Article Text

Abstract
Objective Pulmonary arterial hypertension (PAH), caused by pulmonary artery remodelling and increased pulmonary vascular resistance (PVR) due to an unknown mechanism, is an intractable disease with a poor prognosis. The recent development of PAH-specific treatment medications may allow for higher PVR reduction than previously achieved. This study aimed to identify the prognostic significance of follow-up PVR levels achieved shortly after the initiation of targeted treatment in patients with idiopathic/heritable pulmonary arterial hypertension (I/H-PAH).
Methods We analysed the data of all patients with I/H-PAH admitted to our hospital between 1998 and 2019. We collected data at baseline and during the first invasive haemodynamic evaluation. The primary outcome was death or lung transplantation.
Results Of the 133 treatment-naïve patients enrolled in this study, 47 experienced adverse events during a median follow-up period of 6.4 (IQR 3.5–11.5) years. The median time interval to first follow-up from diagnosis was 162 (IQR 117–253) days. Incidence of the primary outcome was significantly lower in patients who achieved low PVR at follow-up. Of risk factors evaluated at follow-up, the multivariate Cox regression analysis revealed PVR as an independent predictor of the primary outcome (HR 1.103, 95% CI 1.029 to 1.183; p=0.006). The results were consistent across risk profiles according to the simplified risk stratification recommended by the European Society of Cardiology and European Respiratory Society guidelines.
Conclusion Follow-up PVR was an independent predictor of transplant-free survival in patients with I/H-PAH. Evaluation of haemodynamic status shortly after initiating treatment may help predict long-term prognosis.
- pulmonary arterial hypertension
- hypertension, pulmonary
- drug interactions
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Outcomes of patients with pulmonary arterial hypertension (PAH) are determined by the right ventricular (RV) function adapted to increased afterload. Although several risk scores are derived based on the European Society of Cardiology (ESC) and the European Respiratory Society (ERS) guidelines, the prognosis of patients categorised in the low-risk status is not completely managed. Decreasing pulmonary vascular resistance (PVR) from the early phase of treatment by multiple combination therapy may prevent RV failure, leading to a better prognosis.
WHAT THIS STUDY ADDS
Follow-up PVR evaluated shortly after initiating PAH-specific treatment medications was an independent predictor of transplant-free survival in patients with idiopathic/heritable pulmonary arterial hypertension (I/H-PAH). The results were consistent across risk profiles according to the simplified risk stratification recommended by the ESC/ERS guidelines. The addition of PVR assessment to the recommended risk score was useful to predict adverse events in these patients.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE AND/OR POLICY
Prospective RV function mainly depends on the pulmonary vascular response to PAH therapy and decreased PVR at follow-up. Patients with high PVR remain at risk of developing RV failure, leading to a poor prognosis, even though they may achieve a low-risk profile. In the current era with the availability of multiple drug combinations for treating patients with I/H-PAH, tailoring further treatment according to the follow-up PVR levels may improve prognosis.
Introduction
Idiopathic/heritable pulmonary arterial hypertension (I/H-PAH) is a rare disease characterised by remodelling of the pulmonary vasculature. The treatment of this disease has changed dramatically over the last two decades due to the development of pulmonary arterial hypertension (PAH)-specific treatment medications. Currently, we have three types of vasodilators that target the pulmonary artery via different mechanisms, contributing to an increase in cardiac output and a reduction of pulmonary vascular resistance (PVR).
Several risk scores that mainly include parameters associated with cardiac output are used to stratify patients with I/H-PAH.1–4 However, the prognosis of patients categorised in the low-risk status is not completely managed, with an estimated 5-year survival of 68%–92%.2 3 5 Thus, tools for risk stratification in patients with I/H-PAH are needed to improve the management of these patients.
PVR is indicative of the afterload burden on the right ventricle. Persistently high PVR leads to right ventricular (RV) dysfunction. Because outcomes of patients with PAH are determined by the RV function adapted to increased afterload,6–9 decreasing PVR from the early phase of treatment could prevent RV failure, leading to a better prognosis. Reported improvements in haemodynamic parameters due to the recent introduction of targeted combination therapy have led clinicians to expect a stronger reduction in PVR, leading to RV reverse remodelling.10–15 A recent study from Italy reported that both a good pulmonary vascular response and PVR reduction attained with combination therapy could predict future low-risk status.16 However, little is known regarding the association between long-term prognosis and PVR levels following the administration of combination therapy to manage PAH. Furthermore, as the US Registry to Evaluate Early and Long-Term PAH Disease Management (REVEAL) study investigated that follow-up risk assessment was a much stronger predictor of adverse events than baseline evaluation,17 from the perspective of pulmonary vascular response to PAH-targeted drugs, serial PVR measured after initial treatment introduction may be a meaningful factor.
Therefore, we aimed to identify the prognostic significance of follow-up PVR shortly after administering vasodilators in patients with I/H-PAH.
Methods
Study population
This was a retrospective, single-centre cohort study. We enrolled 162 consecutive patients with I/H-PAH, referred to the National Cerebral and Cardiovascular Center (Osaka, Japan) between January 1998 and December 2019. They were diagnosed with I/H-PAH based on the guidelines prevalent at the time. Precapillary pulmonary hypertension (PH) was defined as a mean pulmonary arterial pressure (mPAP) of ≥25 mm Hg at rest and a pulmonary arterial wedge pressure (PAWP) of ≤15 mm Hg. Patients diagnosed with precapillary PH were classified as those with chronic thromboembolic PH (WHO clinical classification system 4) and those with PH due to lung disease (WHO clinical classification system 3) based on findings of lung perfusion scans (no ventilation/perfusion mismatch) and pulmonary function tests (forced expiratory volume in 1 s >70% and total lung capacity >80%), respectively. Furthermore, we also screened for PAH associated with connective tissue disease using antinuclear antibody testing. We additionally excluded 10 patients who were already treated with pulmonary vasodilators before enrolment, 9 patients who died before their first invasive haemodynamic evaluation and 11 patients who could not be stratified for PAH-risk assessment based on the European Society of Cardiology (ESC) and the European Respiratory Society (ERS) guidelines due to unavailability of relevant data.18 Data of the remaining 133 treatment-naïve patients were used for the final analysis. Patients were divided into two groups according to the median PVR level: the low-PVR group (PVR ≤10 Wood units (WU)) and the high-PVR group (PVR >10 WU) in the entire cohort and each risk profile according to the risk stratification method. Written informed consent was waived because of the retrospective design. The opt-out method was applied to obtain consent.19
Measurements and data collection
We collected the following clinical data from medical records at baseline and at the time of the first invasive haemodynamic evaluation at follow-up: age, sex, WHO functional class, 6 min walk distance (6-MWD), laboratory data, ongoing medications and haemodynamic parameters (mean right atrial pressure (RAP), mean PAWP, mPAP, mixed venous oxygen saturation (SvO2), cardiac index and PVR) measured during right heart catheterisation. Combination therapy was defined as two or more different types of PAH-specific treatment medications administered to the patient. Right heart catheterisation was performed with a 7-Fr balloon wedge pressure catheter (Harmac Medical Products, New York, USA) with the patient in a supine position. PAWP and RAP were measured at the end of expiration. Cardiac output was determined using the indirect Fick method and was corrected for body surface area (cardiac index). Additionally, we divided patients into low-risk, intermediate-risk and high-risk groups using a comprehensive risk stratification system2 3 based on the ESC/ERS guidelines18 to evaluate the prognostic significance of PVR in patients at different levels of risk of PAH. Each variable was graded from 1 to 3 (1=low risk, 2=intermediate risk and 3=high risk) for the risk assessment. The sum of all grades was divided by the number of available variables and was rounded off to the nearest integer to quantify patients’ risk levels and accordingly assign them to the applicable risk group. Survival status was confirmed in July 2020 by reviewing clinical records. The primary outcome was defined as a composite of all-cause death and lung transplantation.
Statistical analysis
Continuous variables were presented as mean±SD if normally distributed, and as median and IQR if non-normally distributed. Normality was assessed using the Shapiro-Wilk W test. Comparisons between baseline characteristics were made using a contingency table, and the Pearson χ2 test was applied to evaluate categorical variables. The t-test and Wilcoxon signed-rank test were used for the normally and non-normally distributed continuous variables. Kaplan-Meier survival plots were created starting from baseline until the occurrence of the primary outcome and were compared using the log-rank test. Univariate and multivariate Cox proportional hazards analyses were used to evaluate the HRs and 95% CIs of parameters associated with the composite endpoint. On multivariate analysis, we selected other well-established predictors of risk as covariates. C-statistics of 5-year transplant-free survival were calculated to evaluate whether the addition of PVR would enhance the performance of the risk score. Statistical significance was set at a p value of <0.05. All statistical analyses were performed using the SPSS Statistics software for Windows V.26.
Patient and public involvement
Patients or the public were not involved in our research’s design, recruitment, conduct, and reporting.
Results
Patient characteristics
Of the 133 patients (median age, 33 years; female, 73%) enrolled in this study, 47 (35.3%) experienced the primary outcome (death, 43; lung transplantation, 4) during a median follow-up period of 6.4 (IQR 3.5–11.5) years. The median time interval between diagnosis and the first follow-up was 162 (IQR 117–253) days. Baseline characteristics at diagnosis and the first follow-up are summarised in table 1. At the first follow-up, parameters including the WHO functional class, 6-MWD, B-type natriuretic peptide level and haemodynamic variables (cardiac index, SvO2, mPAP, PVR and PAWP) in all patients had significantly improved as compared with those at diagnosis. The median reduction in PVR was −30.5% (IQR 0.0% to −57.7%). Combination therapy was administered to 48/133 (36%) patients, of which upfront combination therapy was adopted in 42. The proportion of patients who attained a low-risk status at follow-up was significantly higher in those who received combination therapy (77.1% vs 42.4%, p<0.001). Similarly, those who had combination therapy demonstrated a significantly higher reduction in PVR than that observed in those treated with monotherapy (−59.5% (−40.6% to −78.6%) vs −14.1% (0.0% to −32.8%), p<0.001). Baseline characteristics according to PVR levels at follow-up are shown in table 2.
Patient characteristics
Patient characteristics according to PVR levels at follow-up
Risk group distributions at baseline and follow-up
According to the ERS/ESC guidelines risk assessment, at the time of diagnosis, the low-risk, intermediate-risk and high-risk group included 25 (19%), 86 (65%) and 22 (17%) patients with 2/25 (8%), 32/86 (37%) and 13/22 (59%) patients having experienced adverse events, respectively (p=0.001). At follow-up, 73 (55%), 57 (43%) and 3 (2%) patients were categorised as being at low, intermediate and high risks with 15/73 (21%), 29/57 (51%) and 3/3 (100%) patients having experienced adverse events, respectively (p<0.001). A histogram of the percentage changes in the risk score from diagnosis to the first follow-up is shown in online supplemental figure 1. Kaplan-Meier plots according to risk profiles sorted at baseline and follow-up are shown in online supplemental figure 2. Although event-free survival rates were higher in patients categorised in lower-risk profiles, the estimated 5-year transplant-free survival was 86.7% in patients who attained the low-risk status at follow-up.
Supplemental material
Prognostic impact of PVR
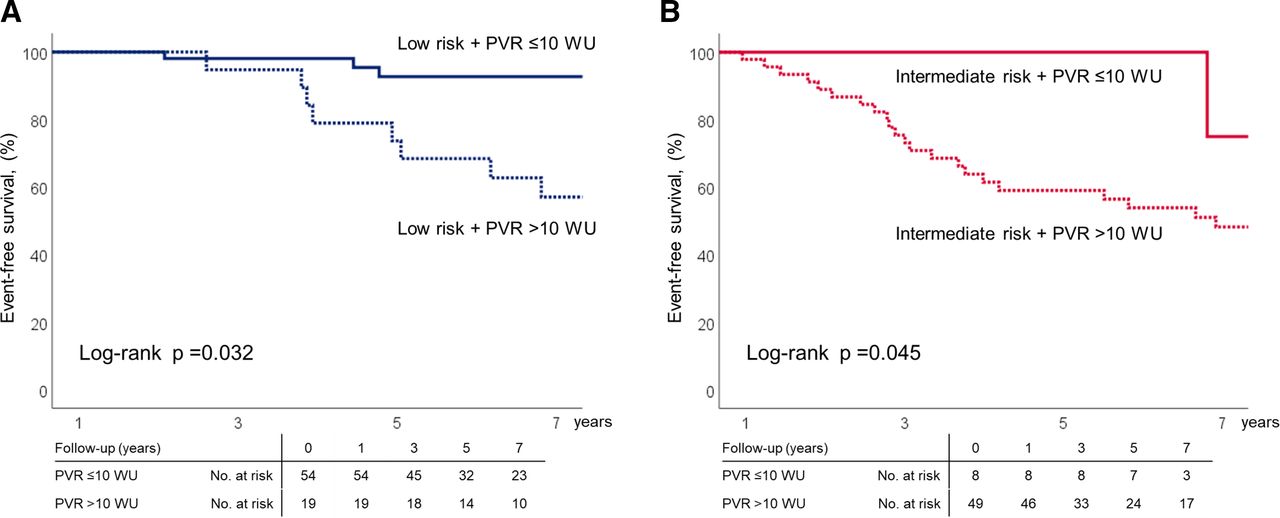
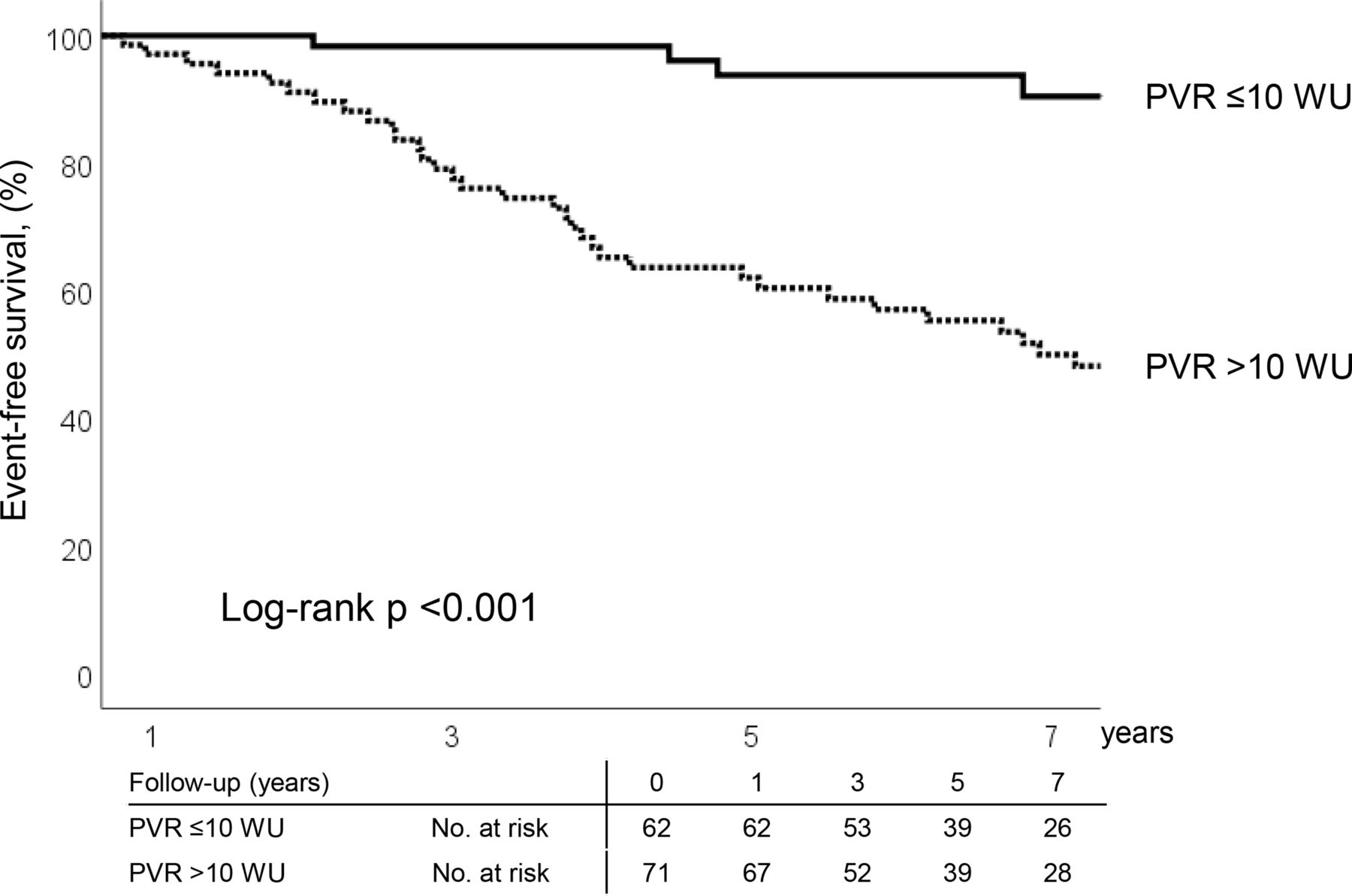
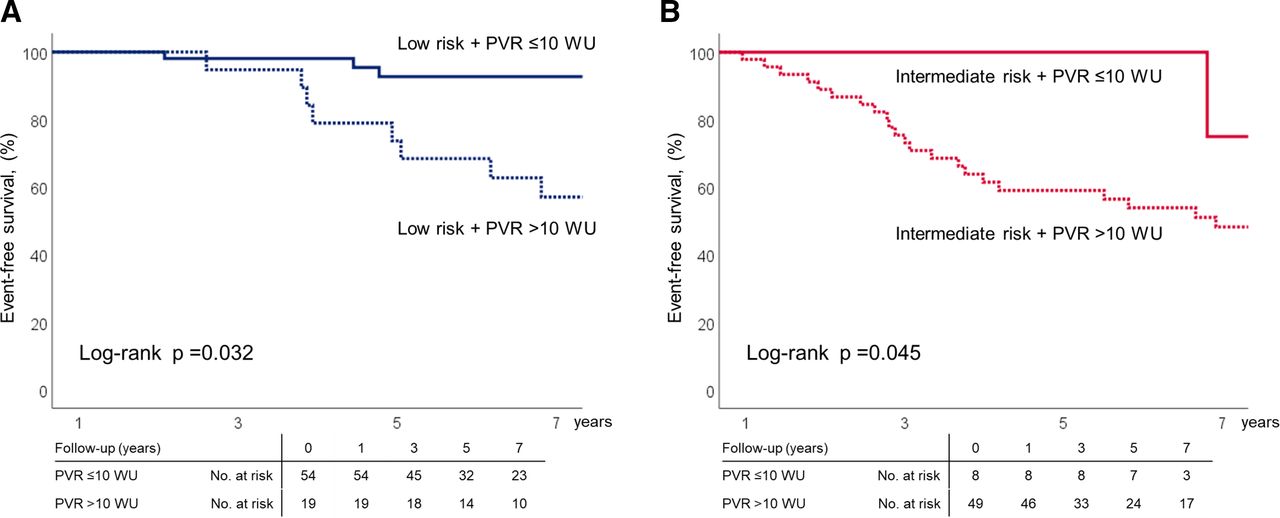
PVR level at diagnosis was not an independent predictor of the primary outcome (HR 1.040, 95% CI 0.979 to 1.104; p=0.203). Conversely, multivariate Cox regression analysis revealed that of all assessed risk factors, PVR measured at follow-up was an independent predictor of the primary outcome (HR 1.103, 95% CI 1.029 to 1.183; p=0.006) (table 3). RAP (HR 1.264, 95% CI 1.098 to 1.455; p=0.001), WHO functional class (HR 13.167, 95% CI 1.728 to 100.315; p=0.013), and B-type natriuretic peptide (HR 0.996, 95% CI 0.993 to 1.000; p=0.037) at follow-up were also found to be independent predictors of adverse outcomes. Cumulative event-free survival rates were significantly higher in patients with low follow-up PVR (figure 1). PVR of >10 WU at follow-up was associated with adverse events even in patients at low risk over 3 years (the estimated 5-year transplant-free survival rate in low-risk patients was 92.7% and 73.7% with PVRs of ≤10 and >10 WU at follow-up, respectively) (figure 2). In the intermediate-risk group at follow-up, the risk of mortality was significantly lower in patients with low PVR (PVR ≤10 WU vs PVR >10 WU, 1/8 vs 27/48; p=0.022), and the estimated 5-year transplant-free survival rates were 100% and 59.0% in those with PVRs of ≤10 and >10 WU, respectively. All high-risk profile patients had a PVR of >10 WU at follow-up and demonstrated an estimated 5-year transplant-free survival rate of 33.3%. The C-statistics of 5-year transplant-free survival when achieving only the low-risk status and achieving both the low-risk status and PVR of ≤10 WU at follow-up were 0.667 and 0.744, respectively.

Kaplan-Meier plots of primary outcomes according to follow-up PVR levels. PVR, pulmonary vascular resistance; WU, wood unit.
{kind=link}
{kind=link}
Kaplan-Meier plots of primary outcomes according to follow-up PVR levels across each risk status group stratified according to the European Society of Cardiology/European Respiratory Society risk score. (A) Low-risk group. (B) Intermediate-risk group. PVR, pulmonary vascular resistance; WU, wood unit.
Cox proportional hazards analysis
Discussion
The novel finding of the present study was that follow-up PVR was significantly associated with long-term prognosis in patients with I/H-PAH, a finding consistent across risk profiles according to the simplified risk stratification system recommended in the ESC/ERS guidelines. The addition of PVR assessment to the recommended risk score was useful to predict adverse events in these patients.
Although the REVEAL registry investigated the association between baseline PVR and short-term mortality in patients with PAH,1 20 other earlier studies reported that baseline PVR was not an independent predictor of adverse events in affected patients.9 21 22 The latest ESC/ERS guidelines do not include parameters indicative of the RV afterload as a part of the recommended risk assessment.18 However, the mortality risk of patients categorised in the low-risk profile is still not well enough, and further risk stratification tools are needed. The prognostic utility of follow-up risk assessments has been demonstrated in previous studies,2 17 23–26 which indicates the necessity of evaluating patients not only at baseline but also after targeted PAH treatment is introduced. A recent study focusing on serial PVR changes in patients with PAH reported that the decrease in PVR due to combination therapy was an additional predictor of a patient’s low-risk status in the future.16 Another study demonstrated that initial combination therapy would improve the REVEAL risk score in proportion to decreased PVR.14 From these studies, it may be possible to suggest that pulmonary vasculature response against specific therapy may be a meaningful parameter in treating these patients. Previous studies indicate that in terms of long-term prognosis, follow-up PVR assessed after treatment introduction could be more important than baseline PVR measured at the treatment-naïve status.
RV dysfunction and right heart failure are the predominant causes of death in patients with PAH.6 7 van de Veerdonk et al reported an association between RV function and poor prognosis in patients with PAH, regardless of PVR reduction.8 In their study, one-fourth of patients experienced a deterioration of RV function despite a PVR decrease. However, the mean reduction rates of PVR and mPAP at follow-up in their study were only 14.5% and 6.0%, respectively (31.2% and 14.7%, respectively, in our cohort), suggesting that they did not achieve adequate PVR reduction. In the combination therapy era, patients who attain low PVR at follow-up regardless of their levels at baseline would maintain their RV function,15 leading to a better long-term prognosis.
The introduction of multiple combination therapies has led to a stronger reduction in PVR. Reportedly, a 30%–65% reduction in PVR was observed using combination therapy.14 15 27–29 Similarly, in our study, a significantly greater decrease in PVR was observed at the first follow-up in patients who had received combination therapy. Although the proportion of combination therapy was relatively low, this was because of the treatment produced in the old era, and approximately 80% of patients were receiving multiple PAH drugs at first follow-up in patients enrolled in the recent 10 years. The prognosis of patients who received combination therapy was also significantly better in our study cohort, similar to previous reports.30 Reduction in PVR due to combination therapy may contribute towards improving prognosis in patients with I/H-PAH.
In the present study, we investigated the prognostic significance of PVR measured at first follow-up after initiating treatment. To the best of our knowledge, no other study has investigated the utility of PVR in patients with I/H-PAH in addition to the risk assessments recommended in the ESC/ERS guidelines. As previously reported, there was no relationship between adverse events and baseline PVR measured before the prescription of PAH drugs. It may be challenging to identify the prognostic risk only by assessing the haemodynamic parameters in the treatment-naïve status17; prospective RV function mainly depends on the pulmonary vascular response to PAH therapy and decreased PVR at follow-up. The estimated 5-year survival rate of patients at intermediate risk with low PVR at follow-up was higher than that of patients at low risk with high PVR. Patients with high PVR remain at risk of developing RV failure, leading to a poor prognosis, even though they may achieve a low-risk profile. In the current era with the availability of multiple drug combinations for treating patients with I/H-PAH, tailoring further treatment according to the follow-up PVR levels may improve prognosis. The multivariate Cox model in our study did not show an independent association between several well-established predictors (such as cardiac index) and adverse events. This may be because of the small sample size and due to the strong correlation between PVR and cardiac index (Spearman’s rank 0.831, p<0.001). Weatherald et al reported that follow-up stroke volume index could be a more appropriate treatment target than cardiac index in patients with PAH.24 This is explained by the fact that cardiac index could be maintained by increasing heart rate without any improvement, or even with worsening, in RV function. Although we did not include stroke volume index in our Cox model because of the strong correlation with cardiac index and PVR, stroke volume index should also be evaluated when treating these patients. As with other reports from Japan,5 31 the patient cohort in our study was younger than that of Western countries. It is reported that there is a high proportion of genetic mutation in Japanese patients with I/H-PAH,32 which may be the reason for the young onset. The young patient cohort may be one of the reasons why the survival rate in patients with I/H-PAH in Japan is higher than that in Western countries,2 3 5 and it may have affected the results similarly in the present study.
Our findings suggest that follow-up PVR could be a valuable additional prognostic predictor while treating patients with I/H-PAH, regardless of their status of risk as per the ESC/ERS guidelines. Aggressive therapy with multiple drugs may be considered when PVR remains persistently high at follow-up, even if the patient has attained a low-risk status. It is difficult to determine the optimal cut-off value of PVR only by this study, and further randomised control trials and observational studies with more patients are needed to verify our hypothesis.
Our study has several limitations. First, consecutive patients enrolled in this study were from a single centre, which may represent a selected cohort. Second, only 133 treatment-naïve patients were included in a 22-year period. This long observation period introduced a bias due to the development of PAH-specific treatment medications over the last two decades. Third, we did not have detailed data on RV function of all patients, such as cardiac MRI findings. Fourth, our study measured cardiac output using the indirect Fick method, although the ESC/ERS guidelines recommend the thermodilution or direct Fick method. Even though a previous report has demonstrated that both indirect Fick and thermodilution methods are useful for assessing cardiac output in patients with PAH,33 this may have affected the results. Finally, as patients who died before their first haemodynamic evaluation were not included in our study, the most severe cases of PAH may have been excluded from the analysis.
In conclusion, follow-up PVR predicted poor outcomes in patients with I/H-PAH. We should assess PVR after the initiation of PAH-specific drugs to stratify the precise risk in affected patients.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants. The study protocol was approved by the ethical committees of the National Cerebral and Cardiovascular Center (approval number R20075). The participants gave informed consent to participate in the study before taking part. The investigation conformed to the principles outlined in the Declaration of Helsinki.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors Guarantor: TO. Conception and design: SS, RA, TA and TO; acquisition of data: SS, RA, JU, TA, AT and TO; analysis and interpretation of data: SS, TA and TO; drafting the article and revising it critically: SS, RA, TA and TO; final approval: TN and TO.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests TO received lecture fees from GlaxoSmithKline K.K., Actelion Pharmaceuticals Japan, Nippon Shinyaku Co., Pfizer Japan and Bayer Yakuhin, and research grants from Pfizer Japan and Mochida pharmaceutical Co. TO belongs to the endowed department of Nippon Shinyaku.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.