Article Text

Abstract
Objective Congestive acute kidney injury (c-AKI) refers to AKI in the presence of right ventricular failure (RVF) and is a highly morbid complication of cardiac surgery. However, treatment has traditionally been reactive rather than proactive due to limited modalities to predict this complication. The objective of this study was to investigate the ability of insulin-like growth-factor binding protein 7 (IGFBP7), to predict c-AKI, AKI and RVF in patients undergoing cardiac surgery, as compared to N-terminal prohormone B-type natriuretic peptide (NT-pro-BNP) and pulmonary artery pulsatility index (PAPi).
Methods This prospective nested case–control study consisted of 350 adult patients who underwent elective cardiac surgery. The outcomes were c-AKI, AKI and RVF. Unadjusted and adjusted conditional logistic regression models and areas under the receiver operating characteristic curve (AUC) were used to assess the predictive performance of each marker.
Results For the prediction of c-AKI, the unadjusted IGPBP7 model had an AUC of 0.81, as compared with 0.51 for NT-pro-BNP and 0.61 for PAPi. The adjusted c-AKI models had AUCs of 0.90 for IGFBP7, 0.87 for NT-pro-BNP and 0.77 for PAPi. For AKI and RVF, the predictive performance of IGFBP7 was moderate and exceeded that of NT-pro-BNP and PAPi in univariable analysis. IGFBP7 remained a robust independent predictor of all outcomes in multivariable analysis, whereas the other markers did not.
Conclusions IGFBP7 is a promising biomarker for prediction of AKI, RVF and c-AKI and could have value for preoperative optimisation and risk stratification of patients undergoing cardiac surgery.
- cardiac surgery
- biomarkers
- heart failure
Data availability statement
Data are available on reasonable request. Data available on request due to restrictions. The data presented in this study are available on request from the corresponding author. The data are not publicly available due to privacy restrictions.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Prevention has been shown to be the best treatment for acute kidney injury (AKI) and right ventricular failure (RVF) after cardiac surgery. However, there is currently a lack of effective predictors of these complications.
WHAT THIS STUDY ADDS
GFBP7 is a highly effective biomarker for predicting postoperative AKI and RVF.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE AND/OR POLICY
A single, preoperative point-of-care serum IGFBP7 measurement could augment the clinician’s ability to identify high-risk patients for perioperative optimisation, prevent important complications and improve patient outcomes.
Introduction
Right ventricular failure (RVF) and acute kidney injury (AKI) are important risk factors for morbidity and mortality following cardiac surgery.1–4 Prediction and early identification of these outcomes is critical for clinical risk stratification and timely, aetiology-specific prevention and treatment.3
Congestive AKI (c-AKI) refers to AKI in the presence of RVF with worse outcomes than its individual components.3 It is an emerging concept that highlights the importance of end organ dysfunction in the survival of patients with RVF. The most effective treatment of c-AKI and RVF is preventative rather than reactive, including preoperative diuresis, volume optimisation and early inotrope use.5 However, to date, no single effective method exists for the prediction of these complications in the perioperative setting. The prediction of c-AKI may be enhanced when combining clinical variables with biomarkers, of which N-terminal prohormone B-type natriuretic peptide (NT-pro-BNP) has demonstrated the most promise in patients undergoing cardiac surgery.3 The utility of NT-pro-BNP has also been investigated in association with RVF and found to perform modestly at best in the perioperative setting.2 5 Aside from biomarkers, the central venous pressure (CVP) and Pulmonary Artery Pulsatility Index (PAPi) are two haemodynamic markers with moderate ability to predict postoperative RVF and c-AKI.3 6 Both haemodynamic markers are load-dependent, with limited evidence to support their routine clinical use.6 Given the limitations of haemodynamic markers and the nonspecific nature of NT-pro-BNP, investigations have turned to the discovery of RVF-specific biomarkers to improve clinical risk stratification and guide therapeutic decisions in this high-risk patient group.7 8
Insulin-like growth factor binding protein 7 (IGFBP7) is a novel biomarker which functions as an inducer of G1 cell cycle arrest, a known mechanism implicated in the pathogenesis of AKI.9 It has been shown in combination with tissue inhibitor of metalloproteases-2 (TIMP2) to predict AKI after cardiac surgery in multiple studies,10 11 as well as being a biomarker of heart failure with preserved ejection fraction.10 12 The objective of this study was to investigate the ability of IGFBP7 to predict c-AKI, AKI and RVF in patients undergoing cardiac surgery, as compared with other potential markers.
Materials and methods
Patient recruitment and study procedures
The details of the study design and patient recruitment process were described elsewhere.3 The patient population consisted of 350 consecutive consenting adult patients who underwent major elective cardiac surgery at the University of Ottawa Heart Institute between 2015 and 2017. Patients, who underwent off-pump procedures, heart transplantation, left ventricular assist devices and procedures requiring circulatory arrest, were excluded. Patients’ baseline characteristics, operative data and outcomes were documented by trained research staff. Baseline echocardiographic assessment of right ventricular function was obtained for all patients by the attending anaesthesiologist, who also noted any difficulty encountered during cardiopulmonary bypass separation.
Outcomes
The primary outcome was c-AKI, as defined by the co-occurrence of AKI and RVF. The secondary outcomes were individually, AKI and RVF. AKI was defined by the Acute Kidney Injury Network criteria13 and postoperative RVF was defined according to criteria established by our group and others.3 7 8 Outcomes were ascertained within 48 hours of surgery and their definitions are presented in detail in table 1.
Diagnostic criteria for primary and secondary outcomes
Cases and controls
Cases were defined as patients with postoperative AKI, RVF or c-AKI. Controls were free of these complications during the follow-up period. Cases and controls were matched 1:1 based on age and sex. All patients received routine standard of care.
Biomarkers
Biomarkers were sampled at baseline immediately following anaesthesia induction. Biomarker samples were centrifuged and plasma supernatants stored at −80°C until analysis. Plasma NT-pro-BNP (Roche Diagnostics) was measured using commercially available US food and Drug Administration-approved electrochemiluminescence immunoassays with a Roche Cobas e411 anaylzer. The manufacturer’s normal reference range for NT-pro-BNP was <300 pg/mL.14 15 IGFBP7 was measured using the Elecsys assay (Roche Diagnostics), with a limit of detection of 0.01 ng/mL.10
Haemodynamic variables
Haemodynamic variables were measured by pulmonary artery catheterisation by the attending anaesthesiologist after anaesthesia induction. These included CVP, systolic and diastolic pulmonary artery pressure (PAPs and PAPd). PAPi was calculated as  .
.
Statistical analysis
Statistical analyses were performed using SAS V.9.4 (SAS Institute) and graphics were produced with R V.4.0 (R Foundation, New Zealand). Categorical variables were compared using Fisher’s exact test for binary variables and χ2 test for variables with three or more categories. Continuous variables were compared using Wilcoxon rank sum test or Student’s t-test where appropriate. Patients with any missing data for the variables of interest were excluded from the analysis.
We used conditional logistic regression to model the association of each of the preoperative markers (IGFBP7, NT-pro-BNP, PAPi) with AKI, RVF and c-AKI. All three preoperative markers were included in the models as continuous variables. Unadjusted models were univariate, containing only the marker in question. A total of nine unadjusted and nine adjusted models were constructed in this fashion. Each of the adjusted models included a single marker, as well as clinical variables retained by backward selection with p value of less than 0.1. The candidate clinical variables included postinduction CVP, mitral or tricuspid valve surgery, diabetes, preoperative creatinine, right ventricular dysfunction and left ventricle ejection fraction. These variables were selected a priori based on their established association with AKI and RVF in cardiac surgical patients.16 17 Age and sex were not included in the models, as the cases and controls were already matched on those variables. The adjusted model for PAPi did not include CVP as PAPi and CVP are collinear.
Measures of association were OR and associated 95% CIs. Area under the curve (AUC) and associated 95% CIs were calculated for each of the models, as a measure of the model’s ability to distinguish cases from controls. Optimal cut-off points for the unadjusted models were determined by maximising Youden’s index.18 Any ties were broken by minimising the distance to the upper left corner.
Patient and public involvement
Patients and the public were not involved in the conduct of this research study.
Results
Baseline characteristics
We identified 85 cases and 85 controls from a total of 350 patients. The characteristics of patients who were cases and controls are presented in table 2. Of the cases, 18 developed c-AKI, 31 developed isolated AKI and 36 developed isolated RVF. Compared with the controls, patients who were cases had significantly higher baseline creatinine, postinduction CVP and PPP. They were also more likely to have diabetes, pre-existing RV dysfunction, and to undergo multiple valve reconstruction or concomitant CABG and valve surgery. Baseline IGFBP7 levels were also higher in the cases as compared with controls, which constituted the most significant preoperative differentiating characteristic between the two groups. Patients who were cases had significantly longer durations of hospital stay, intensive care unit stay and mechanical ventilation.
Patients’ characteristics for all cases (AKI, RVF and c-AKI) and all corresponding controls
Prediction of outcomes with biomarkers and haemodynamic data
The biomarker models for c-AKI had incorporated 18 case–control pairs, and the models for AKI and RVF had incorporated 49 and 51 pairs, respectively. There were fewer case–control pairs for the PAPi models, due to incomplete haemodynamic data (table 3).
Area under the receiver-operating curve (AUC), optimal cut-off points and associated sensitivity and specificity for all adjusted and non-adjusted models predicting c-AKI, AKI and RVF with IGFBP7, NT-pro-BNP and PAPi
Univariate models
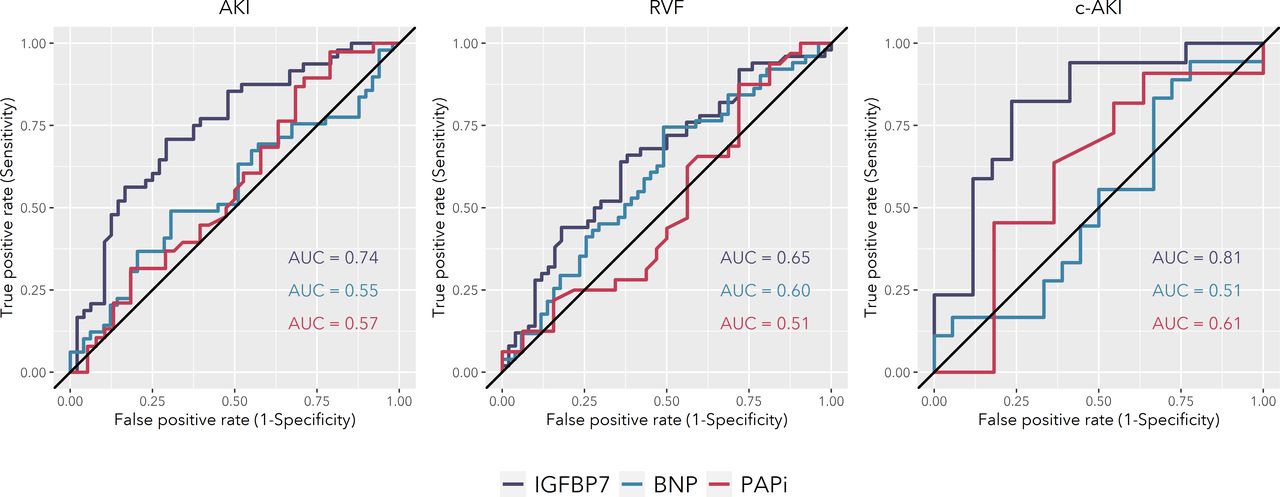
For each of the outcomes, IGFBP7 outperformed NT-pro-BNP and PAPi in the unadjusted analysis (table 3). For the prediction of c-AKI, the unadjusted AUC was 0.81 (95% CI 0.66 to 0.96) for IGFBP7, 0.51 (95% CI 0.31 to 0.71) for NT-pro-BNP and 0.61 (95% CI 0.36 to 0.87) for PAPi. For the prediction of AKI, the unadjusted AUCs were 0.74 (95% CI 0.64 to 0.85) for IGFBP7, 0.55 (95% CI 0.44 to 0.67) for NT-pro-BNP and 0.57 (95% CI 0.44 to 0.70) for PAPi (figure 1). Finally, the biomarkers were modest at best in their predictions of RVF, with unadjusted AUCs of 0.65 (95% CI 0.54 to 0.76) for IGFBP7, 0.60 (95% CI 0.49 to 0.71) for NT-pro-BNP and 0.51 (95% CI 0.36 to 0.65) for PAPi.

Receiver operating characteristic curves for unadjusted prediction models of AKI, RVF and c-AKI with IGFPB7, NT-pro-BNP and PAPi. AKI, acute kidney injury; AUC, area under the curve; c-AKI, congestive AKI; NT-pro-BNP, N-terminal prohormone B-type natriuretic peptide; PAPi, Pulmonary Artery Pulsatility Index; RVF, right ventricular failure.
The univariate ORs for each of the biomarkers and PAPi are presented in table 4. Univariate ORs for each increase of 10 ng/mL in IGFBP7 were 1.63 (95% CI 1.14 to 2.33) for c-AKI, 1.29 (95% CI 1.10 to 1.52) for AKI and 1.17 (95% CI 1.01 to 1.36) for RVF (table 4). The optimal cut-off value for prediction with IGFBP7 was 102 ng/mL for either AKI or c-AKI and 89.5 ng/mL for RVF. NT-pro-BNP and PAPi were not significantly associated with any of the outcomes.
ORs and associated p values for adjusted and non-adjusted logistic regression models predicting c-AKI, AKI and RVF with IGFBP7, NT-pro-BNP and PAPi
Multivariable models
For each of the outcomes, the adjusted NT-pro-BNP and IGFBP7 models had similar receiver operating curves (figure 2) and corresponding AUCs (table 3). For c-AKI, adjusted AUC was 0.90 (95% CI 0.81 to 1.00) for IGFBP7, 0.87 (95% CI 0.76 to 0.99) for NT-pro-BNP and 0.77 (95% CI 0.56 to 0.97) for PAPi. For isolated AKI, adjusted AUC was 0.79 (95% CI 0.67 to 0.88) for IGFBP7, 0.78 (95% CI 0.68 to 0.87) for NT-pro-BNP and 0.68 (95% CI 0.56 to 0.81) for PAPi. For RVF, adjusted AUC was 0.69 (95% CI 0.58 to 0.80) for IGFBP7, 0.74 (95% CI 0.64 to 0.83) for NT-pro-BNP and 0.69 (95% CI 0.56 to 0.82) for PAPi.

{kind=link}
{kind=link}
Receiver operating characteristic curves for adjusted prediction models of AKI, RVF and c-AKI with IGFPB7, NT-pro-BNP and PAPi. AKI, acute kidney injury; AUC, area under the curve; c-AKI, congestive AKI; NT-pro-BNP, N-terminal prohormone B-type natriuretic peptide; PAPi, Pulmonary Artery Pulsatility Index; RVF, right ventricular failure.
The adjusted ORs for each 10 ng/mL increase in IGFBP7 were 1.97 (95% CI 1.20 to 3.24) for c-AKI, 1.25 (95% CI 1.07 to 1.46) for AKI and 1.15 (95% CI 1.00 to 1.32) for RVF (table 4). Of note, there was no statistically significant association between NT-pro-BNP or PAPi and any of the outcomes after multivariable adjustment.
Online supplemental table S1 summarises the clinical predictors of c-AKI, AKI and RVF in each of the multivariable models. Diabetes was an independent predictor in most AKI and RVF models. Mitral and tricuspid valve surgery were independent predictors of c-AKI and AKI in the IGFBP7 and NT-pro-BNP models. Preoperative left ventricular ejection fraction was an independent predictor only for c-AKI, whereas baseline creatinine and RVF predicted postoperative RVF.
Supplemental material
Discussion
IGFBP7 outperformed NT-pro-BNP and PAPi as a predictor of c-AKI, AKI and RVF; and its predictive performance remained robust after multivariable adjustment. Our findings suggest that a single preoperative biomarker measurement could augment the clinician’s ability to identify high-risk patients for proactive optimisation, prevent important complications and improve patient outcomes.
Congestive acute kidney injury
Although c-AKI was only recently described in the literature, it has long been recognised as an end organ sequela of RVF with significant mortality, morbidity and healthcare resource use3. We found that IGFBP7 by itself had excellent ability to predict c-AKI after cardiac surgery (unadjusted AUC=0.81), whereas NT-pro-BNP or PAPi alone only exhibited modest discrimination. These findings corroborate previous work by Zelt et al,3 who reported modest AUCs for a variety of preoperative cardiorenal markers in the prediction of c-AKI (0.67 for NGAL, 0.74 for NT-pro-BNP, 0.67 for hs-TnT and 0.64 for CVP).
Acute kidney injury
We found that preoperative IGFBP7 predicts AKI with a moderate but marginally higher degree of accuracy (AUC=0.74) than previously reported for other markers (0.67 for NGAL, 0.70 for NT-pro-BNP, 0.68 for hs-cTNT and 0.60 for CVP).3 We also found that PAPi alone had limited predictive value for AKI, with an AUC of 0.57. Although the predictive accuracy of IGFBP7 remains to be confirmed by further studies, our reported AUC for NT-pro-BNP is corroborated by a contemporary multicentre trial. In this trial of 960 cardiac surgery patients, the AUC of NT-pro-BNP was 0.64 (0.56 to 0.72) and falls within the 95% CI of that reported in our study.19 The optimal cutoffs for classification were also similar, with a value of 459 pg/mL in our study compared with 504 pg/mL in the larger trial.19 These similarities are confirmatory and speak to the external validity to our findings.
The predictive performance of IGFBP7 also compares favourably with established clinical risk scores. The Cleveland Clinic Score, a validated clinical risk score for AKI after cardiac surgery, had an AUC of 0.72 (95% CI 0.62 to 0.82).20 An earlier clinical risk score by D'Onofrio et al had an AUC of 0.71.21 Thus, preoperative serum IGFBP7 could potentially be used to identify high-risk patients at the point-of-care, before detailed clinical information becomes available.
Right ventricular failure
Perioperative RVF is difficult to predict using traditional means, and existing modalities perform modestly at best.2 We reported an unadjusted AUC of 0.65 for IGFBP7, which outperforms NT-pro-BNP and PAPi in this study and is robust when compared with those reported in the literature. Zelt et al reported unadjusted AUCs of 0.57 for NT-pro-BNP, and between 0.54 and 0.70 for NGAL, hs-cTNT and CVP.3 Although the role of preoperative PAPi has been investigated in the heart failure and left ventricular assist device population, it has not been evaluated in patients undergoing routine cardiac surgery and thus no meaningful comparison could be made.22 To date, one small, single-centre study (N=119) evaluated the role of prebypass- and postbypass PAPi in early identification of cardiac surgery-related RVF,6 but the AUC of preoperative PAPi was not reported. Our findings suggest that IGFBP7 could be further evaluated as a non-invasive screening tool to identify cardiac surgery patients who are at risk for developing perioperative RVF.
The value of clinical variables
The addition of clinical variables led to higher multivariable AUCs as compared with the univariable biomarker or PAPi models. However, while IGFBP7 remained an independent predictor in each of the multivariable models, NT-pro-BNP and PAPi were not independent predictors in any of the models. Both the unadjusted and adjusted models have clinical relevance and their own advantages. An unadjusted model is simpler, requires no accompanying patient information and provides risk stratification at the point-of-care, whereas adjusted models offer higher predictive performance.
Clinical implications
Perioperative RVF is a challenging and deadly syndrome for which the best treatment is preventative rather than reactive.5 Given the importance of RV and renal function in patients’ perioperative and long-term survival, simple and effective risk stratification methods are needed to target the right patients for preventative therapy. Our findings introduce the possibility of integrating a single biomarker measurement as an empiric screen at the time of surgical referral, to identify patients who might benefit most from preoperative diuresis, as well as volume status optimisation, pre-emptive inotropic support and advanced haemodynamic and echocardiographic monitoring in the perioperative setting.
Limitations
Our study is limited by the small number of c-AKI cases, which may have subjected the multivariable models to overfitting. However, c-AKI is a rare complication and our source population (N=350) is relatively large in the realm of biomarker research. In addition, the single-centre nature of our study limits the generalisability of our findings and prompts confirmatory studies at other centres and healthcare jurisdictions. Finally, we could not include urine output in our definition for AKI as we did not collect this information. This could potentially have limited our ability to identify some cases of AKI. However, omitting urine output from the definition of AKI is not uncommon in the anaesthesiology literature.23–25
Conclusions
Preoperative serum IGFBP7 is a strong predictor of c-AKI and a good predictor of AKI and RVF after cardiac surgery, with AUCs comparable or higher than others reported in the literature. IGFBP7 may serve to augment the clinician’s gestalt in predicting these complications in cardiac surgery patients. Its predictive performance and cut-off values will need to be confirmed in larger observational studies prior to being used in interventional trials of c-AKI and RVF prevention in this population.
Data availability statement
Data are available on reasonable request. Data available on request due to restrictions. The data presented in this study are available on request from the corresponding author. The data are not publicly available due to privacy restrictions.
Ethics statements
Patient consent for publication
Ethics approval
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Institutional Review Board of the University of Ottawa Heart Institute (UOHI) (protocol #: 2015049401H and originally approved on 31 August 2015). Participants gave informed consent to participate in the study before taking part.
Acknowledgments
Biochemical assays were performed at the Cardiac Function Laboratory at the University of Ottawa Heart Institute. We would like to thank Dr. Liu, Director of the laboratory, for his support of this project.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @y_macmillan, @mmamas1973, @sunlouise1
Contributors Conceptualisation, LS; methodology, YM, LS; validation, YM, LS; formal analysis, YM, LS; investigation, YM, LS; resources, LS; data curation, LS; writing-original draft preparation, YM, LS; writing-review and editing, YM, MM, LS; visualisation, YM, MM, LS; supervision, LS; project administration, LS; funding acquisition, LS. All authors have read and agreed to the published version of the manuscript. LS: guarantor.
Funding This research was funded by an ORACLE Innovations Grant from the University of Ottawa Heart Institute (grant number 4529). The APC was funded by the University of Ottawa Department of Anesthesiology and Pain Medicine (grant number 4858). LS is supported by a Tier 2 Clinical Research Chair in Big Data and Cardiovascular Outcomes at the University of Ottawa and was named National new Investigator Award by the Heart and Stroke Foundation of Canada.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.