Article Text

Abstract
Background The burden of valvular heart disease (VHD) has increased significantly among ageing populations, yet remains poorly understood in the present-day context of percutaneous and surgical interventions.
Objective To define the incidence, clinical correlates and associated mortality of VHD in the UK Biobank cohort.
Methods We interrogated data collected in the UK Biobank between 1 January 2000 and 30 June 2020. VHD incidence was determined using International Classification of Disease-10 codes for aortic stenosis (AS), aortic regurgitation (AR), mitral stenosis, mitral regurgitation (MR) and mitral valve prolapse. We calculated HRs for incident VHD and all-cause mortality. Clinical correlates of VHD included demographics, coronary artery disease, heart failure and atrial fibrillation. Surgical and percutaneous interventions for mitral and aortic VHD were considered time-dependent variables.
Results Among 486 187 participants, the incidence of any VHD was 16 per 10 000 person-years, with highest rates for MR (8.2), AS (7.2) and AR (5.0). Age, heart failure, coronary artery disease and atrial fibrillation were significantly associated with all types of VHD. In our adjusted model, aortic and mitral VHD had an increased risk of all-cause death compared with no VHD (HR 1.62, 95% CI 1.44 to 1.82, p<0.001 and HR 1.25, 95% CI 1.09 to 1.44, p=0.002 for aortic and mitral VHD, respectively).
Conclusion VHD continues to constitute a significant public health burden, with MR and AS being the most common. Age and cardiac comorbidities remain strong risk factors for VHD. In the modern era of percutaneous and surgical interventions, mortality associated with VHD remains high.
- epidemiology
- aortic valve insufficiency
- aortic valve stenosis
- mitral valve insufficiency
- tricuspid valve insufficiency
Data availability statement
Data may be obtained from a third party and are not publicly available. Data can be obtained by researchers through approved projects (ukbiobank.ac.uk/register-apply).
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- epidemiology
- aortic valve insufficiency
- aortic valve stenosis
- mitral valve insufficiency
- tricuspid valve insufficiency
WHAT IS ALREADY KNOWN ON THIS TOPIC
Valvular heart disease prevalence is rising in Europe and the USA with ageing populations. In the past decade, several percutaneous interventions have been approved for use in high-risk patients, and surgical techniques have dramatically improved.
WHAT THIS STUDY ADDS
The most common types of incident valve disease in this large, contemporary cohort from the UK are mitral regurgitation (8.2 per 10 000), aortic stenosis (7.2 per 10 000) and aortic regurgitation (5.0 per 10 000). Risk is increased by age and the presence of cardiac conditions. Despite the existence of surgical and percutaneous interventions for severe disease, mortality in patients with valve disease remains high.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Examination of real-world clinical practice patterns and guideline adherence for valvular interventions are warranted to investigate the causes of excess mortality among patients with valve disease.
Introduction
With the declining burden of rheumatic heart disease in non-endemic countries, valvular heart disease (VHD) has increasingly become a disease of ageing.1 2 Multiple cohort-based studies show the sharp rise of incident VHD with age, particularly for mitral regurgitation (MR) and aortic stenosis (AS). The shift in VHD epidemiology from rheumatic disease in younger patients to degenerative valve disease in older adults with comorbidities has translated into widespread use of percutaneous interventions.3 At the same time, improvement in postsurgical care has led to reduction of morbidity for surgical valve replacement4 and repair.5
Prior studies have investigated the overall prevalence, clinical determinants, and outcomes of VHD in both USA and European cohorts.1 2 6–8 Such investigations, some dating to the late 1990s and early 2000s, have highlighted the presence of modifiable risk factors such as hypertension and obesity,7 9 for the development and progression of VHD. These studies have also underlined the high mortality associated with VHD.1 8 However, they have not taken into account the more contemporary influence of percutaneous procedures and improved surgical techniques on VHD burden and outcomes.
By leveraging the UK Biobank, a large, contemporary prospective population-based study, we aimed to investigate (1) the incidence and clinical correlates of VHD taking into consideration current burden of known cardiovascular risk factors for VHD and (2) the all-cause and cardiovascular mortality associated with VHD in the modern era of percutaneous and surgical interventions.
Methods
Data sources
The UK Biobank is a large biomedical cohort of adults age 40–69 who were recruited between 2006 and 2010 across 22 assessment centres in the UK, with follow-up assessment until 2020. Participant data include baseline interview of self-reported conditions, physical measurements and linkage to International Classification of Disease-10 (ICD-10) codes used by National Health Services for primary care visits, hospital admissions and death records.10 The UK Biobank includes a ‘first occurrence’ field for new diagnoses that appear in these data sources. Participant-level data provided to researchers are anonymised to protect identity. The study protocol was approved by the UK Biobank (Project 26751).
Patient and public involvement
The UK Biobank disseminates research generated from the database, including this study, for participants and the general public to view through their website and twitter feed (https://www.ukbiobank.ac.uk/). Given that the UK Biobank is a deidentified database, participants were not contacted or involved in the design and conduct of this retrospective study.
Study cohort
VHD was defined using ICD-10 codes and self-report codes for MR, mitral stenosis (MS), mitral valve prolapse (MVP), tricuspid regurgitation (TR), aortic regurgitation (AR) and AS (online supplemental table 1). Prior validation analyses using ICD-10 codes have found a high positive predictive value for all VHDs studied, with moderate or severe disease severity in the majority of cases, particularly for AS.11 Due to the rare occurrence of congenital pulmonic valve disease and tricuspid stenosis among adults, these valvular conditions were not included in our investigation, which was based on an adult cohort.
Supplemental material
MVP was defined by specific ICD-10 codes (online supplemental table 1). For the purpose of our study, we placed participants with codes for both MVP and MR in the general MR category.
Clinical correlates
We chose cardiovascular covariates that are considered contributors or comorbid conditions to VHD. Systolic blood pressure (SBP) and body mass index (BMI) were measured at participant enrolment. Obesity was defined as BMI>30 kg/m2. ICD-10 codes (online supplemental table 2) were used to identify the presence of smoking disorder, dyslipidaemia, diabetes, coronary artery disease (CAD), congestive heart failure (CHF), rheumatic fever, atrial fibrillation/flutter (AF), infective endocarditis and pulmonary hypertension.
Valvular interventions
The Office of Population Census and Surveys version 4 procedural coding system was used to identify mitral and aortic valve surgery (repair and replacement), and percutaneous interventions including annuloplasties and repairs. Mitral valve interventions included diagnostic codes for MR or MS with a corresponding procedural K code. Percutaneous interventions also included a Y code defining the approach.12 Aortic valve interventions included a procedural K code, with transcutaneous aortic valve replacement (TAVR) defined using addition of Y code. Tricuspid valve interventions were defined in a similar fashion (online supplemental table 3).
Outcomes
Incident VHD was defined as ‘first occurrence’ VHD between January 2000 and June 2020, after excluding prevalent cases diagnosed in December 1999 or earlier. Mortality outcomes included all-cause mortality and cardiovascular mortality due to myocardial infarction, stroke, cardiac arrest or CHF (see online supplemental table 4).
Statistical analysis
Continuous variables were expressed as median and interquartile ranges or mean and SDs if normally distributed. Categorical data were expressed as number and percentage of total subjects in each group. Incident rates were calculated per 10 000 person years. The assessment period of participants with and without VHD ended at the date of death or June 2020.We used Cox proportional hazard cause-specific models to calculate HRs and 95% CIs. Demographics (age, male sex), risk factors (SBP, obesity, smoking, dyslipidaemia, diabetes, CAD, CHF and AF) and valve interventions were treated as time-dependent covariates when calculating HR for incident VHD. We calculated HR for any VHD as well as valve disease subtypes: TR, MR, MS, AR, AS. As MVP is considered a genetic condition,13 and its development unrelated to typical cardiovascular risk factors, we did not run multivariate Cox models for this valvulopathy.
Next, we assessed any VHD, mitral valve disease (inclusive of MR, MS and MVP) and aortic valve disease (inclusive of AR and AS) as predictors of all-cause and cardiovascular mortality using Cox proportional hazards models. These models were adjusted for age, sex, SBP, obesity, smoking, dyslipidaemia, diabetes, CAD and CHF as well as valvular interventions. We included only those interventions that were relevant to the affected valve (eg, for our aortic valve model we only included aortic valve interventions). Assessments of Kaplan-Meier versus predicted survival plots and log-minus-log survival plots demonstrated that proportional hazards assumptions were met for each outcome.
Statistical analysis was performed using Stata V.14 (StataCorp) and SAS V.9.4 (SAS Institute). All reported p values are two sided, and statistical significance is reported for α=0.05.
Results
Population characteristics
A total of 486 187 subjects were included in the analysis. There were 13 615 cases of new VHD, including 6900 with MR, 6020 with AS, 4238 with AR, 2095 with MS, 1664 with TR and 1119 with MVP. Incidence rate per 10 000 person-years was 16.3 (95% CI 16.0 to 16.5) for all VHD, with the highest for MR at 8.2 (95% CI 8.0 to 8.4), followed by AS at 7.2 (95% CI 7.0 to 7.3) and AR at 5.0 (95% CI 4.9 to 5.2) (table 1). Demographic characteristics and comorbidities are summarised in table 2. Compared with those without VHD, those with any VHD tended to be older and were more commonly men (56% vs 45%). Rheumatic fever was rare, but a significant contributor to MS (present in 44% of cases) and MR (present in 12% of cases). Male sex was slightly more prevalent (66% males) among those with MVP (table 2). AF was common in all valve disease subtypes, but rare in the non-valvular population. There were 78 mitral valve (8 percutaneous), 238 aortic valve (36 percutaneous) and 25 tricuspid valve (5 percutaneous) interventions. Demographic characteristics and comorbidities of patients with VHD who did and did not receive interventions are summarised in online supplemental table 5. Patients with VHD treated with surgical or percutaneous interventions were predominantly male, and more likely to have CAD or AF. Patients who did not undergo valvular procedures had more CHF.
Valvular heart disease incidence rate and age of diagnosis
Demographics and comorbidities of incident valve disease
Comorbidity profiles of incident VHD
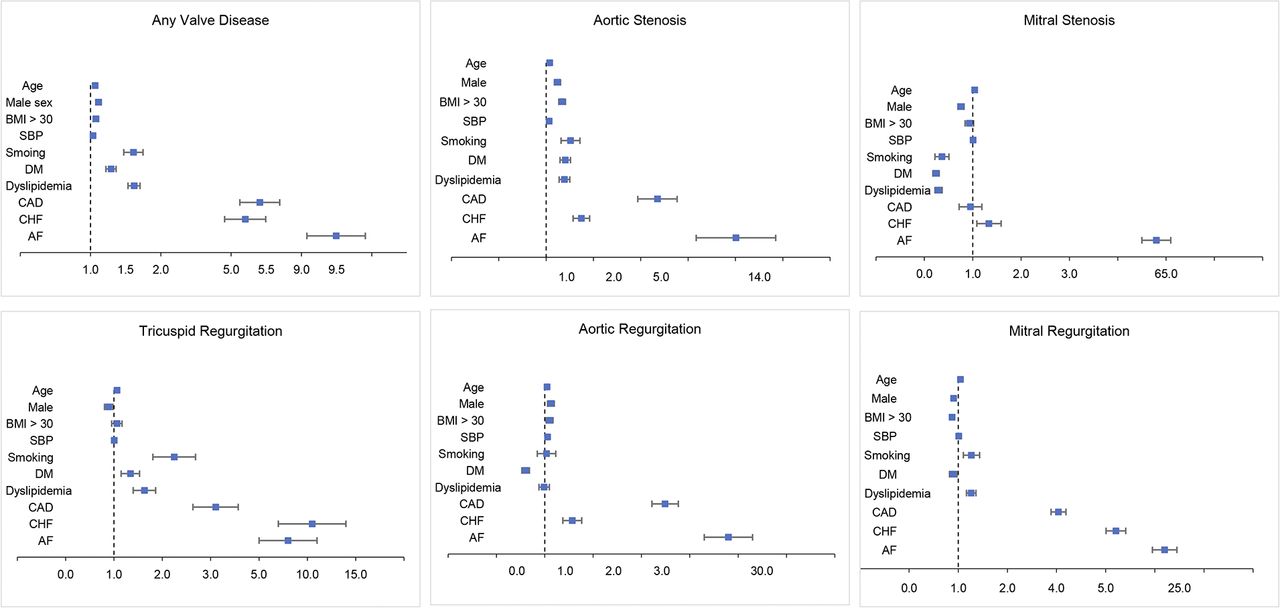
Fully adjusted Cox proportional hazard models of incident valve disease are shown in figure 1. All covariates studied were significantly associated with increased risk of incident VHD. Age significantly increased risk of all incident VHD types. Male sex was associated with incident AS, and AR, but not MS, MR or TR.
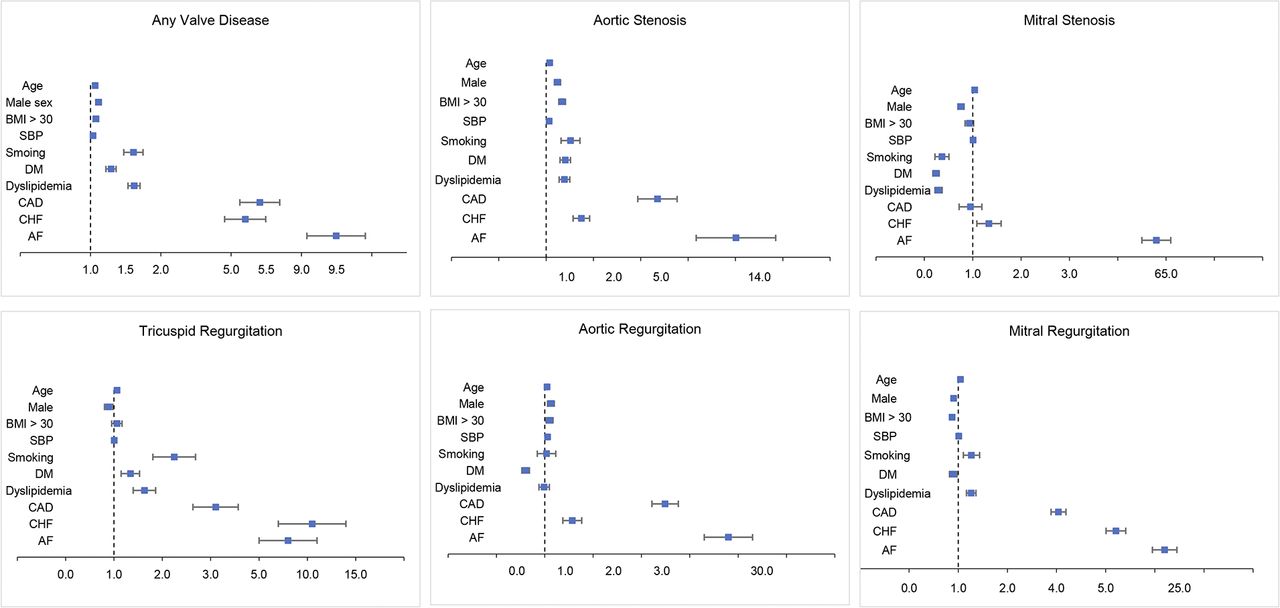
Clinical correlates of incident valvular heart disease (VHD). Forest plots of multivariate Cox regression of incident VHD, VHD subtypes and clinical correlates. AF, atrial fibrillation; BMI, body mass index; CAD, coronary artery disease; CHF, congestive heart failure; DM, diabetes mellitus; SBP, systolic blood pressure.
The greatest HRs for development of any VHD were the following cardiac conditions: AF (HR 9.45, 95% CI 9.08 to 9.93), CAD (HR 5.41, 95% CI 5.12 to 5.71) and CHF (HR 5.2, 95% CI 4.91 to 5.51). Strong positive associations for AF and CHF were observed across all VHD subgroups (figure 1). CAD was associated with increased hazard for all VHD subtypes except MS. Obesity, SBP, smoking, diabetes and dyslipidaemia were associated with increased risk of AS. Obesity and SBP were associated with increased risk of AR but smoking, diabetes and dyslipidaemia were not. Smoking and dyslipidaemia were associated with increased risk of MR but obesity, SBP and diabetes were not. None of these comorbidities (obesity, SBP, smoking, diabetes, dyslipidaemia) were associated with risk of incident MS.
Mortality and VHD
During 8 465 586 person-years of follow-up, there were 598 deaths among patients with incident valve disease, including 312 with aortic valve disease (0.37 deaths per 10 000 person-years), 213 with mitral valve disease (0.25 deaths per 10 000 person-years) and 43 with tricuspid valve disease (0.51 deaths per 10 000 person-years). Of the total deaths, 193 (79 with aortic valve disease and 83 with mitral valve disease) were from cardiovascular causes, all driven by cardiac arrest.
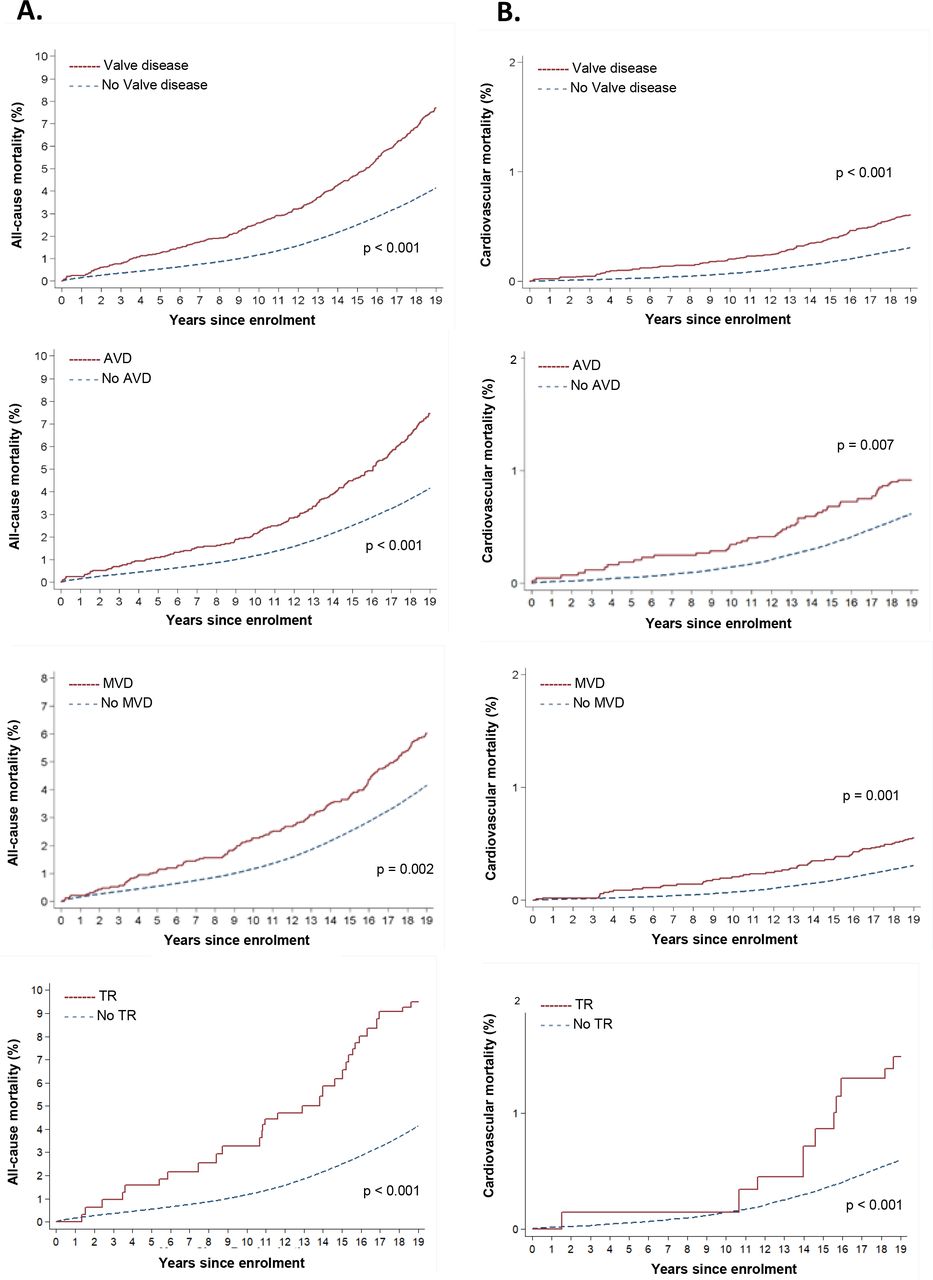
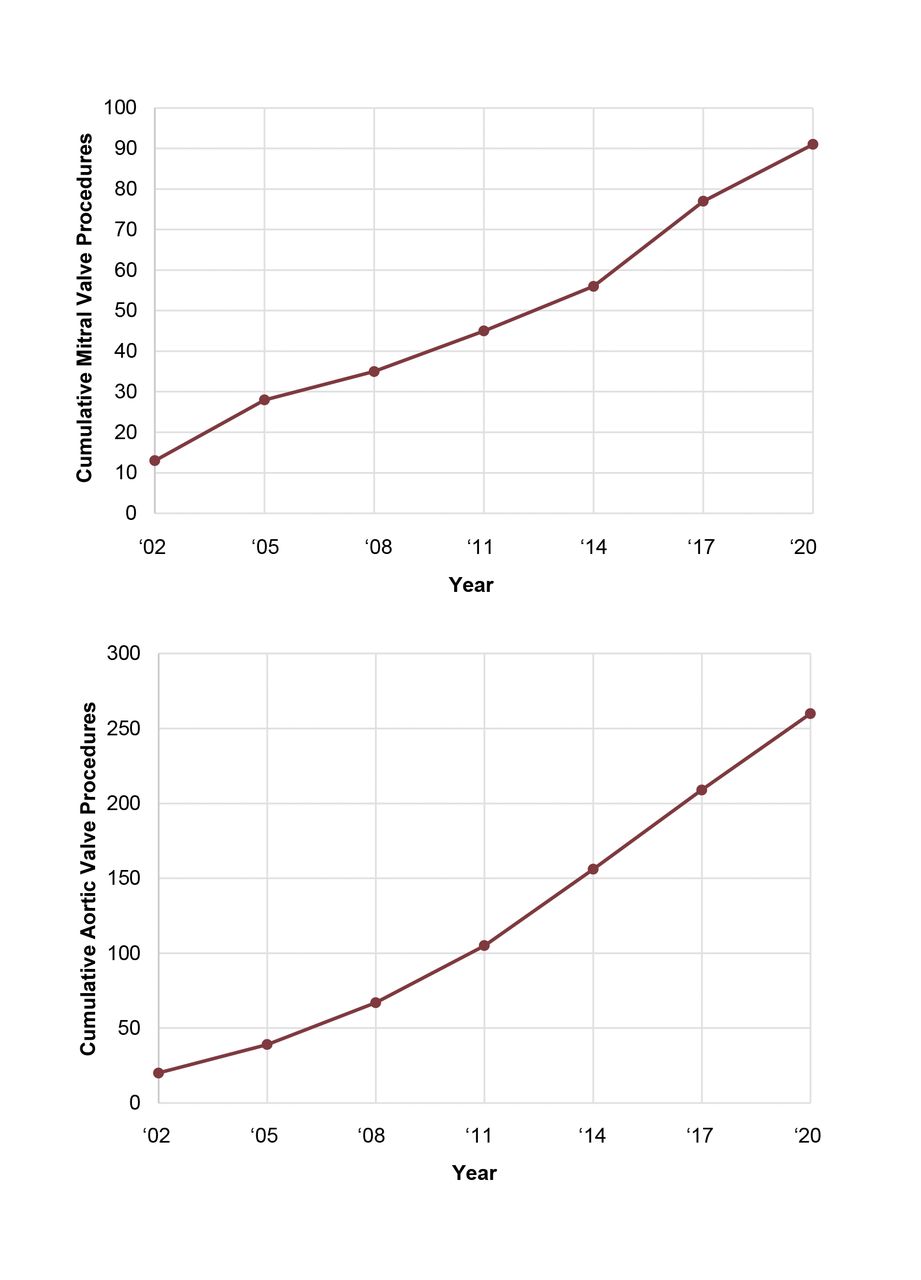
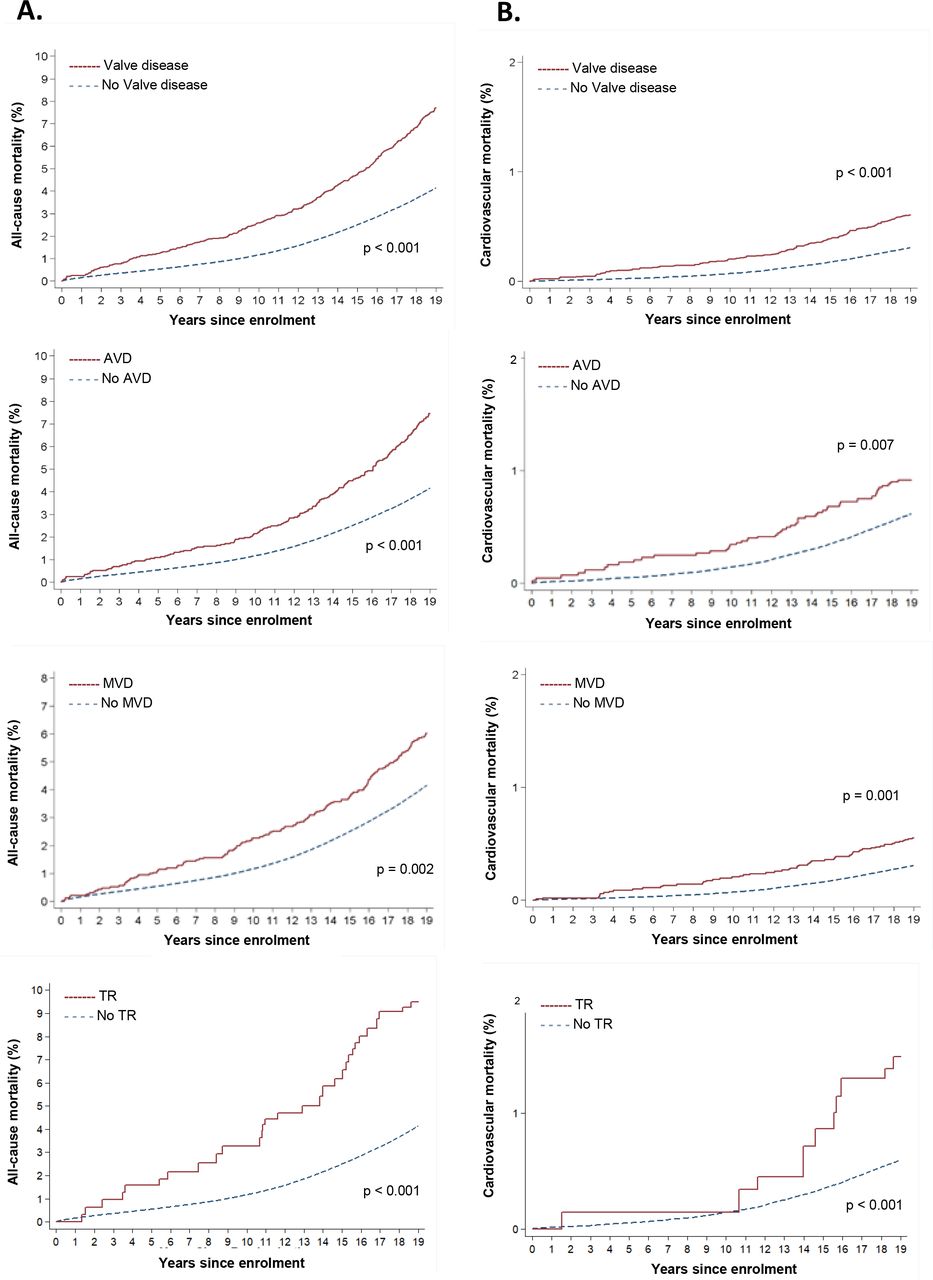
After adjusting for covariates, and despite a progressive increase in number of valve interventions over the years (figure 2), all-cause and cardiovascular mortality remained higher for patients with any VHD (HR 1.65, 95% CI 1.52 to 1.81 and HR 1.72, 95% CI 1.47 to 1.97, respectively) compared with those without VHD (figure 3). When considered separately, aortic VHD (HR 1.62, 95% CI 1.44 to 1.82; HR 1.39, 95% CI 1.09 to 1.69), mitral VHD (HR 1.25, 95% CI 1.09 to 1.44; HR 1.46, 95% CI 1.16 to 1.76) and TR (HR 2.74, 95% CI 2.24 to 3.37; HR 3.00, 95% CI 2.12 to 4.16) exhibited higher all-cause and cardiovascular mortality when compared with no VHD (figure 3). There was a trend towards higher mortality among patients who did not receive interventions compared with those who did, although not statistically significant (online supplemental figure 1).
Supplemental material
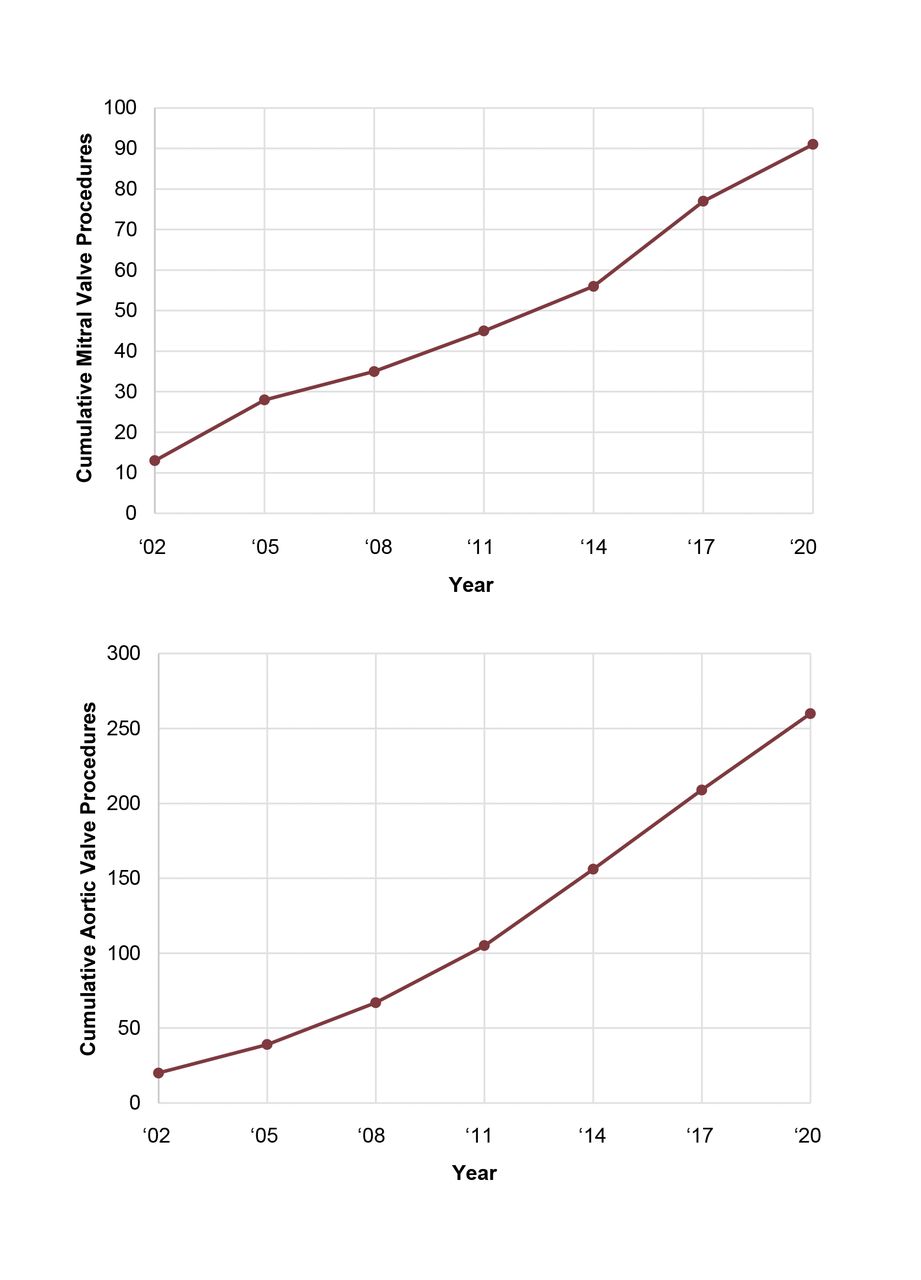
Cumulative number of mitral and aortic interventions. Number of valvular interventions during the study period includes both surgical and percutaneous procedures.
{kind=link}
{kind=link}
{kind=link}
Cumulative mortality of valvular heart disease (VHD). Kaplan-Meier survival curves for all cause (A) and cardiovascular (B) mortality associated with all VHD, and (separately) aortic, mitral, and tricuspid VHD. Models were adjusted for age, sex, systolic blood pressure, obesity, smoking, dyslipidaemia, diabetes, coronary artery disease, congestive heart failure and valvular interventions. AVD, aortic valve disease; MVD, mitral valve disease; TR, tricuspid regurgitation.
Discussion
We leveraged the UK Biobank, a large, contemporary, prospective population-based study, to demonstrate the following: (1) VHD is common and continues to constitute a significant public health burden, (2) Age and cardiac comorbidities like AF, CHF and CAD remain strong risk factors for VHD, (3) In the modern era of percutaneous and advanced surgical interventions, mortality associated with VHD remains high. The strengths of this study are the large size of the cohort, with inclusion of participants recruited from multiple community-based centres across the UK, and comprehensive record of diagnoses through linkage to both outpatient and inpatient visits across the entire National Health Service.
VHD burden
In our study, the incidence rate of any VHD was 16.3 per 10 000 person-years, and the most common valve lesions were MR, AS and AR. Although the incidence rate of VHD in the UK Biobank was high, it was lower compared with other contemporary cohorts. A study of the entire Swedish population from 2003 to 2010 determined an incidence rate of VHD of 6.4 per 10 000 person-years.6 Valve prevalence studies using transthoracic echocardiography to detect severe disease including the OxValve cohort in the UK14 and USA studies1 are in agreement with our findings that MR is the most common type of VHD, followed by AS and AR. TR incidence rate has not been previously defined in large cohorts, however, a community-based cohort identified a prevalence of 0.55% for moderate or greater TR by TTE, compared with a VA-based cohort where the prevalence was 15.6%.15 16
Risk factors for incident disease
Age and sex
Compared with other population-based studies where risk of VHD was assessed cross-sectionally, and only adjusting for age and sex,1 6 we assessed incident VHD over 20 years, and analysed the contribution of multiple risk factors in a multivariate model. After adjustment for confounders and potential mediators, we demonstrate that ageing remained an important risk for incident VHD of any aetiology, confirming the importance of age-related degenerative valvular changes.
In our study, men were at higher risk of developing VHD overall, and more so aortic valve disorders. The latter finding may be explained by hormonal differences17 or by a higher burden of other known risk factors such as aortopathies, endocarditis or bicuspid valves.6
The finding that MVP was slightly more common in men differs from other cohort-based and pedigree studies that have highlighted either a similar MVP burden in both sexes or a female predominance.18 19 This may be related to a different genetic background13 20 or different diagnostic definition (ICD codes in the UK Biobank, echocardiography in US studies).
Valvular comorbidities
Our finding that CAD and CAD risk factors (smoking, hypertension, obesity, hyperlipidaemia, diabetes) are significantly associated with incident AS supports the established paradigm that AS and its predecessor aortic sclerosis exist along the spectrum of atherosclerotic degeneration.21
Low BMI has previously been associated with both MR and TR.7 MVP typically is found in individuals with a thin body habitus,18 suggesting the coexistence of mild collagenopathies is some cases. We found that among cardiac conditions studied, AF was a strong predictor of all incident VHD subtypes. The interplay of left atrial dilation and AF has been well described and can explain this finding in the case of MR, where mitral annular dilation leads to failure of leaflets to coapt.22 Similarly, functional TR occurs in the setting of AF even in the absence of left sided heart disease.23 The heightened risk of AS among participants with AF was an unexpected finding and, to our knowledge, has not previously been described. This may reflect shared risk factors that lead to adverse remodelling of both the aortic valve and the atria. It is intriguing to consider the possibility that AF itself, such as due to a resultant unfavourable neurohormonal signalling, may lead to progression of AS.
There was a strong association between CHF and CAD with all incident VHD subtypes, which is consistent with other cohorts.6 CAD and myocardial ischaemia can cause MR and TR, while shared underlying mechanisms may underlie atherosclerosis and predisposing lesions to MS (mitral annular calcification) and AS (aortic sclerosis). Similarly, the association with CHF may be explained by the presence of functional MR and TR in this cohort. All VHD subtypes increase risk of CHF, so there is likely reverse causation or collinearity given presence of shared risk factors. Further, since most patients with CHF and CAD undergo echocardiography, VHD is more likely to be detected.
Valve disease and mortality
The presence of any VHD independently increased the risk of all-cause mortality by 65% and increased the risk of cardiovascular mortality by 72%, even after adjusting for percutaneous and modern-age surgical interventions. In comparison, a multivariate model from a Belgian cohort including age, left ventricular hypertrophy, left ventricular ejection fraction <50%, dyspnoea, Cumulative Illness Rating Scale (CIRS), found a 42% increase risk of all-cause mortality and a twofold increased risk of cardiovascular mortality, with moderate-to-severe valve disease.24 Adjustment for CIRS and echocardiographic abnormalities may explain the difference in mortality risk.
Only 316 patients in the UK Biobank cohort received aortic or mitral valve interventions. Even if we assume that only 10% of reported AS in this sample was severe, this would imply less than half received an aortic valve intervention, which is similar to a recent finding using the US-based Cardiovascular Health Study.25 A French population-based cohort found similar low uptake of valvular interventions despite high associated societal burden in mortality, readmissions and healthcare costs.26 Others have highlighted the under-referral of patients with severe MR for surgical repair27 or transcatheter edge-to-edge repair,28 and of patients with severe AS for TAVR or SAVR.29 The low absolute number of valvular interventions identified in our study may be a consequence of incorrect or insufficient coding efforts leading to underestimation of the true number of surgical or percutaneous procedures. However, the persistent excess mortality related to VHD, and across different types of VHD (figures 2 and 3), despite a cumulative increase in interventions over the past 20 years (figure 2), raises the possibility of low adherence to guideline-directed therapy, including referral to valve centres and access to interventions, similar to what observed in other European and US cohorts. In addition, similar all-cause and cardiovascular mortality in untreated compared with treated VHD suggests that valvular interventions have yet to be incorporated into current practice in a way that offers survival benefit at the population level.
Study limitations
Our study has several limitations. First, UK Biobank participants have lower rates of self-reported chronic diseases and are on average less socioeconomically deprived and more white, compared with UK census data.30 Second, available ICD-10 codes did not allow grading of VHD severity, though prior studies in Sweden and the USA have shown presence of VHD codes predict moderate or severe disease.6 11 Further studies using echocardiography to quantify valvular disease severity are needed to confirm appropriateness of interventions and low-adherence to valvular guidelines in the UK. Third, participants did not undergo universal transthoracic echocardiography screening, and participants with known cardiac conditions like CAD, CHF and AF are more likely to get screened with echocardiography. Hence, VHD may be detected at higher rates among these individuals.
In the UK Biobank, VHD continues to constitute a significant public health burden, with MR and AS being the most common. Age and cardiac comorbidities, namely CHF, CAD and AF remain strong risk factors for VHD. In the modern era of percutaneous and advanced surgical interventions, mortality associated with VHD remains high. The link between excess mortality in VHD and low-adherence to guideline-directed therapies warrants further investigation.
Data availability statement
Data may be obtained from a third party and are not publicly available. Data can be obtained by researchers through approved projects (ukbiobank.ac.uk/register-apply).
Ethics statements
Patient consent for publication
Ethics approval
UK Biobank received ethical approval from the North West - Haydock Research Ethics Committee (reference 21/NW/0157). Participants of the UK Biobank gave written informed consent prior to enrollment in the database in accordance with the Declaration of Helsinki.
Acknowledgments
This research has been conducted using the UK Biobank.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @monicatung
Contributors MT and FND contributed to conception and design of the study, including analytical methods and wrote the paper. GN and JT accessed the UK biobank data and performed all statistical analyses. GM advised on study design, data interpretation and paper writing. All authors checked and approved the final manuscript. MT and FND are guarantors.
Funding This work was supported by the National Institutes of Health NHLBI R01HL153447 (FND).
Competing interests FND has received consultant fees from Zogenix. GM has received research support from Baylis Medical. However, these relationships are not relevant to the work described in the manuscript. The remaining authors have no competing interests to disclose.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.