Article Text

Abstract
Objective This study aimed to evaluate the prognostic value of hyperemic microvascular resistance (HMR) and its relationship with hyperemic stenosis resistance (HSR) index and fractional flow reserve (FFR) in stable coronary artery disease.
Methods This is a substudy of the DEFINE-FLOW cohort (NCT02328820), which evaluated the prognosis of lesions (n=456) after combined FFR and coronary flow reserve (CFR) assessment in a prospective, non-blinded, non-randomised, multicentre study in 12 centres in Europe and Japan. Participants (n=430) were evaluated by wire-based measurement of coronary pressure, flow and vascular resistance (ComboWire XT, Phillips Volcano, San Diego, California, USA).
Results Mean FFR and CFR were 0.82±0.10 and 2.2±0.6, respectively. When divided according to FFR and CFR thresholds (above and below 0.80 and 2.0, respectively), HMR was highest in lesions with FFR>0.80 and CFR<2.0 (n=99) compared with lesions with FFR≤0.80 and CFR≥2.0 (n=68) (2.92±1.2 vs 1.91±0.64 mm Hg/cm/s, p<0.001). The FFR value was proportional to the ratio between HMR and the HMR+HSR (total resistance), 95% limits of agreement (−0.032; 0.019), bias (−0.003±0.02) and correlation (r2=0.98, p<0.0001). Cox regression model using HMR as continuous parameter for target vessel failure showed an HR of 1.51, 95% CI (0.9 to 2.4), p=0.10.
Conclusions Increased HMR was not associated with a higher rate of adverse clinical events, in this population of mainly stable patients. FFR can be equally well expressed as HMR/HMR+HSR, thereby providing an alternative conceptual formulation linking epicardial severity with microvascular resistance.
Trial registration number NCT02328820.
- coronary artery disease
- coronary vessels
- microvascular angina
Data availability statement
Data are available in a public, open access repository. https://datadryad.org/stash/dataset/doi:10.5061/dryad.h18931zm6.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known about this subject?
Fractional flow reserve (FFR) and hyperemic microvascular (HMR) is assumed to reflect the epicardial and microvascular disease, respectively. Impaired microcirculation is associated with worse outcome following acute coronary syndromes.
What does this study add?
FFR is closely related to microvascular resistance and can mathematically be expressed as HMR/HMR+hyperemic stenosis resistance index. Increased HMR is not associated with poor outcome in stable coronary lesions.
How might this impact on clinical practice?
Evaluation of the microcirculation should be integrated in assessment of coronary artery disease as it potentially confounds the FFR value. However, there is no prognostic value of increased microvascular resistance in stable coronary lesions.
Introduction
Fractional flow reserve (FFR) is calculated as the ratio between the mean distal coronary artery pressure (Pd) and the mean aortic pressure (Pa) during hyperemia.1 Administration of intracoronary nitrates ensures relaxation of the epicardial arteries and adenosine dilates the microcirculation and generates the hyperemic pressure gradient across an epicardial stenosis. Microcirculatory dysfunction impairs hyperemia and thus increases the hyperemic pressure ratio, potentially altering the treatment decision. Conceptually, preserved FFR and low coronary flow reserve (CFR) indicate either increased hyperemic microvascular resistance (HMR) or in a setting of normal microvascular resistance a high resting myocardial flow.2 Conversely, reduced microvascular resistance produces lower FFR values for the same stenosis geometry.
A continuous relationship exists between FFR and major adverse cardiac events (MACEs) both before and after revascularisation, with lower FFR values associated with poorer outcomes. Interestingly, even FFR values right above the threshold (ie, 0.80–0.90) associate with an increased rate of revascularisation during follow-up.3 The net effect of coronary disease arises from both epicardial and microvascular components. CFR assesses both,4 and low CFR, especially in combination with low FFR, associates with adverse cardiovascular outcomes.5 6 HMR conceptually distinguishes between low FFR lesions with concordant low CFR (higher resistance) and with discordant intact CFR (lower resistance).3 Increased microvascular resistance has prognostic value following primary percutaneous coronary interventions (PCIs)7 and immediately after PCI in stable patients with ischaemic heart disease.8
This manuscript presents a substudy of Distal Evaluation of Functional performance with Intravascular sensors to assess the Narrowing Effect—combined pressure and Doppler FLOW velocity measurements—DEFINE-FLOW (NCT02328820), an international clinical trial with 12 participating centres in Europe and Japan.9 The primary purpose of the trial was to evaluate the prognostic value of combined FFR and CFR assessment by deferring PCI in the lesions with normal CFR (≥2.0) despite reduced FFR (≤0.80). This substudy aims to (1) evaluate the prognostic value of HMR in stable coronary artery disease and (2) investigate the link between the microcirculation and epicardial pressure gradients and, thereby, between HMR and FFR according to the CFR level.
Methods
Study subjects
The design of the DEFINE-FLOW (clinicaltrials.gov NCT02328820) study has been published previously.10 Data generated by the authors are available in a public, open access repository.11 Combined pressure and Doppler sensors (on a single 0.014″ wire) measured pressure and flow in all subjects. The main inclusion criteria were patients with ischaemic heart disease eligible for PCI, diameter stenosis ≥50%, and reference diameter ≥2.5 mm. The main exclusion criteria were prior coronary artery bypass graft surgery, left main disease, vessel tortuosity, severe left ventricular hypertrophy, contraindication to adenosine infusion, recent (within 3 weeks) ST-elevation myocardial infarction, culprit lesion in non-ST-elevation myocardial infarction and life expectancy less than 24 months. The results of the main study have been published.9
Patient and public involvement
Patients or the public were not involved in the design, conduct, reporting of the study, or dissemination plans of our research.
Ethics approval
The study was conducted according to the Helsinki Declaration following approval of local ethical committees/institutional review boards at all participating sites (Denmark: Aarhus, Italy: Rome, Japan: Gifu, Toda, Tokyo, Tsuchiura, Netherlands: Amsterdam AMC, Blaricu, Breda, Spain: Madrid, UK: London).
Invasive haemodynamic measurements and clinical decision making for revascularisation
In lesions suitable for PCI, flow and pressure were measured using the ComboWire XT (Phillips Volcano, San Diego, California, USA). For hyperemic measurement, 100 µg (or 60 µg if limited by arrhythmia) intracoronary adenosine was administered for two consecutive values12 after placing the wire as distally as possible. All flow and pressure curves were independently and centrally analysed at a blinded core lab (University Medical Centers, location Academic Medical Center, Amsterdam, Netherlands). PCI was performed only in lesions with combined FFR≤0.80 and CFR<2.0 and deferred in discordant and concordant negative combinations.
Statistics
HMR was defined as the ratio between the distal coronary pressure (Pd) and maximal coronary flow velocity during hyperemia. Hyperemic stenosis resistance (HSR) was defined as the ratio between the pressure gradient across the lesion (Pa−Pd) and maximal coronary flow velocity during hyperemia. Data were stratified according binary FFR/CFR thresholds into four groups: FFR>0.80 and CFR≥2.0, FFR≤0.80 and CFR≥2.0, FFR≤0.80 and CFR<2.0, FFR>0.80 and CFR<2.0. FFR is defined as Pd(h)/Pa(h), HMR=Pd(h)/Q(h) and HSR=[Pa(h)−Pd(h)]/Q(h), where Pd(h), Pa(h) and Q(h) represent the mean distal coronary pressure, mean aortic pressure and the average peak velocity during maximal hyperemia, respectively. Additional relationships can be derived as follows:



Straightforward manipulation shows that FFR=HMR/(HMR+HSR) or, alternatively, that 1/FFR=1+HSR/HMR. The first equation is equivalent to Ohm’s law for two resistors in series, corresponding to sequential epicardial and microvascular resistances.
Continuous variables are presented as mean±SD and categorical variables as number (%). The relationship between 1/FFR and HSR/HMR was investigated using linear regression analysis. Parameters were analysed per vessel using generalised estimating equations with pairwise analysis and Bonferroni adjustment for clustering. Lesions were classified according to a binary HMR threshold (2.5 mm Hg/cm/s) derived from a previous study13 and composite primary endpoint major adverse cardiovascular events were evaluated with a Kaplan-Meier survival curve in lesions that were not revascularised at the index procedure. In unrevascularised vessels, HMR was evaluated as a continuous variable to predict target vessel failure after adjustment for CFR and FFR using a Cox proportional hazards regression model accounting for multiple lesions per patient. Analysis was conducted in R V.4.0.5 (R Foundation for Statistical Computing, Vienna, Austria) and SPSS V.17 (IBM, USA).
Results
Baseline characteristics
Tables 1 and 2 show population demographics and lesion/vessel characteristics. Mean age was 67 years and 74% of the population was men; 344 (80%) presented with stable ischaemic heart disease and 86 (20%) with non-ST elevation myocardial infarction. The majority of lesions were located in the left anterior descending artery (LAD) 314 (59%) and a majority of patients received aspirin and statin therapy (table 1). In total n=430 patients and n=533 lesions were included for physiological evaluation, of which data from n=456 lesions passed core-lab quality for analysis (table 2).
Demographics
Vessel-level haemodynamic and anatomic data
Overall and stratified invasive haemodynamic data
Mean FFR and CFR values were 0.82±0.10 and 2.2±0.6, respectively (table 2). HMR varied among the four quadrants by binary FFR=0.80 and CFR=2.0 (table 3): 2.4±0.89 (FFR>0.80 and CFR≥2.0), 2.53±0.93 (FFR≤0.80 and CFR<2.0), 1.91±0.64 (FFR≤0.80 but CFR≥2.0) and 2.92±1.2 (FFR>0.80 but CFR<2.0), all units of mm Hg/cm/s and p<0.001. High HMR was associated with higher age (69 vs 65 years), higher FFR (0.83±0.1 vs 0.81±0.1) and highest proportion of hypertensives (61% vs 37%) (table 4). All haemodynamic values (except baseline average peak velocity) improved following PCI (table 5).
Haemodynamic data according to FFR and CFR levels
HMR-level and haemodynamic characteristics
Pre and post-PCI
Clinical outcomes according to HMR-level
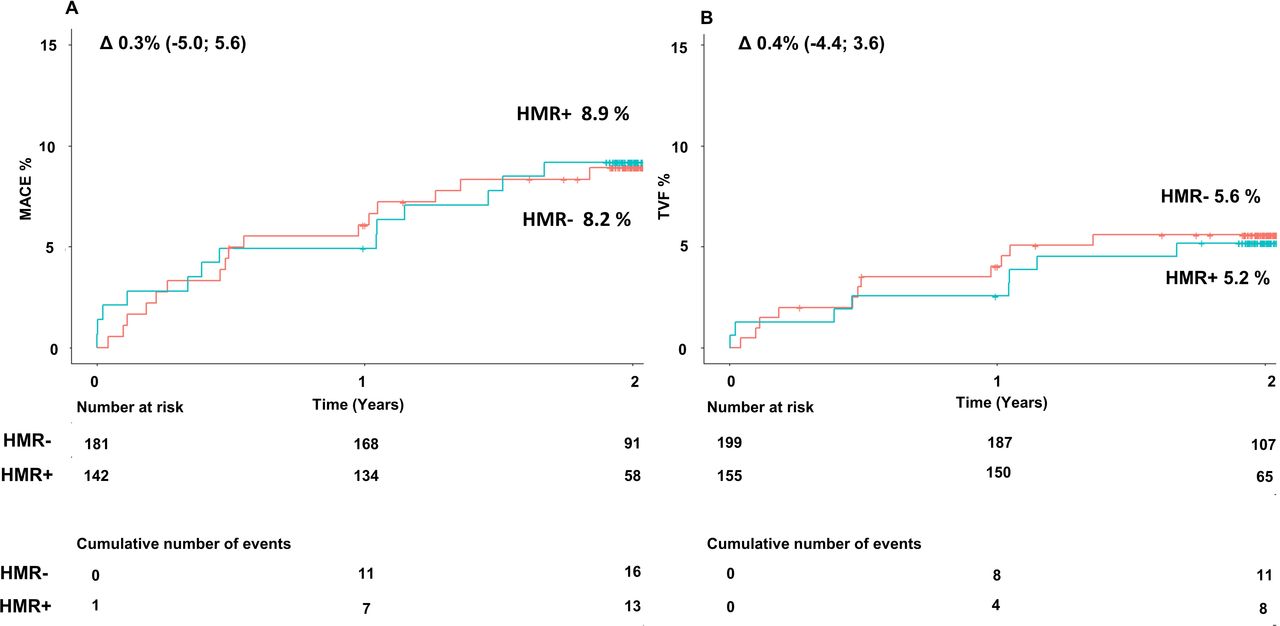
Kaplan-Meier curves of cumulative MACEs and target vessel failure (TVF) demonstrated no significant differences for medically treated lesions when using an HMR threshold of 2.5 mm Hg/cm/s: MACE: ∆ 0.3%, 95% CI (−5.0 to 5.6) and TVF: ∆ 0.4%, 95% CI (−4.4 to 3.6) (figure 1). Cox regression modelling of HMR as a continuous parameter demonstrated an HR of 1.51 (IQR 0.9 to 2.4), p=0.10, for target vessel failure for per 1 mm Hg/cm/s increase in HMR (figure 2).

Kaplan-Meier survival curve of (A) major adverse cardiovascular events (MACE) and (B) target vessel failure (TVF) in lesions with high versus low hyperemic microvascular resistance (HMR+ vs HMR−, using threshold 2.5 mm Hg/cm/s) and treated medically. There was no significant differences in the event rate.

Cox regression model of estimated target vessel failure (TVF) in medically treated vessels when adjusted for FFR and CFR after accounting for multiple lesions per patient. HR per 1 mm Hg/cm/s increase in HMR. CFR, coronary flow reserve; FFR, fractional flow reserve; HMR, hyperemic microvascular resistance.
The relationship between FFR and HSR/HMR
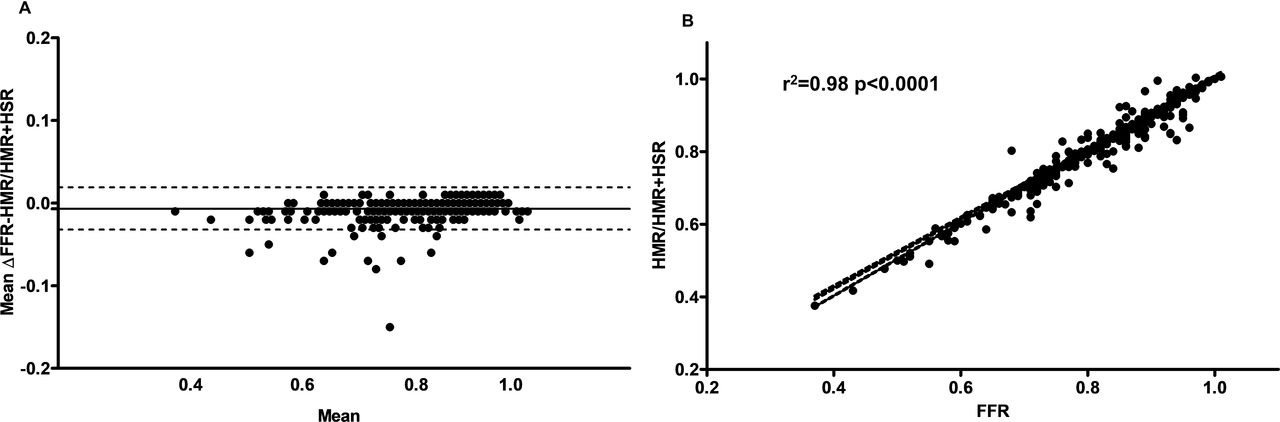
FFR was closely related to the ratio HMR/(HMR+HSR) with r2=0.98, slope 0.95±0.005, p<0.0001; the Bland-Altman plot showed a low bias (−0.003±0.02, figure 3). The highest and lowest HMR was observed in the reverse discordant group with FFR>0.80 and CFR<2.0 and in the discordant group with FFR≤0.80 and CFR≥2.0, respectively (figure 4). Likewise the highest and lowest HSR was observed in the concordant abnormal group with FFR≤0.80 and CFR<2.0 and in the concordant normal group with FFR>0.80 and CFR≥2.0 (table 3).
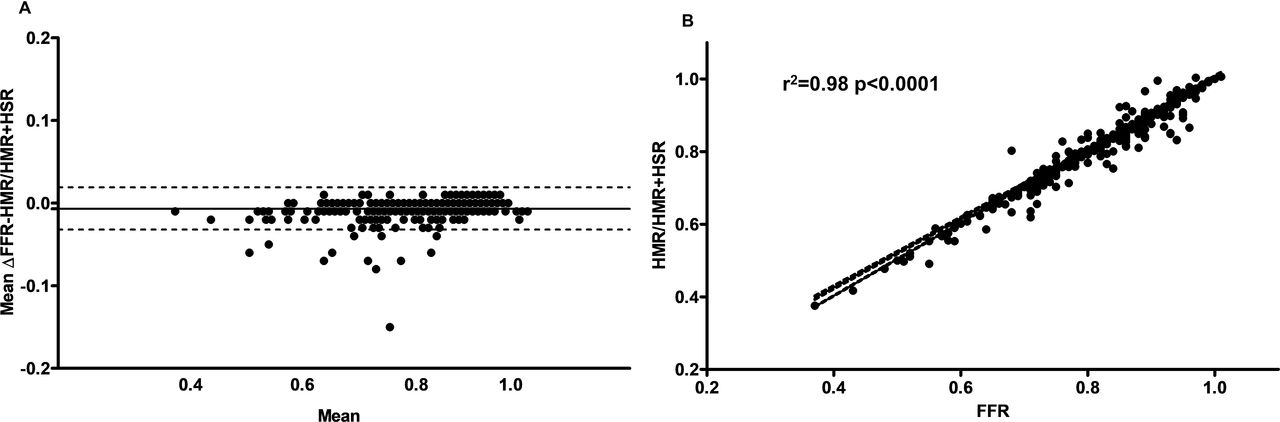
The novel relationship between fractional flow reserve (FFR) and hyperemic microvascular resistance (HMR) and hyperemic stenotic resistance (HSR). (A) Bland-Altman plot of the mean difference between HMR–HSR and the mean value. Bias −0.003±0.02. The dotted line indicates the 95% CI. (B) Linear correlation between HMR/HMR+HSR and FFR, r2=0.98, p<0.0001.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
FFR and HMR, according to FFR/CFR concordance. The dotted line indicates HMR median=2.23 mm Hg/cm/s and FFR=0.80. HMR is highest in the reverse discordant group with FFR>0.80 and CFR<2.0 and lowest HMR in the discordant group with FFR≤0.80 and CFR≥2.0. CFR, coronary flow reserve; FFR, fractional flow reserve; HMR, hyperemic microvascular resistance.
Discussion
The main results of this study were (1) increased HMR did not associate with an increase in clinical events. (2) A basic haemodynamic relationship exists between FFR and microvascular resistance, namely (HMR/HMR+HSR); (3) HMR is concordantly associated with the FFR classification and pronounced in lesions with combined low CFR and high FFR.
Guidelines recommend physiological assessment of moderate coronary artery disease prior to intervention.14 Although deferring PCI given FFR>0.80 is associated with a good overall prognosis,15 the presence of FFR above the threshold does not necessarily indicate completely normal haemodynamic conditions in the investigated coronary territory. Increased microvascular resistance impairs the hyperemic pressure drop across an epicardial lesion and is thereby associated with higher FFR values,16 although correct for the current state of the microvasculature. Untreated lesions with combined FFR≤0.80 and CFR<2.0 are associated with the least favourable outcomes.6 Increased index of microvascular resistance can be observed in lesions with FFR>0.80.17 Hence, high resistance in the microvascular bed can occur in the setting of reversible perfusion defects as assessed by myocardial perfusion scintigraphy.18 Consequently, HMR plays a proportionally larger role than HSR in FFR for most moderate lesions (50%–90%), whereas in severe lesions the collaterals confound the apparent HMR value unless corrected for the coronary wedge pressure.
Microvascular resistance and the vasodilatory reserve are significant determinants of FFR, highlighted by the close relation between FFR and the ratio between HMR and total vascular resistance (HMR+HSR). In lesions with low FFR and normal CFR, the low FFR is driven by a low HMR, enhancing the pressure gradient across the epicardial stenosis.19 Because pressure gradients depend on absolute flow, which is proportional to distal myocardial mass, lower FFR can be observed in LAD versus non-LAD lesions20–22 even for the same perfusion (flow normalised to distal myocardial mass). Because HMR does not explicitly adjust for the amount of distal myocardium, some of the difference between LAD and non-LAD findings may simply reflect the larger typical mass supplied by the LAD.23 Relatedly, FFR associates with the amount of viable myocardium, hence vascular resistance can be higher in non-viable myocardium and generate a higher FFR.24 25 This association was negligible in the current study, as the average left ventricular ejection fraction was normal.
Under steady-state physiological conditions, the main pressure drop occurs in the microcirculation, and the epicardial arteries function as conduit vessels.26 In coronary artery disease, epicardial stenoses increase the total vascular resistance. Thus, in conditions with abnormal microcirculation (eg, hypertension, chronic kidney disease, diabetes, aortic stenosis, left ventricular hypertrophy), the FFR value may be higher compared with a state of healthy microcirculation, leading to deferral of revascularisation for an FFR value around the 0.80 threshold. However, we could not demonstrate a significant association between poor outcome and high HMR in our substudy. Increased microvascular resistance measured as HMR and index of microcirculatory resistance are predictors clinical outcome following primary PCI and acute and chronic coronary syndromes.7 8 It contrasts with the results of this current study for several reasons. First, the prognostic value of microvascular resistance was related to the post-PCI FFR. In chronic coronary syndromes PCI improves the epicardial hemodynamics and decreases microvascular resistance,27 confirming the current results. Thus, post-PCI microvascular resistance partly reflects the PCI result, like the prognostic value of the post-PCI FFR.28 After revascularisation FFR, CFR, HSR and HMR was only assessed in relatively few cases, making it impossible to evaluate the prognostic value of post-PCI HMR. Second, PCI was deferred in lesions with FFR<0.80 and CFR≥2.0, which in clinical circumstances could have mandated PCI. Third, a high microvascular resistance reflects myocardial injury and infarction size in patients with acute ST-elevation myocardial infarction,29 hence its prognostic value in that different scenario; in stable patients the microvascular resistance is multifactorial and reflects underlying risk factors like hypertension and age that cause microvascular remodelling.30 Finally, the clinical outcome results of low versus high HMR, reflect the benign nature of chronic coronary syndromes in this population without left main and three vessel disease and therefore few events.
Limitations
For severe coronary lesions, collateral blood flow contributes to an increasingly substantial amount of myocardial supply. Because we did not record coronary wedge pressures systematically, we only report apparent HMR and not adjusted for collateral flow in cases of severe epicardial stenosis.
Conclusions
Increased HMR is not associated with increased event rate in stable coronary artery disease. FFR is related to stenosis and microvascular resistance via the equation HMR/HMR+HSR. Further randomised studies are needed to evaluate the clinical relevance of these findings.
Data availability statement
Data are available in a public, open access repository. https://datadryad.org/stash/dataset/doi:10.5061/dryad.h18931zm6.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by the respective EC/IRB in all the respective countries that participated. Participants gave informed consent to participate in the study before taking part.
References
Footnotes
Contributors AE drafted the manuscript. AE and JW contributed to data analysis. AE, NJ, RLK, EHC contributed to study design. All authors contributed to the data collection, revision and editing of the manuscript. AE, JW, EHC, NRH are responsible for the overall content as guarantors.
Funding Funds from Philips Volcano Corporation supported this study.
Competing interests JJP has been consultant for Philips. RLK and NJ and KLG received internal funding from the Weatherhead PET center for Preventing and reversing Atherosclerosis. NJ has an institutional licensing and consulting agreement with Boston Scientific for the smart minimum FFR algorithm; and received significant institutional research support from St. Jude Medical (CONTRAST, NCT02184117) for a different study using intracoronary pressure sensors. NJ received significant institutional research support from Philips/Volcano Corporation for this study. EHC received institutional research support from Philips/Volcano Corporation for this study.
Provenance and peer review Not commissioned; externally peer reviewed.