Article Text

Abstract
Background Hepatocyte growth factor (HGF) is a biomarker with potential for use in the diagnosis, treatment and prognostication of cardiovascular disease (CVD). Elevated HGF is associated with calcification in the coronary arteries. However, knowledge is limited on the role HGF may play in extracoronary calcification (ECC). This study examined whether HGF is associated with ECC in the aortic valve (AVC), mitral annulus (MAC), ascending thoracic aorta and descending thoracic aortic (DTAC).
Methods At baseline, adults aged 45–84 years, free of CVD, in the Multi-Ethnic Study of Atherosclerosis had HGF and ECC measured by ELISA and cardiac CT scan, respectively. ECC measurements were repeated after an average of 2.4 years of follow-up. Prevalent ECC was defined as Agatston score >0 at baseline. Incident ECC was defined as Agatston score >0 at follow-up among participants with Agatston score=0 at baseline. We used Poisson and linear mixed-effects regression models to estimate the association between HGF and ECC, adjusted for sociodemographic and CVD risk factors.
Results Of 6648 participants, 53% were women. Mean (SD) age was 62 (10) years. Median (IQR) of HGF was 905 (757-1087) pg/mL. After adjustment for CVD risk factors, the highest HGF levels (tertile 3) were associated with greater prevalence and extent of AVC, MAC and DTAC at baseline compared with the lowest tertile (tertile 1). Additionally, the risk of incident AVC and MAC increased by 62% and 45%, respectively, in demographic-adjusted models. However, the associations were not statistically significant in fully adjusted models. The highest HGF levels were also associated with 10% and 13% increase in MAC and DTAC progression, respectively, even after adjustment for CVD risk factors.
Conclusion Higher HGF levels were significantly associated with a greater risk of calcification at some extracoronary sites, suggesting an alternate biological pathway that could be targeted to reduce CVD risk.
- Atherosclerosis
- Biomarkers
- Cardiac Imaging Techniques
- Epidemiology
- Heart Valve Diseases
Data availability statement
The data for this study are not publicly available but may be obtained from a third party by submitting a proposal through NIH BioLINCC at https://biolincc.nhlbi.nih.gov/studies/mesa/.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Elevated hepatocyte growth factor is associated with calcification in the coronary arteries. However, it remains unclear whether hepatocyte growth factor increases the risk of calcification at extracoronary sites.
WHAT THIS STUDY ADDS
In a large multiethnic community-based cohort, higher levels of hepatocyte growth factor were significantly associated with a greater risk of calcification at multiple extracoronary sites.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Hepatocyte growth factor may represent an alternate biological pathway that could be targeted to reduce the burden of cardiovascular disease.
Introduction
Hepatocyte growth factor (HGF) is a novel biomarker with the potential for use in the diagnosis, treatment, prognostication and prevention of cardiovascular disease (CVD).1–3 It is a derivative of mesenchymal cells with multiple cardioprotective functions such as the regulation of cell growth, cell motility and cell morphogenesis, in addition to its antiapoptotic, antifibrotic, anti-inflammatory and angiogenic properties.2–5 HGF may be a useful biomarker of clinical and subclinical CVD, in part because it is released on damage to cardiac and vascular endothelial cells.2 3 Prior research that examined the association of circulating HGF with subclinical and clinical CVD found that higher HGF levels were associated with greater progression of atherosclerosis measured by coronary artery calcification (CAC) and carotid plaque.6 Additionally, higher HGF levels were associated with an increased risk of incident coronary heart disease (CHD), stroke, heart failure and poor cardiovascular health.7–10
However, it is unknown whether higher HGF levels are associated with an increase in the risk of extracoronary calcification (ECC) measured in the aortic valve (AVC), mitral annulus (MAC), ascending thoracic aorta (ATAC) and descending thoracic aorta (DTAC) . While CAC and ECC share many risk factors in common, these risk factors do not necessarily overlap across vascular beds. In addition, calcification in multiple extracoronary sites is associated with an increased risk for CHD and mortality.11 12 Therefore, further research is needed to understand factors that drive atherosclerosis in different vascular beds. This study aims to test the hypothesis that study participants with higher HGF levels would be more likely to have a higher prevalence and incidence of ECC as well as greater extent and progression of ECC, regardless of sex or race/ethnicity.
Methods
Study population
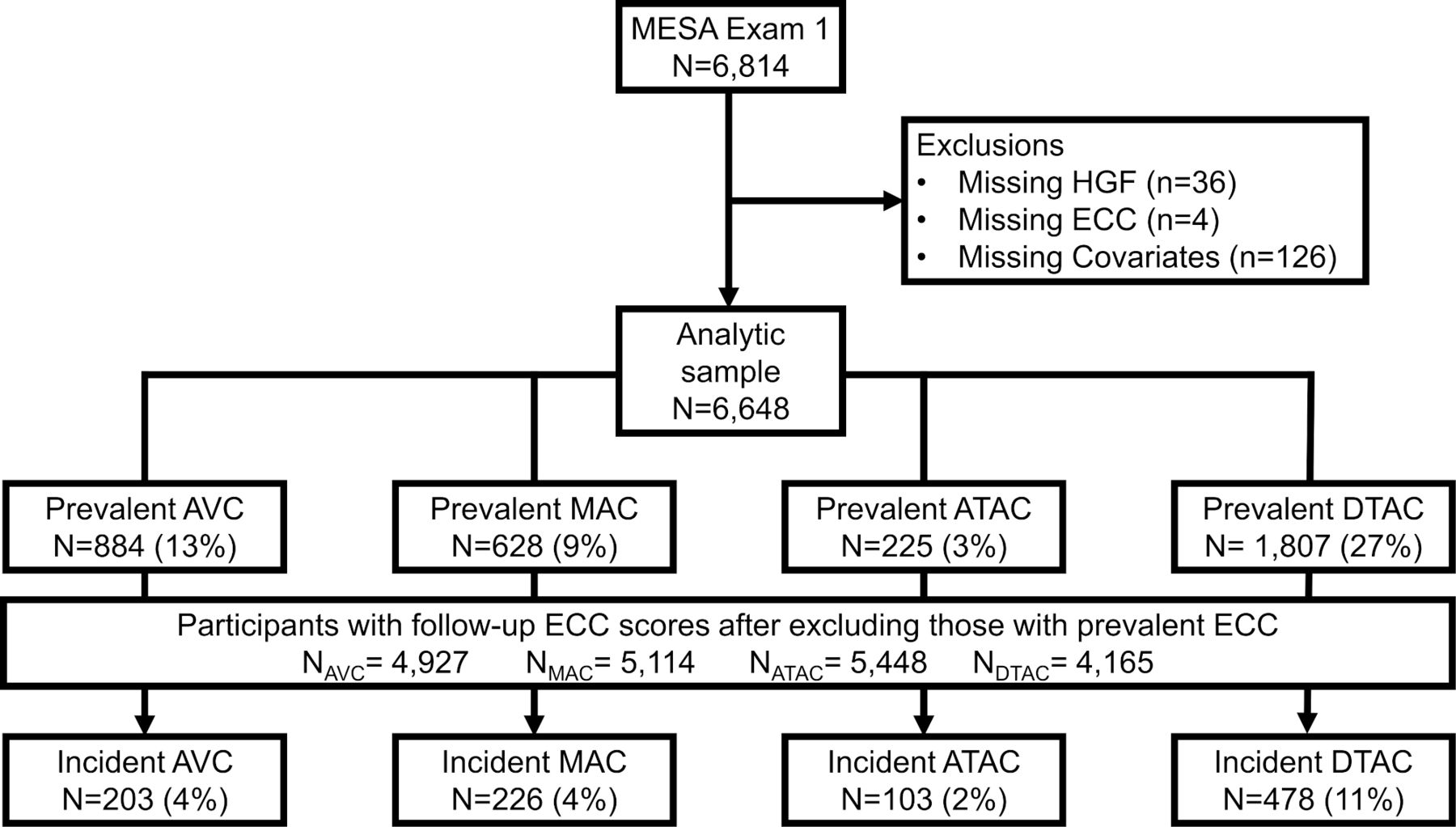
The Multi-Ethnic Study of Atherosclerosis (MESA) is a prospective cohort study designed to investigate the prevalence, correlates and progression of subclinical CVD.13 From 2000 to 2002, MESA recruited 6814 participants aged 45–84 years free of clinically recognised CVD from populations near six field centres in Baltimore, Maryland; Chicago, Illinois; Forsyth County, North Carolina; Los Angeles, California; New York, New York and St Paul, Minnesota. The study participants were non-Hispanic White (38%), Chinese-American (12%), non-Hispanic Black (28%) and Hispanic (22%) adults. The Institutional Review Boards of the participating field centres approved MESA and its ancillary studies. All recruited study participants gave written informed consent. The final analytical sample used for this study was 6648 after excluding participants with missing observations for the variables of interest (figure 1).
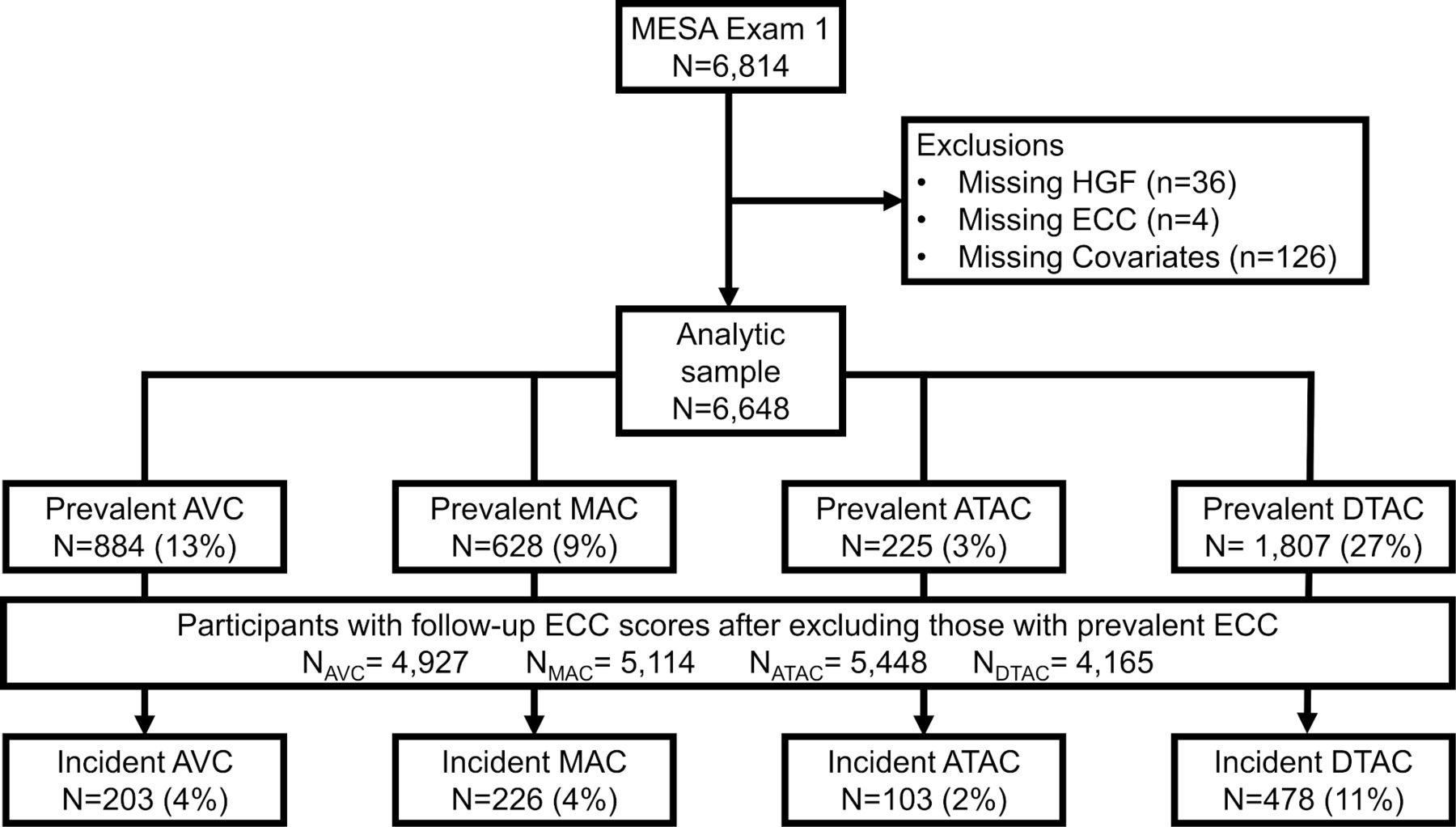
Flowchart of study participants. ATAC, ascending thoracic aorta; AVC, aortic valve; DTAC, descending thoracic aortic; ECC, extracoronary calcification; HGF, hepatocyte growth factor; MAC, mitral annulus; MESA, Multi-Ethnic Study of Atherosclerosis.
Exposure: HGF
To measure serum HGF, venous blood was obtained from fasting participants during the baseline examination. Serum separation was completed within 30 minutes of phlebotomy and aliquots were stored at −70°C.6 A quantitative sandwich ELISA with the Human soluble HGF/CD62P Immunoassay kit (R&D Systems, Minneapolis, Minnesota) was used to measure serum HGF protein. This methodology was validated by R&D systems, as specified in the package insert and verified by the laboratory at the University of Minnesota that measured HGF for this study. The lower limit of detection was 40 pg/mL.6 14 The interassay laboratory coefficients of variation were 12.0%, 8.0% and 7.4% at respective mean concentrations of 687 pg/mL, 2039 pg/mL and 4080 pg/mL for lyophilised manufacturer’s controls,6 14 and 10.4% at a mean concentration of 688 pg/mL for an in-house pooled serum control.6 14
Outcome: ECC
The details of the MESA cardiac CT protocol have been previously described.15 Between 2000 and 2002, two consecutive baseline non-contrast cardiac CT scans that were ECG gated to the R–R interval were obtained from each study participant.15 The Imatron C-150XL electron-beam CT scanner (GE-Imatron, San Francisco, California) was used at three field centres while the four slice-multidetector row CT scanner was used at the three other centres.15 High concordance has been reported between both CT scanner types with a kappa statistic of 0.94–0.96.16 17 After an average of 2.4 years, study participants were randomly assigned for a follow-up CT scan at either examination 2 (2002–2004) or examination 3 (2004–2005). The Agatston scoring method18 was used to quantify the presence of calcification at four extracoronary sites, namely (1) AVC to just before the aortic root, (2) level of the MAC, (3) ATAC and (4) DTAC.
Covariates
The covariates included in this study were assessed as continuous or categorical variables. We assessed age, body mass index (BMI), physical activity, pack-years of smoking, systolic blood pressure, total cholesterol, high-density lipoprotein cholesterol (HDL-C) and estimated glomerular filtration rate (eGFR) as continuous variables while sex, race/ethnicity, MESA field centre, health insurance, education, smoking, diabetes, use of antihypertensive and use of lipid-lowering medication were assessed as categorical variables.
BMI was calculated as weight over height squared (kg/m2). Physical activity was measured in metabolic equivalent of task-minute/week (MET-min/week) from the total minutes of moderate and vigorous exercise. Systolic blood pressure was measured three times in a seated position and the mean of the last two measurements was used in the analyses. Fasting blood samples were collected to measure total cholesterol and HDL-C. eGFR was calculated from serum concentrations of creatinine and cystatin C measured at baseline using the Chronic Kidney Disease Epidemiology Collaboration equation.19
Health insurance status was categorised as participants with or without health insurance. Education was dichotomised as ≥Bachelor’s degree and <Bachelor’s degree. Smoking status had three categories: never, former and current. Diabetes was defined using criteria from the American Diabetes Association.20
Statistical analyses
We performed all analyses using STATA statistical software V.15.0 and considered a p value <0.05 under a two-tailed test as statistically significant. Baseline characteristics of study participants were grouped by HGF tertiles. We reported frequencies with percentages for categorical variables and means with SD or medians with IQR for continuous variables. We used the χ2 and analysis of variance tests to compare baseline characteristics by the HGF tertiles for categorical and continuous variables, respectively.
Prevalent ECC was defined as Agatston score >0 at the baseline scan. Incident ECC was defined as Agatston score >0 at the follow-up scan among participants with Agatston score=0 at the baseline scan. We examined the associations of HGF (categorised into three tertiles) with prevalent and incident ECC (each of the four measures separately) using Poisson regression models with robust variance estimation. Estimates were presented with the corresponding 95% CIs. The models were progressively adjusted as follows: model 1 was adjusted for basic demographics: age, race/ethnicity, sex and field centre. Model 2 was adjusted for covariates in model 1 in addition to education, physical activity, smoking status, pack-years of smoking, BMI and health insurance. Model 3 was adjusted for covariates in models 1 and 2 along with total cholesterol, HDL-C, use of lipid-lowering medication, systolic blood pressure, use of antihypertensive medication, diabetes mellitus and eGFR.
The four measures of ECC were also modelled as continuous variables on the raw scale in Agatston units and logarithmically transformed for analysis. We used a linear mixed-effects regression model to estimate the associations of HGF with ECC extent at baseline and progression at 2 years. The linear mixed-effects regression model jointly examines cross-sectional and longitudinal effects of covariates on ECC, while also considering participant-specific random slopes and intercepts. The three adjusted models fitted for this analysis were similar to the aforementioned models for the Poisson regression. The distribution of prevalent and incident ECC by HGF tertiles were presented as figures. We tested for the interaction of HGF with sex and race/ethnicity by including cross-product terms in the fully adjusted models. Stratified analysis by subgroups was conducted where interaction was statistically significant.
Results
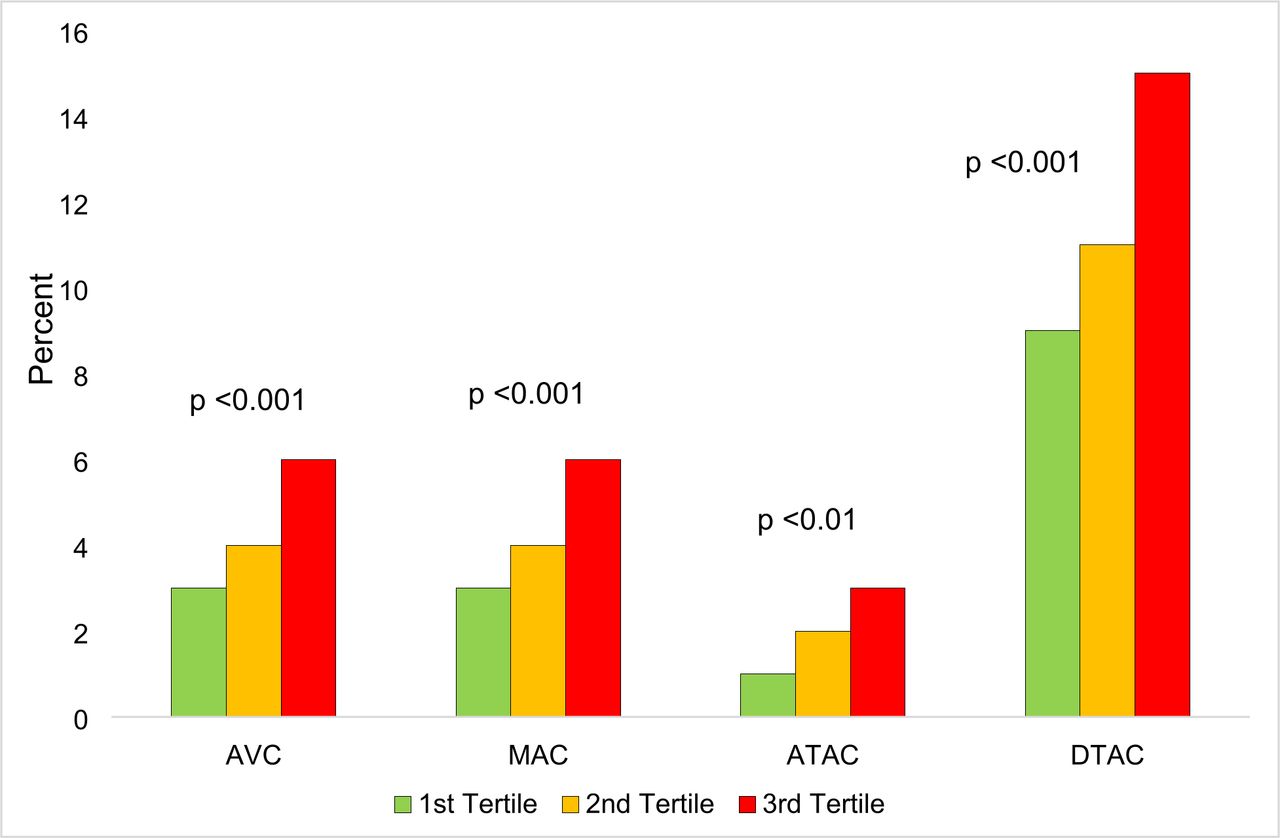
The mean age (SD) of MESA participants at baseline was 62 (10) years and 53% were women. A review of baseline characteristics showed that sociodemographic factors, CVD risk factors and ECC differed by HGF tertiles except for health insurance status. Mean baseline ECC scores were higher across increasing HGF tertiles (table 1). The counts with percentages of participants with prevalent and incident calcification at the four extracoronary sites are shown in figure 1. The distributions of prevalent and incident ECC by HGF tertiles are shown in figures 2 and 3, respectively.

Distribution of prevalent ECC by HGF tertiles. Green: first tertile of HGF; orange: second tertile of HGF; red: third tertile of HGF. ATAC, ascending thoracic aorta; AVC, aortic valve; DTAC, descending thoracic aortic; ECC, extracoronary calcification; HGF, hepatocyte growth factor; MAC, mitral annulus.

{kind=link}
{kind=link}
{kind=link}
Distribution of incident ECC by HGF tertiles. Green: first tertile of HGF; orange: second tertile of HGF; red: third tertile of HGF. ATAC, ascending thoracic aorta; AVC, aortic valve; DTAC, descending thoracic aortic; ECC, extracoronary calcification; HGF, hepatocyte growth factor; MAC, mitral annulus.
Characteristics of study participants by HGF tertiles
Cross-sectional analyses
Table 2 shows the cross-sectional association between HGF and prevalent ECC at baseline (ie, ECC scores >0). After adjustment for demographics (model 1), the highest HGF levels (tertile 3) were associated with a greater likelihood of having prevalent ECC for all four measures, with 50% (26%, 78%), 80% (44%, 125%), 84% (26%, 169%) and 28% (16%, 41%) higher prevalence of AVC, MAC, ATAC and DTAC, respectively. Although the prevalence ratios were attenuated, the association of HGF with the prevalence of these ECC measures remained statistically significant after full adjustment for CVD risk factors (model 3) except for ATAC. Table 3 shows the association between HGF and ECC extent at baseline (log-transformed ECC +1). Likewise, we found HGF levels in the highest tertile were associated with a greater extent of all four ECC measures at baseline. After adjustment for demographics (model 1), HGF was associated with 28% (18%, 40%), 32% (22%, 44%), 9% (4%, 15%) and 56% (36%, 79%) greater extent of AVC, MAC, ATAC and DTAC, respectively. After full adjustment for CVD risk factors (model 3), the association of HGF with AVC, MAC and DTAC extent remained statistically significant, although the associations were attenuated.
Multivariable-adjusted prevalence ratios for the association between HGF and ECC
Multivariable-adjusted per cent difference for the association between HGF and ECC extent
Longitudinal analyses
Over the average follow-up of 2.4 years, participants with the highest HGF levels had an increased risk of incident AVC (incident rate ratios: 1.62 (1.12, 2.34)) and incident MAC (1.45 (1.03, 2.03)) but not incident ATAC or DTAC (table 4). After full adjustment for CVD risk factors in model 3, the association of HGF with incident ECC was no longer statistically significant. Table 5 shows the association between HGF and 2-year progression of ECC. In fully adjusted models, the highest HGF levels were associated with 10% (4%, 15%) increase in MAC progression and 13% (6%, 21%) increase in DTAC progression. However, there was no evidence of AVC or ATAC progression at 2 years.
Multivariable-adjusted incidence rate ratios for the association between HGF and ECC
Multivariable-adjusted per cent change for the association between HGF and ECC progression
We found significant interaction by sex (p<0.001) for the association between HGF and AVC. In the fully adjusted models, men in the highest HGF tertile had 30% (11%, 51%) greater AVC extent at baseline and 10% (2%, 18%) increase in AVC progression at 2 years (online supplemental table S1). There was no evidence of a significant association between HGF and AVC extent or progression in women. We also found significant interaction by race/ethnicity for the association of HGF with MAC (p=0.04) and DTAC (p=0.001). In the stratified analysis by race/ethnicity, we observed that White and Hispanic participants in the highest HGF tertile had an adjusted 31% (12%, 54%) and 27% (10%, 47%) greater MAC extent at baseline, respectively (online supplemental table S2). Chinese-American and Black participants had an adjusted 18% (0%, 39%) and 9% (0%, 19%) increase in MAC progression at 2 years, respectively (online supplemental table S2). In addition, Black participants had an adjusted 32% (4%, 67%) greater DTAC extent at baseline and 20% (6%, 37%) increase in DTAC progression at 2 years while White participants had 17% (5%, 30%) increase in DTAC progression at 2 years (online supplemental table S3).
Supplemental material
Discussion
Summary of results
In this multiethnic cohort of adults free of CVD at baseline, we found that HGF levels in the highest tertile (tertile 3) were associated with greater risk of prevalent ECC compared with the lowest tertile (tertile 1). However, in the fully adjusted models, there was no evidence of a similar association for incident ECC. The highest levels of HGF were associated with greater ECC extent at baseline but with only MAC and DTAC progression at 2 years. There was evidence of an association of the highest HGF levels with AVC extent and progression in men but none in women. A greater MAC extent at baseline was observed in White and Hispanic participants with HGF levels in tertile 3, while an increase in MAC progression at 2 years was observed in Chinese-American and Black participants. Among Black participants, HGF levels in tertile 3 were associated with greater DTAC extent, while an increase in DTAC progression at 2 years was seen in White and Black participants.
Comparison to previous studies
The findings of our study are comparable to prior research that examined the association between HGF and progression of atherosclerosis. In one study, the authors found that higher levels of HGF were significantly associated with greater progression of atherosclerosis measured by CAC and carotid plaque.6 However, another study from the same population found that in the overall cohort, change in HGF levels over a 2-year period was not significantly associated with progression of atherosclerosis measured by CAC, but among Black participants, change in HGF levels was associated with 70% increase in the risk for progression of atherosclerosis.14 Our findings extend the results of these studies by providing evidence for the role HGF may play in atherosclerosis at multiple extracoronary sites. Although CAC and ECC may share similar risk factors, these risk factors do not necessarily overlap across vascular beds.
Explanation of findings
HGF is a cytokine released by mesenchymal cells in response to endothelial damage and dysfunction. Our findings showing that higher HGF levels are associated with the presence of ECC may be attributable to the actions of HGF through the c-Met/Akt/Notch3 signalling pathway to activate pathological vascular calcification in smooth muscle cells.6 21 Additionally, the angiogenic properties of HGF in the formation of vascular plaque facilitate the progression of atherosclerosis.22 The lack of statistical significance for incident ECC and progression in some vascular beds could be due to small sample sizes and insufficient duration of follow-up and may not necessarily be explained by the presence of confounding factors.
In stratified analyses, the highest HGF levels were linked to a greater risk of AVC extent at baseline and progression at 2 years in men, but a similar finding was absent in women. Median HGF levels were higher in women than men in this study (918 pg/mL versus 887 pg/mL); however, comparable to the results of prior research, a higher risk factor burden in women does not always translate to a higher risk for atherosclerosis.23 More research is required to understand whether there is a differential effect of sex on the association between HGF and ECC. Furthermore, prior research showed a lesser burden of atherosclerosis among Black and Hispanic participants in the MESA cohort compared with White and Chinese-American participants.24 However, in this study, we found significant associations of the highest HGF levels with a greater burden of atherosclerosis in varying degrees at the different vascular beds for all four racial/ethnic groups. The mechanisms responsible for this racial/ethnic heterogeneity are still under investigation but may indicate the need to develop racial/ethnic-specific nomograms to accurately identify subclinical CVD burden.25
Public health implications
CVD is still the leading cause of morbidity and mortality globally.26 In the USA, the 2020 health-adjusted life expectancy was 67 years and the estimated annual total expenditure on CVD was over $360 billion. Consequently, CVD prevention should remain a public health priority.27 28 As subclinical atherosclerosis precedes the onset of clinical CVD, timely detection may prevent or delay the progression to clinical CVD through more comprehensive risk factor modification. In the management of CVD, clinicians combine the clinical assessment of patients with additional tools to improve risk stratification, diagnosis, treatment and prognostication.29 These additional tools include biomarkers measured and quantified from blood, tissue and urine samples or assessed by imaging techniques.29 Evidence from this study and prior studies suggest that HGF can be utilised to estimate the likelihood of subclinical atherosclerosis, CHD, stroke and heart failure.6 7 9 14 However, there is a need for more well-designed prospective studies to replicate and validate the findings of our study, so the full potential of HGF can be optimised. Furthermore, future research could explore the inclusion of HGF as a risk-enhancing factor to improve the precision of atherosclerotic CVD risk stratification.
Strengths and limitations
Strengths of this study include the prospective cohort design and the use of a large, community-based multiethnic sample. MESA employed highly standardised methods to collect data on a broad array of CVD risk factors and measures of calcium outside the coronary beds. Nevertheless, our study findings should be interpreted in the context of the following limitations. First, our study was observational, so we cannot prove causality or rule out the likelihood that unmeasured or inadequately measured confounders may be responsible for the observed associations. Second, our findings may not truly represent the general population because the selection of MESA participants was not randomised. In addition, since participants were required to be free of CVD at the time of enrollment, those with higher risk for ECC may have been excluded, thus attenuating the strengths of associations observed. Third, we assessed circulating HGF and not tissue-specific HGF but prior research shows that both measurements are correlated.6 30 Fourth, the interval between examination 1 CT and examination 2/3 CT measurements may not have been sufficient to demonstrate an association between HGF and ECC incidence/progression in all the extracoronary sites. Finally, we did not examine the association of HGF with measures of calcification in other vascular locations such as the iliac arteries or aortic arch because the data were not available.
Conclusions
In this multiethnic community-based cohort study of adults free of CVD at baseline, higher HGF levels were significantly associated with greater risk of prevalent ECC and ECC extent independent of traditional CVD risk factors. HGF was also associated with some measures of incident ECC and progression. However, we cannot make causal inferences because of the observational study design. Therefore, additional well-designed studies would be required to replicate and validate the findings of this study to determine whether HGF may represent an alternate biological pathway that could be targeted to reduce CVD risk. Future research could explore the inclusion of HGF as a risk-enhancing factor to improve the precision of CVD risk stratification
Supplemental material
Data availability statement
The data for this study are not publicly available but may be obtained from a third party by submitting a proposal through NIH BioLINCC at https://biolincc.nhlbi.nih.gov/studies/mesa/.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by Johns Hopkins School of Medicine IRB. Applicant number: NA_00030361. Participants gave informed consent to participate in the study before taking part.
Acknowledgments
The authors thank the other investigators, the staff, and the MESA participants for their valuable contributions. A full list of participating MESA investigators and institutions can be found at http://www.mesa-nhlbi.org.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @DrOlaOsi, @RichardAFerraro, @rblument1, @ErinMichos
OO and OO contributed equally.
Contributors OO, OO and EDM designed the study and wrote the first draft of the manuscript. OO performed the statistical analysis. OO, OO, RAF, PMN, NBL, PAD, SJB, RB, MJB and EDM provided critical revisions for important intellectual content. All authors approved the final draft for submission. OO and OO accept full responsibility for the finished work and the conduct of the study, had access to the data, and controlled the decision to publish.
Funding The MESA study was supported by contracts HHSN268201500003I, N01-HC-95159, N01-HC-95160, N01-HC-95161, N01-HC-95162, N01-HC-95163, N01-HC-95164, N01-HC-95165, N01-HC-95166, N01-HC-95167, N01-HC-95168 and N01-HC-95169 from the National Heart, Lung, and Blood Institute (NHLBI), and by grants UL1-TR-000040, UL1-TR-001079, and UL1-TR-001420 from the National Centre for Advancing Translational Sciences. HGF measurement was funded by R01HL98077. Dr. Michos is funded by the Amato Fund for Women’s Cardiovascular Health at Johns Hopkins University, Baltimore, MD, USA.
Competing interests None declared.
Provenance and peer review Not commissioned; internally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.