Article Text

Abstract
Introduction Mineralocorticoid receptor antagonists (MRAs) reduce mortality and morbidity in patients with heart failure and reduced ejection fraction (HFrEF), but are largely underused. We evaluated the frequency, motives, predictors and outcomes of MRA discontinuation in a real-world heart failure population.
Methods and results This was a single-centre, retrospective cohort study where medical record-based data were collected on patients with HFrEF between 2010 and 2018. In the final analysis, 572 patients were included that comprised the continued MRA group (n=275) and the discontinued MRA group (n=297). Patients that discontinued MRA were older, had a higher comorbidity index and a lower index estimated glomerular filtration rate (eGFR). Predictors of MRA discontinuations were increased S-potassium, lower eGFR, lower systolic blood pressure, higher frequency of comorbidities and a higher left ventricular ejection fraction. The most common reason for MRA discontinuation was renal dysfunction (n=97, 33%) with 59% of these having an eGFR <30 mL/min/1.73m2, and elevated S-potassium (n=71, 24%) with 32% of these having an S-potassium >5.5 mmol/L. Discontinuation of MRA increased the adjusted risk of all-cause mortality (HR 1.48; 95% CI 1.07 to 2.05; p=0.019).
Conclusions Half of all patients with HFrEF initiated on MRA discontinued the treatment. A substantial number of patients discontinued MRA without meeting the guideline-recommended levels of eGFR and S-potassium where mild to moderate hyperkalaemia seems to be the most decisive predictor. Further, MRA discontinuation was associated with increased adjusted risk of all-cause mortality.
- heart failure
- drug monitoring
- pharmacology, clinical
Data availability statement
Data are available upon reasonable request. Data cannot be shared due to ethical restrictions, as data contain potentially identifying or sensitive patient information, which is imposed by Ethical Review Board. The data will be shared on reasonable request to the corresponding author.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Mineralocorticoid receptor antagonists (MRAs) reduce mortality and morbidity in patients with heart failure and reduced ejection fraction, but are largely underused. A large contributor to the underuse of MRAs is discontinuation but it is not clear why and to which extent MRAs are discontinued in real-world heart failure patients.
WHAT THIS STUDY ADDS
In this study, we found that about half of all patients initiated on MRA discontinued the treatment, which is slightly higher than previous reports. The most common reasons for discontinuation in clinical practice were reduced renal function and hyperkalaemia; however, a substantial number of patients withdrew from MRA before meeting the guideline-recommended levels of estimated glomerular filtration rate and S-potassium. Continuing MRA had a benefit on survival despite initial moderately reduced function and development of worsening renal function during MRA treatment.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
We suggest that the risk of inadequate means of follow-up restrains optimal use of MRAs, especially in patients with moderately impaired renal function and/or mild hyperkalaemia. Our findings provide explanations to the gap between guideline-directed use of MRAs and real-world practice.
Introduction
Mineralocorticoid receptor antagonists (MRAs) reduce mortality and morbidity in patients with heart failure and reduced ejection fraction (HFrEF), and on this basis they have received a class 1 indication in European and US guidelines.1–5 Yet, the use of MRA remains suboptimal in patients with HFrEF.3 6–9 Discontinuation of MRA contributes mostly to its underuse since about one-third of all patients initiated on MRA discontinue treatment.6 10
Adverse effects of MRA treatment can be potentially serious and include worsening renal function, hyperkalaemia, hypotension and sexual side effects such as gynecomastia. The European Society of Cardiology (ESC) heart failure guidelines recommend half a dose of MRA if serum-potassium (S-potassium) is above 5.5 mmol/L, if serum-creatinine (S-creatinine) rises to 221 µmol/L or if the estimated glomerular filtration rate (eGFR) is under 30 mL/min/1.73 m2. However, MRA treatment should be discontinued if S-potassium rises to >6.0 mmol/L or eGFR decreases under 20 mL/min/1.73 m2.4 Serious hyperkalaemia (S-potassium >6.0 mmol/L) is associated with an increased risk of malign arrhythmias and sudden cardiac deaths and the risk of developing hyperkalaemia is higher with older age and impaired renal function.11–13 Since a majority of the HFrEF population is elderly, with a mean age of 75 years, and almost half have at least moderately impaired renal function, hyperkalaemia is an important risk to consider.14 15 Further, a significant proportion of the patients have several other comorbidities to consider.16 An abundant number of comorbidities including renal dysfunction may affect the extent of MRA treatment and the risk of MRA withdrawal in patients with heart failure.
A large contributor to the underuse of MRA is discontinuation where previous studies have shown a discontinuation rate of 30–47%.6 17 In the present study on real-world patients with HFrEF, we wanted to understand the reasons why MRA is withdrawn to such a large extent. The aims were to determine:
characteristics and outcomes in patients with HFrEF—patients continuing MRA treatment versus patients discontinuing MRA treatment,
the incidence of MRA discontinuation and reinitiation as well as predictors of MRA discontinuation including comorbidity burden, and
why MRA is discontinued in clinical practice.
Methods
Study design and patient population
This was an observational, single-centre, retrospective cohort study.
Medical records were screened for all patients who received a diagnose of heart failure (International Classification of Diseases codes I50.X, I42.0, I42.6, I42.7, I42.9, I11.0, I13.0 and I13.2) who had at least one contact with the Heart Centre or Department of medicine at Umeå University Hospital, Sweden between 2010 and 2018. We excluded all patients with EF above 40% and those who died before 1 January 2016. All patients who were treated with MRA at index were included.
Data collection
We manually collected data from the medical records regarding medical therapy, laboratory data, clinical, echocardiogram and electrocardiography parameters. Patients were included from 1 January 2010 until 20 March 2018. The start of the data collection was 1 June 2015, and the end of data collection was 28 February 2019. Index data were collected at the time of diagnosis; if the patients were diagnosed before 2010, index data were collected as close as possible to 1 January 2010. Follow-up data were collected by the journal entry closest to the end of the data collection period, which ranged from March 2016 to February 2019. The index date was chosen for analysis of baseline predictors for continuation as well as for the survival analysis.
The medical records were examined to determine if MRA had been discontinued during the study period. Temporary cessation due to, for example, hospitalisation, infection where treatment was swiftly reinitiated was not considered to be a discontinuation. Reinitiation was also determined by examination of the medical records and was only counted as a reinitiation if the treating physician had the intention that the patient would continue with the medication for a longer period of time.
To record the reasons for discontinuation, the analysis of the medical records was done by direct content analysis.18 The principles of this method are to use existing theory and prior research to identify concepts as initial coding categories. We initially used 18 codes with operational definitions to specify each code. The medical records on patients who discontinued MRA were scrutinised by one of the co-authors (AS) to determine the reasons for MRA discontinuation, and when applicable, reasons for MRA reinitiation. The paragraphs from the medical records where the reasons for discontinuation were mentioned were pasted into a data file. Co-authors AS and AJH used the paragraphs from the medical records to identify a suitable predefined coding category. Each patient was given up to three coding categories. If we did not find any explanation in the medical records, we evaluated the laboratory data with a focus on hyperkalaemia and elevated S-creatinine.
The most common index for calculation of the total comorbidity burden is the Charlson Comorbidity Index (CCI) that provides a combined score for the disease burden of the patient.19 20 CCI was calculated by searching for ICD-codes that corresponded to each comorbidity and by reviewing the medical records of each patient. Renal dysfunction was defined as eGFR lower than 60 mL/min/1.73 m2 as calculated by the revised Lund-Malmö equation. Hyperkalaemia was defined as S-potassium >5.5 mmol/L.
Outcomes
The outcomes in this study were frequency of MRA discontinuation and reinitiation. The reasons for MRA discontinuation and reinitiation were derived from the qualitative data analysis. All-cause mortality in patients with HFrEF was compared between those discontinuing MRA versus those who continued MRA during the study time.
Statistical analysis
All analyses were performed in IBM SPSS Statistics V.25. The two-tailed significance level was set at p<0.05. Categorical variables are presented as frequencies (%). Continuous variables are expressed as mean and SD when normal distributed and as medians with IQR when not normal distributed. OR and HR are presented as estimate and 95% CIs. Comparison of characteristics was carried out with the Pearson χ2 test for categorical variables and Fisher exact test when appropriate. Student’s t-test was used for continuous values with normal distribution and Mann-Whitney U test when not normal distributed.
Multivariable logistic regression was used to assess factors associated with MRA discontinuation. A subgroup multivariable logistic regressions analysis was performed by excluding all patients with S-potassium >5.5 mmol/L and eGFR <30 mL/min/1.73 m2. All covariates were included in the analysis simultaneously since our aim was to evaluate how different covariates affected the outcome and not to build a predictive model.
Associations of all-cause mortality and MRA use were assessed with the Cox proportional hazard model. We performed the analyses adjusting for the following covariates: sex, age, eGFR, S-potassium and CCI. In the CCI-score, renal dysfunction was excluded to preserve the independency since we also included eGFR as a covariate. Assumptions of proportionality of hazard were verified by log–log plots. The Kaplan-Meier method was used to construct cumulative survival groups for the discontinued and the continued MRA groups. Primary comparisons between the two groups were based on the log-rank test.
Results
From a total of 4449 patients in the heart failure population, 1739 patients had a left ventricular ejection fraction (LVEF) <40%. Sixty-nine patients were excluded due to death within 1 month after heart failure diagnosis. A total of 1137 patients were alive on 1 January 2016. Of these, 572 patients were treated with MRA and were included in the final analyses comprising the continued MRA group (n=275) and the discontinued MRA group (n=297). MRA was reinitiated in 124 (42%) of the patients that discontinued MRA. Of these 124 patients, 53 (43%) had an additional discontinuation. Patients that discontinued MRA were more often women, were older and had a slightly lower eGFR. Notably, there were no differences in treatment with angiotensin-converting enzyme inhibitor, angiotensin receptor blocker, angiotensin receptor neprilysin inhibitor, beta-blocker or LVEF (table 1).
Characteristics of patients with MRA treatment compared with patients with discontinued MRA treatment
According to the CCI score, the discontinued MRA group had a higher frequency of moderate to severe chronic kidney disease (eGFR <60 mL/min/1.73 m2), cerebrovascular disease, peripheral vascular disease and leukaemia/malignant lymphoma/metastatic cancer. Overall, the total CCI score was higher in the discontinued MRA compared with the continued MRA group (table 2).
Patients with MRA treatment compared with patients with discontinued MRA treatment
Predictors for the risk of MRA discontinuation were increased S-potassium, lower eGFR, lower systolic blood pressure, higher CCI score and higher LVEF. Notable, higher age and female sex were not associated with increased risk of MRA discontinuation in the multivariable logistic regression analysis (figure 1A). When patients with real or relative contraindications to MRA were excluded, eGFR was no longer a predictor for MRA discontinuation but all other predictors remained significant (figure 1B).
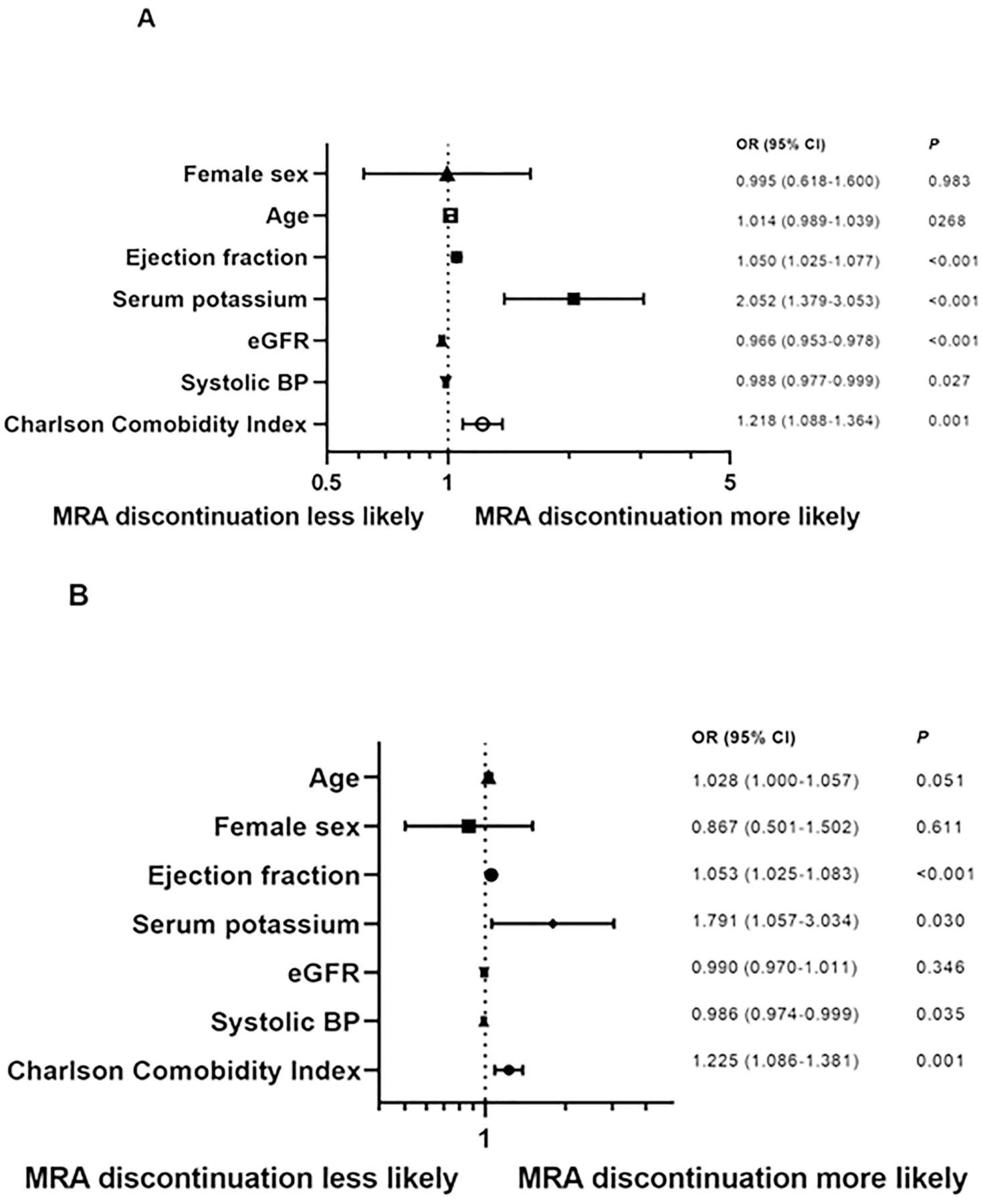
(A) Multivariable logistic regression of factors associated with MRA discontinuation for all patients (n=572). (B) Subgroup multivariable logistic regression of factors associated with MRA discontinuation, excluding all patients with formal contraindications, that is, S-potassium >5.5 mmol/L and eGFR <30 mL/min/1.73 m2 (n=427). BP, blood pressure; eGFR, estimated glomerular filtration rate; MRA, mineralocorticoid receptor antagonist.
Patients in the continued MRA group had a higher probability of survival, log rank p<0.001 (figure 2). In total, there were 184 deaths, 61 (22%) in the continued MRA group and 123 (41%) in the discontinued MRA group; the mean follow-up time was 837±705 days. Discontinuation of MRA was associated with an increased adjusted risk of all-cause mortality (HR 1.48; 95% CI 1.07 to 2.05; p=0.019), but not S-potassium or eGFR (figure 3).
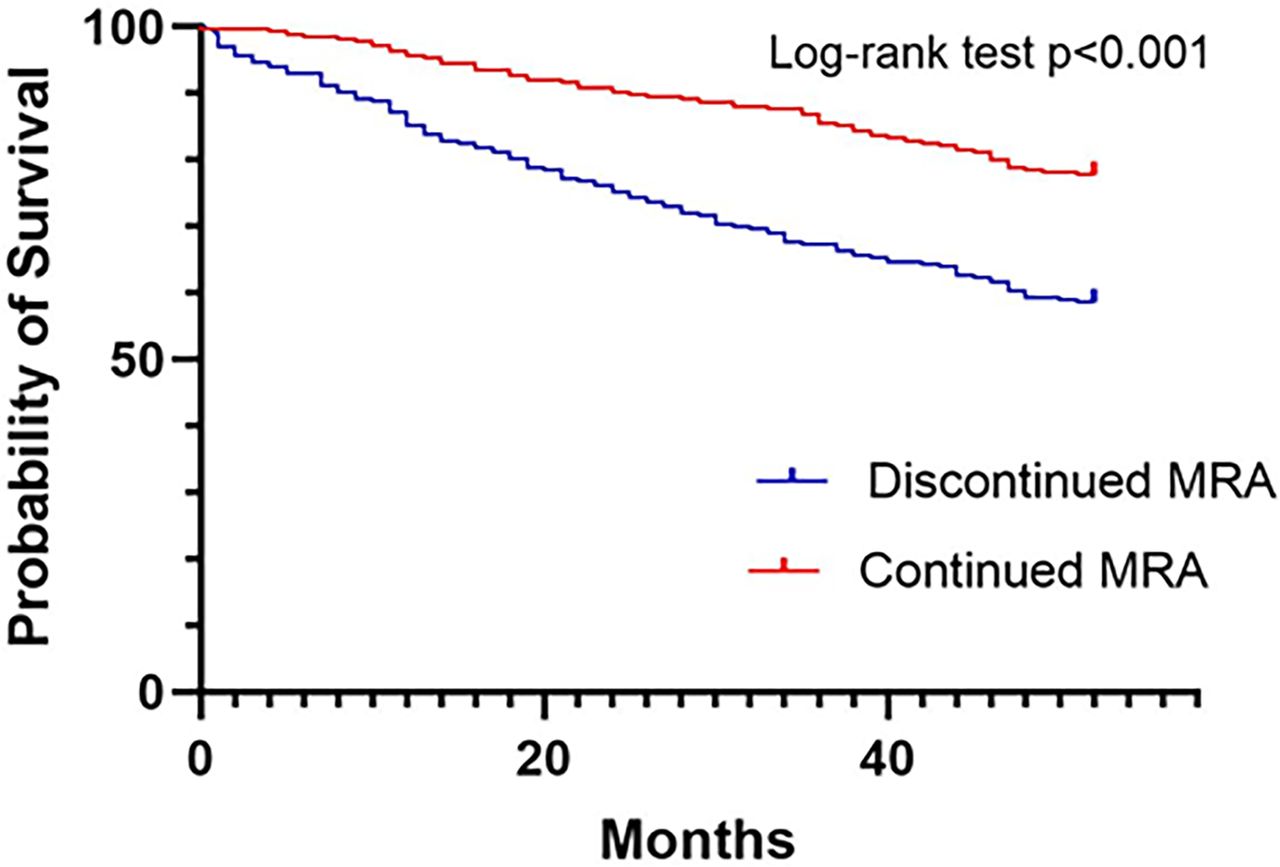
Kaplan-Meier survival plot for discontinued MRA versus continued MRA (n=572). MRA, mineralocorticoid receptor antagonist.
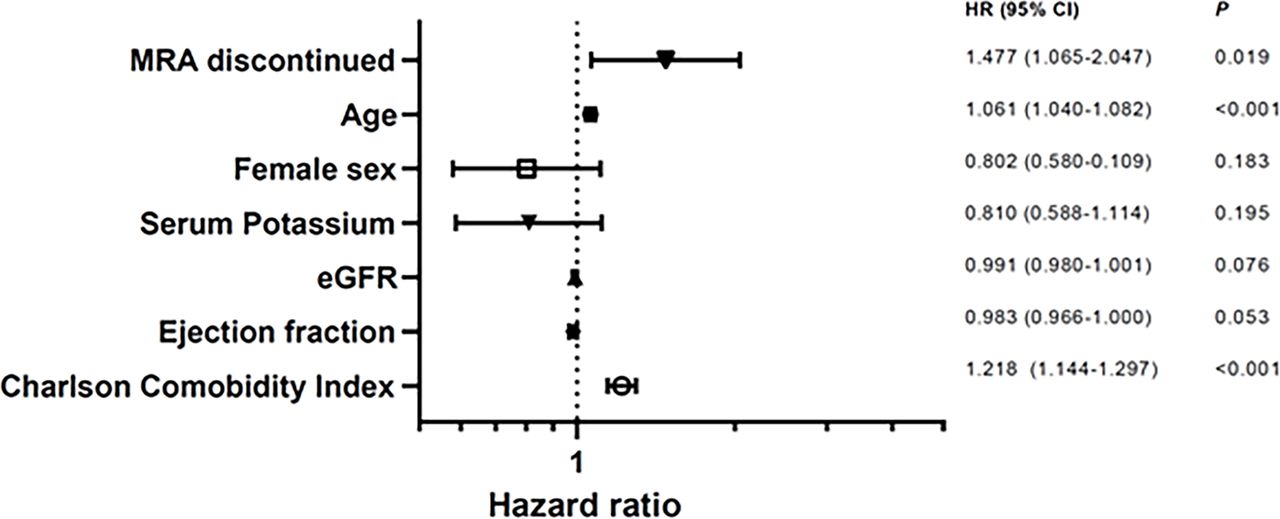
Adjusted risk of all cause-mortality in all patients (n=572). eGFR, estimated glomerular filtration rate; MRA, mineralocorticoid receptor antagonist.
The direct content analyses of the medical records showed that the most common reasons for MRA discontinuation were renal dysfunction (n=97, 33%), followed by elevated S-potassium (n=71, 24%). Low blood pressure (97±17 mm Hg) and orthostatic hypotension was the third most common reason (n=56, 19%), followed by patient-reported side effects (n=22, 7%). The most common side effects reported were vertigo, nausea, tiredness and overall reduced general condition. Lack of compliance (n=19, 6%) was another reason for discontinuation and was comprised of patients either not wanting to initiate treatment or that the patient discontinued treatment without recommendation from their physician (figure 4).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Reasons for MRA discontinuation (n=297). LVEF, left ventricular ejection fraction; MRA, mineralocorticoid receptor antagonist.
In the 97 (33%) patients with renal dysfunction as a reason for MRA discontinuation, only 54 patients (56%) had an eGFR <30 mL/min/1.73 m2 and 95 (98%) had an eGFR <60 mL/min/1.73 m2 (mean eGFR were 30±11.3 mL/min/1.73 m2). Further, 71 patients (24%) had elevated S-potassium as a reason for discontinuation, but only 23 (32%) of these had S-potassium >5.5 mmol/L and 10 (14%) had S-potassium >6.0 mmol/L (mean S-potassium (±SD) 5.4±0.6 mmol/L). Thirty-eight patients had both renal dysfunction and elevated S-potassium listed as reasons for discontinuation, which means that there were 130 patients listed with renal dysfunction and/or hyperkalaemia. Of these 130 patients, 78 (60%) had eGFR >30 mL/min/1.73 m2 and S-potassium <5.5 mmol/L.
Discussion
The most common reasons for MRA discontinuation in our heart failure population were renal dysfunction and elevated serum-potassium, but a large proportion did not have actual guideline-recommended contraindications. Our discontinuation rate of 52% is slightly higher than previously reported rates of 30–47% in previous registry and observational studies.6 17 21 22 However, comparisons between studies should take into account differences in contextual settings, populations and study designs. Nearly 50% of the patients who discontinued MRA attempted reinitiation of therapy, but about half of these had another MRA discontinuation. Of those with renal dysfunction, 98% had <60 mL/min/1.73 m2 but only 59% had eGFR <30 mL/min/1.72 m2. Moderately impaired renal function (eGFR <60 mL/min/1.72 m2) was previously described as a major limiting factor for MRA treatment.21 23 In patients with moderately impaired renal function, the risk of worsening renal function and hyperkalaemia is higher although it was shown not to affect the clinical benefits of MRA.24–26 Managing hyperkalaemia often includes withdrawal of hyperkalaemia-inducing medications such as MRA, which causes compromises as it possiblly deviates its beneficial effects on morbidity and mortality in HFrEF. A possible explanation to the high frequency of MRA discontinuation without meeting the guideline-recommended threshold is a shortage of safe follow-up and laboratory monitoring in patients at higher risks for side effects. Clinical guidelines recommend close monitoring of renal function and electrolyte levels after MRA initiation, but observational studies in real-world settings show that those guidelines are frequently not followed.27 28 Clinical monitoring within the first months of initiation is of particular importance since this is when the greatest changes in S-potassium and S-creatinine occur.17
In ESC guidelines, dose reduction of MRA is recommended if S-potassium rises above 5.5 mmol/L, and a disruption of therapy recommended if S-potassium exceeds 6.0 mmol/L. Furthermore, MRA should be re-introduced if S-potassium goes back to normal after disruption of therapy.29 In a Swedish observational study, 58% of all patients who discontinued MRA had at least one event of hyperkalaemia (S-potassium >5.5 mmol/L) during the first year of therapy; this compares to 24% of discontinuation due to hyperkalaemia in the present study where only one-third of such patients had an actual S-potassium >5.5 mmol/L.17 In our study, the high rate of withdrawal due to hyperkalaemia without an actual S-potassium over 5.5 mmol/L could be due to that half of the patients also had reduced renal function, which further increases the risk for serious hyperkalaemia. Serious hyperkalaemia (S-potassium >6.0 mmol/L) had an incidence of 1–5.5% in the Randomized Aldactone Evaluation Study (RALES), The Eplerenone in Mild Patients Hospitalization and Survival Study in Heart Failure (EMPHASIS-HF) and Eplerenone Post-AMI Heart Failure Efficacy and Survival Study (EPHESUS) trials, but this has been seen more commonly after introduction in the real-world clinical practice.1–3 12 30 In our study, only 3% of the patients had serious hyperkalaemia at discontinuation.
Noteworthy, when all patients with guideline-recommended real or relative contraindications were excluded, reduced renal function was no longer an independent predictor of MRA discontinuation, but S-potassium remained a predictor. An interpretation of this is that S-potassium levels are more decisive for MRA discontinuation in clinical practice than is decreased eGFR. Further, female sex and elderly patients were more common in the discontinued MRA group, but these were not independent predictive factors for MRA discontinuation in the multivariable analysis. It could be that women with HFrEF more often have renal dysfunction compared with men, and that renal dysfunction and other comorbidities are more abundant in the elderly.31 Low blood pressure and orthostatic hypotension was the third most common reason for discontinuation, and systolic blood pressure remained an independent predictor for discontinuation in both of the multivariable logistic regression analyses. Reduced systolic blood pressure is an independent predictor of mortality in patients with HFrEF, however, MRA was shown to have the least hypotensive effect compared with other guideline-recommended medical treatments.32 33 Therefore, it has been suggested that MRA discontinuation should be the last resort in cases with hypotension. However, there are currently no present management recommendation for hypotension in patients with HFrEF, which is why it is often a subjective clinical judgement rather than pre-defined blood pressure thresholds that determine if discontinuation is necessary as well as which guideline-recommended medical treatment should be discontinued.4
Improved EF was a reason for discontinuation in 20 patients (7%). In the Withdrawal of pharmacological treatment for heart failure in patients with recovered dilated cardiomyopathy (TRED-HF) trial, withdrawal of angiotensin-converting enzyme inhibitors/angiotensin receptor blockers, beta blockers and MRA in asymptomatic patients with dilated cardiomyopathy with improvement from LVEF less than 40% to over 50% or greater, resulted in a substantial reduction in LVEF and worsening symptoms within 8 weeks from withdrawal. This study suggests that the improvement in cardiac function following medical treatment does not reflect a sustained recovery but rather reflects remission, which is why withdrawal of medical treatment should not be attempted since it is needed to maintain the remission.34
Patients who continued MRA had a higher probability of survival (figure 2). This finding was consistent in the adjusted survival analysis where MRA discontinuation was associated with increased all-cause mortality after adjusting for relevant covariates (figure 3). These results should be interpreted with caution since this is an observational study. A majority of our patients had at least moderately impaired renal function, but eGFR was not associated with increased adjusted risk of all-cause mortality. This is in line with previous studies that show that the overall benefits of MRA on survival were present despite initial moderately reduced function and development of worsening renal function during MRA treatment.24–26 We did not show an association between S-potassium and adjusted risk of all-cause mortality. Previous studies have shown an increased mortality risk with hyperkalaemia in patients with heart failure; however, hyperkalaemia was no longer associated with increased risk after adjusting for renin-angiotensin-aldosterone-system inhibition (RAAS-I) discontinuation, but RAAS-I discontinuation was strongly associated with increased mortality.12 35–37 This may imply that hyperkalaemia is rather a risk factor for discontinuation and underuse of RAAS-I, however, further research is needed to confirm the relationship between hyperkalaemia and MRA discontinuation.
Limitations
The single-centre study design limits the generalisability and external validity of our results. Further, there is probably a portion of patients with heart failure that were treated in primary care that were not included in our heart failure population. With a retrospective observational study design, it is not possible to establish cause–effect relationship. When describing treatment effect on survival, we can only evaluate correlations between groups rather than causation. Unfortunately, the data in the medical records did not provide enough information to assess the New York Heart Association functional class.
Conclusions
In this study, we found that about half of all patients initiated on MRA discontinued the treatment. The most common reasons for discontinuation in clinical practice were reduced renal function and hyperkalaemia; however, a substantial number of patients withdrew from MRA before meeting the guideline-recommended levels of eGFR and S-potassium. S-potassium levels seem to be more decisive for MRA discontinuation than renal dysfunction. Further, MRA discontinuation was associated with increased adjusted risk of all-cause mortality, but not eGFR and S-potassium levels.
Supplemental material
Data availability statement
Data are available upon reasonable request. Data cannot be shared due to ethical restrictions, as data contain potentially identifying or sensitive patient information, which is imposed by Ethical Review Board. The data will be shared on reasonable request to the corresponding author.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by The Regional Ethical Review Board in Umeå, Sweden (registration number 2015/419- 31 and 2016/233-32M). Patients’ medical records are protected by confidentiality by the Public Access to Information and the Secrecy Act but can be available for research purposes after approval by an Ethical Review Board. A paper stating that information from the health care visit could be used in research and quality registries was placed at the outpatient cardiology clinic, the cardiology care unit and cardiology ward. We did not obtain informed consent from the included patients, which was waived by the Ethical Review Board. Since health care data are classified as especially sensitive information, the responsibility for none-disclosure is essential. The non-anonymised database was stored on a computer protected by the firewall of Umeå University Hospital. The responsible researcher gave each patient a specific code, and the anonymous coded database was used in all statistical analyses. No individual data could be identified in the results since all statistical analyses were presented on a group level. This study complies with the Declaration of Helsinki.
Acknowledgments
The authors thank all personnel who obtained data for the study. This work has previously been published as a preprint in the first author’s doctoral thesis.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors AJH, KL, HN contributed to conceptualisation and study design. AS, AJH, GW contributed to data acquisition. AJH, HN contributed to data analysis. AJH contributed to writing—original draft preparation. HN, AS, FV, EB, KL contributed to writing—reviewing and editing. HN, KL, FV, EB contributed to supervision. AJH is responsible for the overall content as guarantor. All authors read and approved the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.