or analysis and interpretation of data, or both: ML, ER, AH, EX, MvS, GH, MJ, CK. Drafting of the manuscript or revising it critically for important intellectual content: ML, TS, SY, KLL, MJ, CK. Final approval of the manuscript submitted: AS, CP, TT, TR, AK, HS.
Funding ML received funding from the Technical University of Munich (Clinician Scientist Grant) and from the Else Kröner-Fresenius Foundation (Clinician Scientist Grant).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.