Article Text

Abstract
Background Patients with severe atherosclerosis have been found to exhibit considerable changes in blood pressure (BP) between arms. The objective of our study was to investigate the predictive value of interarm blood pressure difference (IABPD) for coronary artery disease (CAD) severity.
Methods It was a cross-sectional study conducted in the Department of Cardiology, Chittagong Medical College Hospital, Chattogram from May 2020 to November 2020. The study conveniently selected 110 individuals who visited the department for a coronary angiography during the study period. The BP of both arms were synchronously measured 1–2 days before the coronary angiography and IABPD were calculated. After coronary angiography, two blinded interventional cardiologists visually estimated the amount of coronary artery obstruction and determined the Gensini score.
Results Among the participants, more than three-fourths of the patients were above 50 years of age (64.66%), and the majority were male (86.67%). 14.7% of participants had no occlusion in their coronary artery, 38.0% of participants had insignificant occlusion, 26.7% participants had mild occlusion, 10.3% participants had moderate occlusion, 3.3% participants had significant occlusion and 6.0% participants had total occlusion. Corrected pulse IABPD (cIABPDpulse) showed the greatest area under the receiver operating characteristic curve (0.73) for predicting a high Gensini score (>median). Multiple regression analysis revealed a significant relationship between corrected systolic IABPD (cIABPDsys) and the Gensini score (B=0.057, p<0.001).
Conclusion The differences in BP between the arms were found to be having a strong positive correlation with CAD severity.
- Coronary Artery Disease
- Coronary Angiography
- Hypertension
- Biostatistics
Data availability statement
All data relevant to the study are included in the article or uploaded as online supplemental information. The data that support the findings of this study are available from the corresponding author on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Significant inter-arm blood pressure (BP) difference is present in patients with advanced atherosclerosis.
WHAT THIS STUDY ADDS
Corrected inter-arm pulse pressure difference and corrected inter-arm systolic BP difference are better in predicting coronary artery disease severity.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Results from our study should help raise awareness among the physicians to practise simultaneous BP measurement in both arms, especially in the coronary artery disease patents.
INTRODUCTION
Osler initially defined the interarm blood pressure difference (IABPD) in 1915,1 since then this easily obtained noninvasive parameter is being practised all over the globe.2 3 In contrast to the right artery, the left subclavian artery forms an acute angle at its origin from the aorta, resulting in decreased blood flow. Consequently, right arm blood pressure (BP) is typically greater than left arm BP, leading in IABPD.4 As a clinical recommendation for hypertensive condition, an IABPD less than 10 mm Hg is regarded to be normal.5 In patients with advanced atherosclerosis, however, significant arm-to-arm changes in BP have been found.6
Ischaemic heart illnesses are among the leading causes of death on a global scale, although the relationship between IABPD and coronary artery disease (CAD) remains poorly understood.7 IABPD with systolic BP (SBP) more than 5 or 10 mm Hg was an independent factor of unfavourable cardiovascular outcome and all-cause mortality, according to a cohort analysis of people without a history of cardiovascular disease.8 Patients with a higher IABPD SBP seemed to have a greater rate of CAD and cerebrovascular disease, as well as a higher 10-year cardiovascular risk, according to a different prospective study (CoCoNet) involving 3699 participants.9 Sixty-three per cent of patients with IABPD of 15 mm Hg or higher had CAD involving at least one coronary artery, and 83% of those patients with CAD had multivessel CAD, according to a study that examined the association between IABPD and CAD in 283 patients who had coronary angiography.10 However, seven further investigations found no significant relationship between pre-existing CAD and IABPD, while other prospective studies found that an IABPD of 10 mm Hg or above increased the development of CAD (despite the fact that these investigations were restricted by the use of non-invasive methods of diagnosis).9 11 12
The purpose of this study was to evaluate the link between IABPD and CAD severity in order to establish IABPD as a predictor of CAD severity. Findings from our research can help establish the role of IABPD as a tool for assessing atherosclerotic severity of CAD and thus help prevent the progression of atherosclerosis by aggressive risk factor interventions and reduce cardiovascular mortality.
Materials and methods
Study design and study participants
This cross-sectional investigation was carried out between May 2020 to November 2020 at the Department of Cardiology, Chittagong Medical College Hospital. All the patients (213) visiting the department for coronary angiography during the study period were conveniently approached for enrollment in the study. Since this study was conducted during the COVID-19 pandemic, patients attending the department were lower compared with the prepandemic period. Sixty-six patients did not consent to enter the study, and 37 patients with a history of revascularisation, congenital heart disease, significant valvular heart disease, peripheral artery disease, atrial fibrillation, cardiomyopathy and aortic coarctation were excluded from the study (figure 1).

Strengthening the Reporting of Observational Studies in Epidemiology flow chart of study participants. A total of 213 individuals were approached for enrolment. Ninety-three individuals were eliminated because they did not match the inclusion requirements, leaving 110 as the final sample size.
Operational definitions
Patients were diagnosed with hypertension if they had a ‘persistent rise in SBP ≥140 mm Hg and/or diastolic BP (DBP) ≥90 mm Hg for at least two occasions, or if they were using antihypertensive medication or had a history of hypertension’.13 Patients were diagnosed with diabetes if they had a ‘history of diabetes or used antidiabetic medications, or if their fasting plasma glucose was ≥126 mg/dL or 2 hours after fasting plasma glucose was ≥200 mg/dL, or if their glycated hemoglobin (HbA1c) was ≥6.5%, or if they exhibited classic symptoms of hyperglycaemic or hyperglycaemic crisis, and their random plasma glucose was ≥200 mg/dL (≥11.1 mmol/L)’.14 Dyslipidaemia was diagnosed if the patient had ‘total cholesterol above 200 mg/dL, low-density lipoprotein (LDL) cholesterol above 130 mg/dL, high-density lipoprotein (HDL) cholesterol below 40 mg/dL (>1.0 mmol/L) in males and 50 mg/dL (>1.3 mmol/L) in women, triglycerides above 150 mg/dL (>1.7 mmol/L), or was taking lipid-lowering therapy’.15 Unstable angina is chest discomfort or pain resulting from inadequate blood and oxygen supply to the heart.16 Non-ST-elevation myocardial infarction (NSTEMI) is diagnosed in patients with acute coronary syndrome-like symptoms and elevated troponin levels, but no STEMI-like ECG abnormalities.16 STEMI is clinically diagnosed when there is new (or increased) and sustained ST-segment elevation in at least two contiguous leads of >1 mm in all leads, excluding leads V2–V3 for which the following cut-off points apply.17 Current smoker, smoking cigarettes within 1 month of this admission; recent smoker, quit between 1 month and 1 year before this admission; past smoker, quit greater than 1 year before this admission; non-smoker, never smoked cigarettes.18
Measurement of arm BP and IABPD
BP were measured 1–2 days prior to coronary angiography. Patients rested for at least 5 min prior to having their BP taken with an aneroid sphygmomanometer (ALPK2 500 V, Japan) in both arms simultaneously, which was valid and properly calibrated. The bladder cuff was an appropriate size and can encompass more than two-thirds of the arm. Before the procedure, tight clothes were removed, and the arm was sustained at the heart level. Two measurements were recorded at 2 min intervals. Mean pressure was calculated as, one-third times SBP added with two-thirds times DBP and pulse pressure was calculated as the difference between SBP and DBP. In order to account for the significance of baseline BP, the IABPD was measured as the change in BP between the two arms and corrected (cIABPD) by calculating the proportion arm with the higher BP.
Assessment of CAD severity
With the aid of coronary angiography data, two interventional cardiologists visually estimated the extent of coronary artery obstruction in each patient. The interventional cardiologists were approached conveniently from the same department. After informing about the aims and objectives of the study, they voluntarily contributed to the study. The profiles of the patients were concealed from the cardiologists. Using the data, they subsequently evaluated the Gensini score. The Gensini score was devised in 1975 to quantify the severity of CAD by considering the geometrical severity of a lesion as assessed by angiography, the cumulative effect of several blockages, and the significance of the myocardium at risk.19 Each lesion was assigned a value based on the proportion of stenosis: 25% stenosis was ranked 1, 50% stenosis was ranked 2, 75% stenosis was tanked 4, 90% stenosis was ranked 8, 99.9% stenosis was ranked 16 and 32 was assigned for total occlusion. This score was then multiplied by a value based on the site of the affected section (ie, the lowest value 0.5 was assigned left circumflex arterial artery, posterolateral branch and second diagonal artery, 1 was assigned for right coronary artery, obtuse marginal branches as well as first diagonal branch, 1.5 assigned for middle left descending artery, 2.5 for left circumflex artery and proximal left anterior descending branch, the highest point 5 was assigned for left main coronary artery). The Gensini score is then determined by adding the scores for coronary stenosis degree and lesion site.
Statistical analysis
For data analysis, we used Stata (V.16; StataCorp). Using a histogram, a normal Q-Q plot and the Kolmogorov-Smirnov test, the normality of continuous data was determined. Due to the positively skewed distribution of the Gensini score, the original score was transformed as ln (original Gensini score +1) in order to be included in the study. As a measure of the centre of quantitative data, the arithmetic mean was used, while the SD was used as a measure of dispersion. We summarised qualitative data using frequency and relative frequency. Student’s t-test was performed to determine the significance of the difference between the two arms’ mean BP values. Pearson’s correlation analysis was used to analyse the association between the Gensini score and IABPD parameters. We also computed receiver operating characteristic (ROC) curves to predict a high Gensini score, and then used the DeLong method to determine differences between ROC curves for various IABPD. Simple and multiple linear regression model was fit using the Gensini score as the outcome variable to investigate the role of IABPD parameters and other associated factors. A two-tailed p<0.05 was regarded as statistically significant. Our dataset did not have any missing data. All reporting conformed to the Strengthening the Reporting of Observational Studies in Epidemiology standards.20
Results
Most respondents were males (94%), aged between 51 and 60 years (36.36%), living predominately in the urban areas (60.91%). Almost all of the respondents demonstrated a right-hand dominance (95.45%). The majority of responders had no history of CAD (69.09%). The majority of the responders were currently smoking (34.55%) or had a history of smoking (29.09%). Most of the respondents did not have a history of diagnosed comorbidities including diabetes mellitus (76.36%), hypertension (57.27%) and dyslipidaemia (70%). The respondents’ diagnosis during the study revealed that the majority had unstable angina 52.72%, with NSTEMI being the second common (28.18%). An abnormality of fasting blood glucose was found to be in most of the respondents, with impaired glucose (30.00%) and diabetes (24.55%). The distribution of lipid profiles of the respondents revealed majority portion of the respondents had a normal level of cholesterol (72.73%), LDL (69.09%), HDL (91.00%) and triglyceride (57.27%). Most of the respondents had some level of CAD, with a majority having an insignificant block (40.00%). More than half the patients had elevated SBP in the right arm (50.91%) and SBP in the left arm was normal in most of the patients (51.82%). DBP was mostly normal in both hands (56.36%) (table 1).
Background information on study participants (n=110)
Moreover, a statistically significant difference was discovered between the right and left hand in diastolic (p=0.04) and pulse pressures (0.01) (figure 2).

Blood pressure measurements of study participants. Significant difference between the both arms (p<0.05) is highlighted with an asterisk (*).
Between normotensive and hypertensive participants, the correlation between IABPD measures and Gensini score was studied (table 2).
Correlation of Gensini score and IABPD parameters
All the IABPD parameters positively correlated with the Gensini score(figure 3); all of them were found to be highly statistically significant in case of normotensive patients (p<0.05). However, in case of hypertensive patients cIABPDsys (p<0.01), cIABPDpulse(p<0.011), IABPDsys(p<0.013) and IABPDmean (p<0.008) constituted statistical significance.
{kind=link}
{kind=link}
{kind=link}
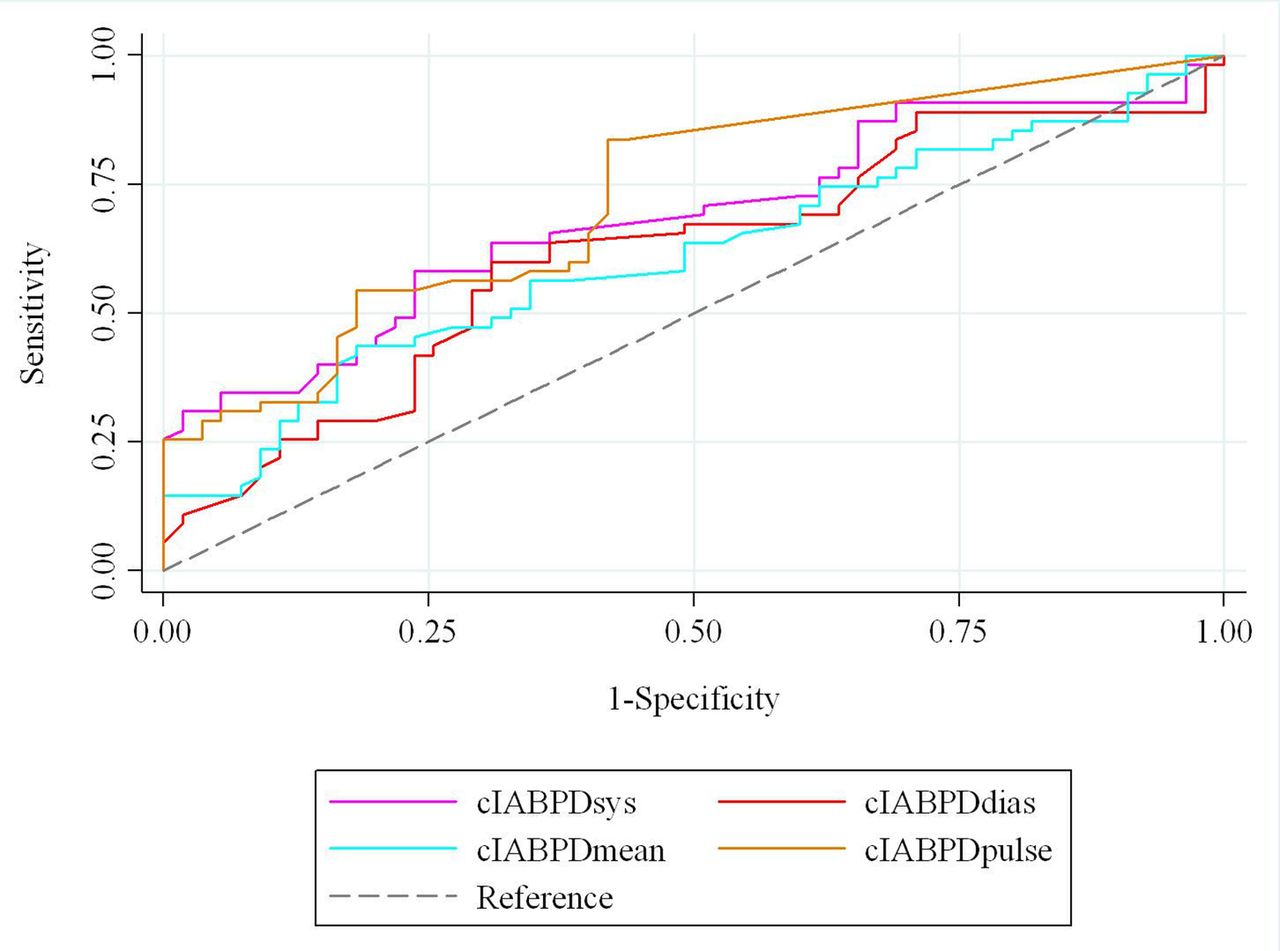
Comparison of receiver operating characteristic (ROC) curve for cIABPDsys: cIABPDdia, cIABPDmean and cIABPDpulse to predict high (>median (25.25)) Gensini Score. Area under the ROC curves for cIABPDsys: 0.69, cIABPDdia:0.62, cIABPDmean: 0.61, and cIABPDpulse: 0.73. cIABPDpulse, corrected pulse interarm blood pressure difference.
To investigate the factors related with Gensini score, a linear regression model was used (table 3). The univariate model revealed significant association between gender (p<0.01), diabetes mellitus (p<0.004), hypertension(p<0.001), dyslipidaemia (p<0.007), cIABPDsys(p<0.001), cIABPDmean (p<0.07) and cIABPDpulse(p<0.001). The model showed that males tend to score 3.2% higher than females, hypertensive 31.5% than normotensive, diabetic 4.9% than non-diabetic, dyslipidaemic 17.2% than normal lipid level, higher cIABPDsys 95% than lower, higher cIABPDmean 96% than lower and higher cIABPDpulse 94% than lower. However, in a multivariate model only hypertension (p<0.001) and cIABPDsys(p<0.001) retained their significance. The model demonstrated that hypertensive respondents had 12.2% chance higher than normotensive and increased cIABPDdia had 94.3% higher chance of having higher value in Gensini score.
Univariate and multivariate analysis of factors associated with the Gensini score
Discussion
This was one of the first studies, to the best of the researchers’ knowledge, to attempt to explore the relationship between the risk of developing CAD and the Gensini score in the setting of Bangladesh. While the prevalence of CAD has increased significantly among the Bangladeshi population in recent years, few studies have been undertaken to create or apply a system for disease identification earlier.21
The difference between arms’ BP is one such critical diagnostic and prognostic factor. Our study discovered a significant difference in diastolic and pulse pressures between the two arms. Among the participants in our study, 57 (51.82%) participants had normal IABPD and 53 (48.18%) participants had raised (>10 mm Hg) IABPD. Extensive research has been undertaken to gain a better understanding of the clinical importance of interarm BP, both systolic and diastolic, with the difference generally being greater in the right than in the left.22 This was mostly owing to the acute angle formed by the left subclavian artery, which reduced blood flow and, consequently, BP, in comparison to the right.23 Consistently, research has revealed that an increase in IAD difference is associated with an increase in cardiovascular morbidity and mortality,8 24 25 as well as a possible prognostic factor.22 A greater difference of 5–10 mm Hg was particularly consistent with a greater risk for the patients.8
Further analysis of the relationship between the Gensini Score and IABPD parameters between the normotensive and hypertensive respondents revealed a significant correlation of all IABPD parameters among the normotensive patients. However, cIABPDsys, cIABPDpulse, IABPDsys and IABPDmean was found to be significant for both groups. These results align with those of a previous study done by Park et al, who recognised cIABPDsys had significant correlation with severity of coronary diseases.25 This correlation can help physicians identify and manage the vulnerable risk groups.
Lastly, a regression analysis was conducted to determine the impact of various variables on the Gensini score. The univariate model predicted that those of female gender, hypertensive, diabetic, dyslipidaemic, had higher values of cIABPDmean and cIABPDpulse were in higher risk compared with their counterparts. This correlation can be explained by the fact that the Gensini score was developed to measure the risk of CAD based on arterial stenosis.19 The factors mentioned above are usually associated with increased incidence of vascular insults in various mechanisms and increases the risk of CADs. For example, whereas CAD has historically been regarded as a male-prevalent disease, accumulating data indicates that women, particularly after menopause, are at an increased risk of getting CAD.26 Hypertension is one of the strongest risk factors that may be modified for CAD, being the strongest predictor in childhood and adolescence. Hypertension harms the blood vessels in a variety of ways, including acting as a physical force for the development of atherosclerosis, which may lead directly to the development of late-onset obstruction, hence raising the risk of CAD.27 Diabetes mellitus is significantly related to CAD, with a twofold to fourfold increase in risk compared with non-diabetic controls. Through metabolic disorders such as hyperglycaemic and dyslipidaemia, DM may directly harm endothelial cells and smooth muscles.28 On the other hand, dyslipidaemia has long been recognised as a primary and independent risk factor for CAD, even as a necessary condition for developing CAD. It has been established that dyslipidaemia is the initial risk factor contributing to the onset of CAD before other risk factors take action.29 As each component independently or in combination increases the likelihood of having CAD, they are associated with a higher Gensini Score.
However, in a multivariate model, only hypertension (p<0.001) and cIABPDsys (p<0.001) exhibited statistically significant results. According to the model, hypertensive respondents had 12.2% higher chance than normotensive and increased cIABPDdia had 94.3% higher chance of having a higher value in the Gensini score. Park et al also found Hypertension to be a significant predictor of Gensini score.25 The variation in the results might be attributed to the variation in sample size.
The precise mechanism of IABPD is unknown, however, the link between IABPD and CAD suggests that atypical alterations like luminal constriction (atherosclerosis) and vascular rigidity (arteriosclerosis) are related.9 30
The study has some limitations. BP were only tested once, however, data showing repeated BP measures lower the variance in IABPD by 30%31 and boost repeatability.32
Since this was a cross-sectional study, we couldn’t establish causality for the associations that we presented in this study. We performed multiple linear regression to adjust for the possible confounders. In future prospective investigations, the measurement of central BP via cardiac catheterisation, which is more clinically relevant to cardiovascular illness, may be required to validate our findings. Nonetheless, according to a number of studies, numerous measures were not always reproducible, and a single reading is sufficient for IABPD screening. Standard simultaneous and automated measurement of BP in both arms mitigates the potential impacts of BP variations, cuff-response bias (white coat effect), observer bias, and digit preference. Consequently, despite various limitations, our findings continue to support the notion that IABPD may be a useful therapeutic measure. Additionally, the study sample should be diversified and increased in future studies to ensure that the conclusions are generalisable.
Conclusion
IABPD was found to correlate significantly with the severity of CAD in our study. However, the guideline of measuring both arms during the initial assessment of high BP is not commonly practised by the general practitioners.33 Therefore, results from our study should help raise awareness among the physicians to practise simultaneous BP measurement in both arms, especially in the CAD patients. Future studies with a more diverse population can aid in the development of methods for the clinical implementation of these findings.
Data availability statement
All data relevant to the study are included in the article or uploaded as online supplemental information. The data that support the findings of this study are available from the corresponding author on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by the Institutional Review Board (IRB) of Chittagong Medical College (Approval number: CMC/PG/2019/611). Participants gave informed consent to participate in the study before taking part.
Acknowledgments
We gratefully acknowledge all the patients and the interventional cardiologists who participated in this study.
References
Footnotes
Contributors SD, MAI, JD, FC and SR contributed to conception and design. SD, MAI and FC drafted the manuscript. SD and JD contributed to data acquisition. MAI contributed to analysis, and MAI and FC contributed to interpretation and critically revising the manuscript. All authors gave final approval and agreed to be accountable for all aspects of work ensuring integrity and accuracy. SD accepts as guarantor full responsibility for the finished work, had access to the data, and controlled the decision to publish.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.