Article Text

Abstract
Objective Atrial fibrillation (AF) ablation services were significantly affected by the COVID-19 pandemic. We aimed to evaluate a symptom-based clinician prioritisation scheme for waiting list management compared with patient-completed quality of life (QoL) scores. We also sought to understand factors influencing QoL, particularly the impact of COVID-19, on patients awaiting AF ablation, via a bespoke questionnaire.
Methods Patients awaiting AF ablation were sent two QoL questionnaires (Atrial Fibrillation Effect on QualiTy of Life (AFEQT) and EuroQol 5D (EQ5D-5L)) and the bespoke questionnaire. At a separate time point, patients were categorised as C1—urgent, C2—priority or C3—routine by their cardiologist based on review of clinic letters.
Results There were 118 patients included with priority categorisation available for 86 patients. Median AFEQT scores were lower in C2 (30.4; 17.2–51.9) vs C3 patients (56.5; 32.1–74.1; p<0.01). Unplanned admission occurred in 3 patients in C3 with AFEQT scores of <40. Although 65 patients had AF symptoms during the pandemic, 43.1% did not seek help where they ordinarily would have. An exercise frequency of ≥3–4 times a week was associated with higher AFEQT (56.5; 41.2–74.1; p<0.001) and EQ5D (0.84; 0.74–0.88; p<0.0001) scores.
Conclusion The QoL of patients awaiting AF ablation is impaired and AFEQT helps to identify patients at risk of admission, over and above physician assessment. COVID-19 influenced patients seeking medical attention with symptomatic AF when they normally would. Regular exercise is associated with better QoL in patients awaiting AF ablation.
- atrial fibrillation
- COVID-19
- catheter ablation
- delivery of health care
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Patients with symptomatic atrial fibrillation (AF) are at increased risk of hospital admission particularly with Atrial Fibrillation Effect on QualiTy of Life (AFEQT) scores <65.7.
Catheter ablation has been shown to be highly effective at reducing AF symptoms and improving patient quality of life (QoL).
The COVID-19 pandemic has led to a reduction in the capacity for elective ablation procedures in the UK and worldwide.
WHAT THIS STUDY ADDS
This is the first study to evaluate the impact of the COVID-19 pandemic on patients awaiting AF ablation while evaluating their QoL scores.
This study has identified that most patients have had concerns on the impact of COVID-19 on their AF ablation.
Concerns over COVID-19 were associated with reduced QoL and with patients not seeking medical attention with symptomatic AF when they would normally do so.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE AND/OR POLICY
These findings have important implications highlighting the value of AFEQT alongside physician assessment, in the prioritisation of the most patients with symptomatic AF for AF ablation.
NHS England are encouraging the use of patient-reported outcome measures in patient assessment pre-intervention and post-intervention.
This study highlights the high level of AF symptoms in patients awaiting ablation and supports the use of AFEQT as a tool in patient assessment for AF ablation.
Introduction
Atrial fibrillation (AF) is associated with symptoms in up to two-thirds of patients.1 2 Patients with the most significant symptoms have an increased risk of hospital admission and consume more healthcare resources.3 For symptomatic patients, catheter ablation has been shown to be highly effective at reducing AF symptoms, improving quality of life (QoL) and reducing hospital admissions.4–6 Catheter ablation of AF is recommended as class I indication (level of evidence A) for symptomatic paroxysmal and persistent AF that is not controlled by anti-arrhythmic drugs.4 7
The provision of ablation services throughout the world has been reduced by the COVID-19 pandemic. This has resulted in the cancellation of ablation procedures with procedure numbers reduced by 64% from March to May 2020 in the UK,8 which was also reflected worldwide.9 The impact of COVID-19-related reduced activity and increased waiting time on patients waiting for AF ablation is unknown. We sought to understand whether we could accurately prioritise the most symptomatic patients and understand the impact of the COVID-19 pandemic on the health and QoL of patients awaiting AF ablation.
Methods
Patients on the waiting list for AF ablation at a single institution in August 2020 were assessed. Those who had not yet been assigned a procedure date, were sent a bespoke questionnaire related to the impact of COVID-19 on their AF, along with a symptom-specific and a generic QoL questionnaire. The bespoke questionnaire (see online supplemental file 1) assessed comorbidities, daily exercise, medication for AF and the impact of COVID-19 on the patient’s healthcare usage. The AF-specific questionnaire was the Atrial Fibrillation Effect on QualiTy of Life (AFEQT),10 which assesses AF in three domains: AF symptoms, the effect of AF on activities and concerns about AF treatment. The second was the EuroQol 5D (EQ5D-5L)11 questionnaire, which is a generic QoL instrument often used to derive health utilities and thereby assess the cost-effectiveness of healthcare interventions. Patients were sent the questionnaires in the post and asked to return them in a prepaid envelope.
Supplemental material
At a separate time point (July 2020), the cardiologist in charge of the patient’s care was asked to assess the procedure urgency using a three-tier classification based on the three priority system of the Royal College of Surgeons12 as modified by the British Heart Rhythm Society.13
Category 1 (C1)—clinically urgent. For patients with potentially life-limiting AF issues or severe daily symptoms, for example, tachycardia-induced cardiomyopathy.
Category 2 (C2)—high priority. For patients with significant and frequent debilitating symptoms, for example, hospital admissions or inability to work.
Category 3 (C3)—routine. For patients who did not meet the criteria above.
The assessment was made on the basis of the clinic correspondence, and the consultants were blinded to the patients’ responses to the questionnaires as these were sent 1 month later. Results were collated and analysed, by a blinded independent clinician. Statistical analysis was performed using GraphPad Prism with statistical significance taken as p<0.05. Data were tested for normality. Where not normally distributed, data were transformed using log 10 and natural log. Statistical tests used included Student’s t-test, one-way analysis of variance and Fisher’s exact test. The equivalent non-parametric test was used where data could not be normalised. Data are presented here as mean±SEM with ‘n’ representing the number of patients. QoL scores are presented as median values with IQR.
Patient and public involvement statement
The bespoke questionnaire was curated in partnership with the Atrial Fibrillation Association (AFA), which is a patient representative body and involved input from both patients and patient representatives. The questionnaires were posted out to patients.
Results
Of the 142 patients on the active waiting list who were not yet assigned a procedure date, 121 patients (84%) returned completed questionnaires. Data completeness on the returned questionnaires was over 98%, but three patients were excluded due to incomplete entries on the EQ5D and AFEQT (see online supplemental file 2).
Supplemental material
Demographics and AF history
The mean age of the patients was 63±0.9 years, 65% male. The symptom burden was predominantly described as paroxysmal (64.4%; 76 patients) followed by continuous (persistent) symptoms (21.2%; 25 patients) with 16 patients (13.6%) who were unsure about their symptom burden and one incomplete entry. The duration from first AF symptoms was variable ranging from a few months to over 10 years. There were 23 (19.5%) patients who had a diagnosis of AF for >10 years. Most patients (78/118; 66.2%) had a previous AF-related hospital admission. These results are shown in table 1.
Demographics and AF patterns in patients awaiting AF ablation
Waiting list prioritisation
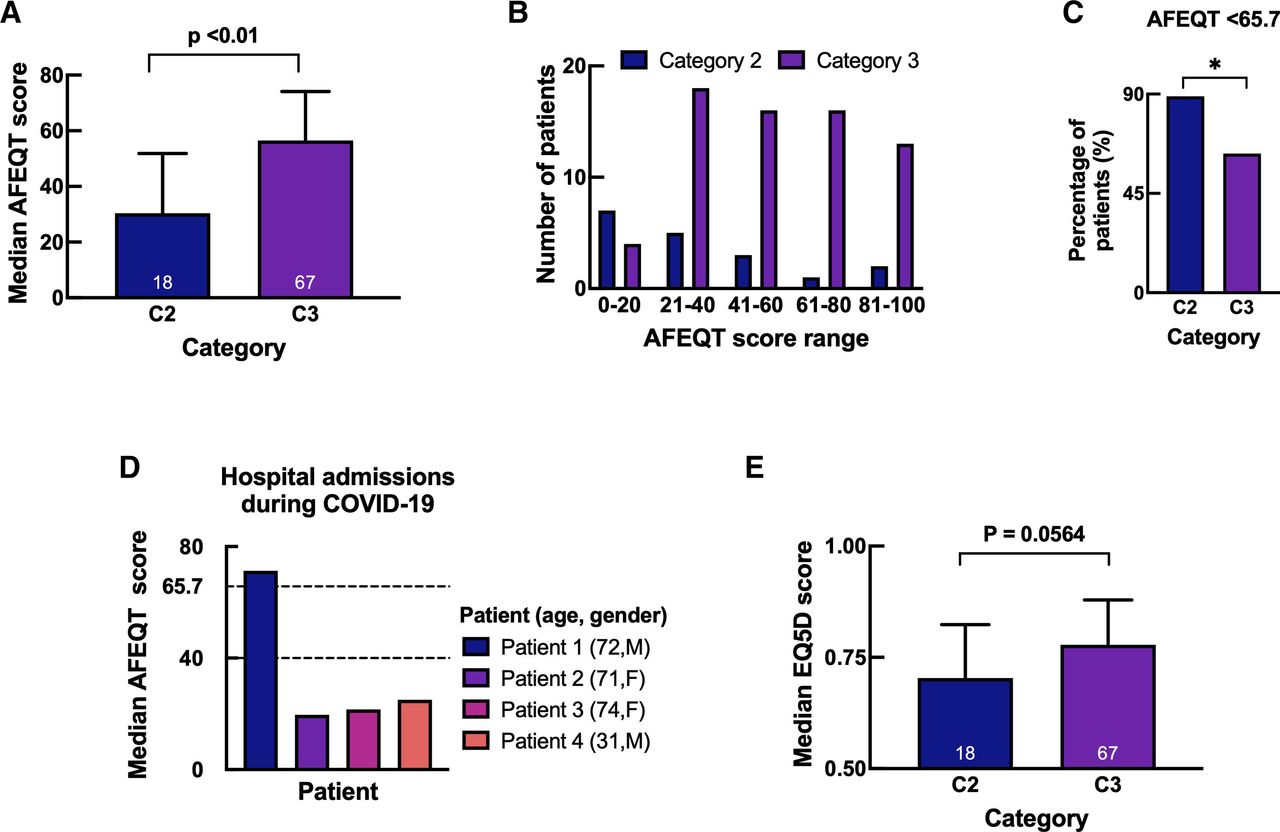
There were 86 patients who had consultant assessment of patient prioritisation and a returned questionnaire with a QoL score. These patients were representative of the total group of 118 patients (see online supplemental file 3). The sole patient in category 1 (C1—clinically urgent) had already been assigned a procedure date and therefore was excluded. There were 18 patients in category 2 (C2—high priority) and 67 patients in category 3 (C3—routine) (see online supplemental file 2). C2 patients had lower median AFEQT scores (30.4; 17.2–51.9) compared with C3 patients (56.5; 32.1–74.1; p<0.01) (figure 1A). The distribution of AFEQT scores in C2 and C3 is demonstrated in figure 1B. The proportion of patients with an AFEQT score of <65.7, which in the Outcomes Registry for Better Informed Treatment of Atrial Fibrillation (ORBIT-AF) registry was a marker of increased hospital resource utilisation,1 was higher in C2 (89%) compared with C3 (63%; p<0.05) (figure 1C). In total, there were six (6/118) patients with unplanned hospital admissions. Of the 85 patients with priority categorissation data available, there were 4 unplanned hospital admissions. All four patients were in the C3 priority group, although three had extremely low AFEQT scores (<40) (figure 1D). Of the remaining two patients, with no priority categorisation data available, one had an AFEQT score <40. This suggests that 66.7% (4/6) patients with unplanned hospital admissions had extremely low AFEQT scores. Generic QoL assessment with the EQ5D was less sensitive than AFEQT, in differentiating C2 and C3 patients, although scores were lower in C2 patients (0.7; 0.4–0.82) compared with C3 (0.78; 0.62–0.8; p=0.056), this did not reach statistical significance (figure 1E).
Supplemental material

Quality of life scores and patient prioritisation. The median Atrial Fibrillation Effect on QualiTy of Life (AFEQT) (A) and EuroQol 5D (EQ5D-5L) (E) scores in patients from category (C)2 and C3. (B) Distribution of AFEQT scores in C2 and C3. (C) Percentage of patients within each category with an AFEQT score <65.7; n=85. White text within bars denotes number of patients. Statistical significance determined by t-test and Fisher’s exact test. (D) AFEQT scores from the four patients who had hospital admissions during the COVID-19 pandemic.
To understand which aspect of AF was driving the clinical prioritisation between C2 and C3 patients, we analysed the three subgroups of AFEQT: symptoms, daily activities and concerns regarding treatment. There was no significant difference in the level of symptoms between patients in C2 (50; 16.7–67.7) and C3 (58.3; 38.9–83.3; p=0.135). However, C2 patients had significantly lower median AFEQT scores in the daily activity domain (29.2; 12–45.8) compared with C3 patients (56.3; 20.8–77.1; p<0.05), and AFEQT concerns domain (C2 26.4; 7.64–53.5 vs C3 55.6; 36.1–69.4; p<0.001).
Comorbidities
Most patients (94/118, 79.6%) had at least one comorbidity, with hypertension the most common (44%), followed by peripheral vascular disease (17%), heart failure (10%), diabetes mellitus (9%) and cerebrovascular disease (5%). Patients with heart failure included those with tachycardia-induced cardiomyopathy currently stable in sinus rhythm (5/12), valvular heart disease (2/12), heart failure with preserved ejection fraction (2/12), hypertrophic cardiomyopathy (HCM) (1/12), cardiac sarcoid (1/12) and previous Takutsubo cardiomyopathy (1/12). As part of understanding overall health-related QoL, we collected data on additional comorbidities including angina, arthritis, chronic obstructive pulmonary disease, malignancy, mental health conditions and HCM (see online supplemental file 1 for details). Patients awaiting AF ablation had a variable number of additional comorbidities, ranging from one up to eight conditions. Only a minority of patients reported no other comorbidity (24/118; 20.3%). Most patients had between one and three (78/118; 66.1%) or greater than four (16/118; 13.6%) additional comorbidities.
Exercise
Despite the health issues noted, >60% of patients reported being able to carry out a 30 min period of moderate exercise at least 3–4 times a week. Most patients exercised 3–4 times per week (25.4%), followed by 5–6 times per week (17.8%), and daily (16.9%). There were fewer patients exercising less at 1–2 times per week (11%), or less than once per week (10%) but a significant number reporting never doing exercise (17.8%). There was a single incomplete entry.
Pharmacological therapy
The majority of patients (91.5%) were on drug therapy in the form of a single agent (51.7%) or combination therapy (39.8%) with only a small proportion of patients not on any medical therapy (6.8%). According to the National Institute for Health and Care Excellence guidance, all patients planned for rate or rhythm control were offered beta-blockers as first-line therapy depending on symptoms, heart rate, comorbidities and preference.14 Beta-blockers alone were used as a single agent in 37% of patients, or in combination therapy with a class IC agent in 16% or with a class III agent in 15%. Sole use of a class III agent (amiodarone or sotalol) was lower at 7%, as was standalone use of class IC agents (flecainide or propafenone) at 5%. A smaller number of patients were on calcium-channel blockers (2%) and digoxin (1%). There was one patient on a combination of calcium-channel blockers and a class IC agent. Triple antiarrhythmic drug (AAD) strategy was only used in a small proportion of patients (3%).
Most patients (88.2%) were anticoagulated, predominantly with a novel oral anticoagulant (NOAC) (84.8%), with a small proportion with warfarin (3.4%). There were 12 patients (10.2%) who were not anticoagulated with incomplete entries from 2 patients. Here, there were 9 patients with a CHA2DS2VASc 0 and 2 patients with a CHA2DS2VASc 1 with a single patient with a CHA2DS2VASc 2 who was intolerant to NOACs.
Patient perspective of COVID-19 impact on AF treatment
The unique aspect of this study was to explore the impact of the COVID-19 pandemic on patients awaiting AF ablation. We explored patient’s levels of concern regarding potential delays to their AF ablation procedure with 2/3 of patients expressing a moderate (36.4%) to severe (30.5%) level of concern about potential delays. We also sought to assess how the pandemic had affected patient’s presentation to medical services. AF symptoms for which the patient would ordinarily have sought medical attention were reported by 65 of the 118 patients (55.1%). A significant proportion of patients (28/65; 43.1%) did not seek medical attention despite these symptoms. For those that sought medical attention this was evenly distributed between the patient’s general practitioner (21/65; 32.3%), and the accident and emergency department (19/65; 29.2%), although eight patients (12.3%) required the assistance of more than one healthcare provider. Only a few patients required a hospital admission (6/65; 9.2%).
Factors influencing QoL
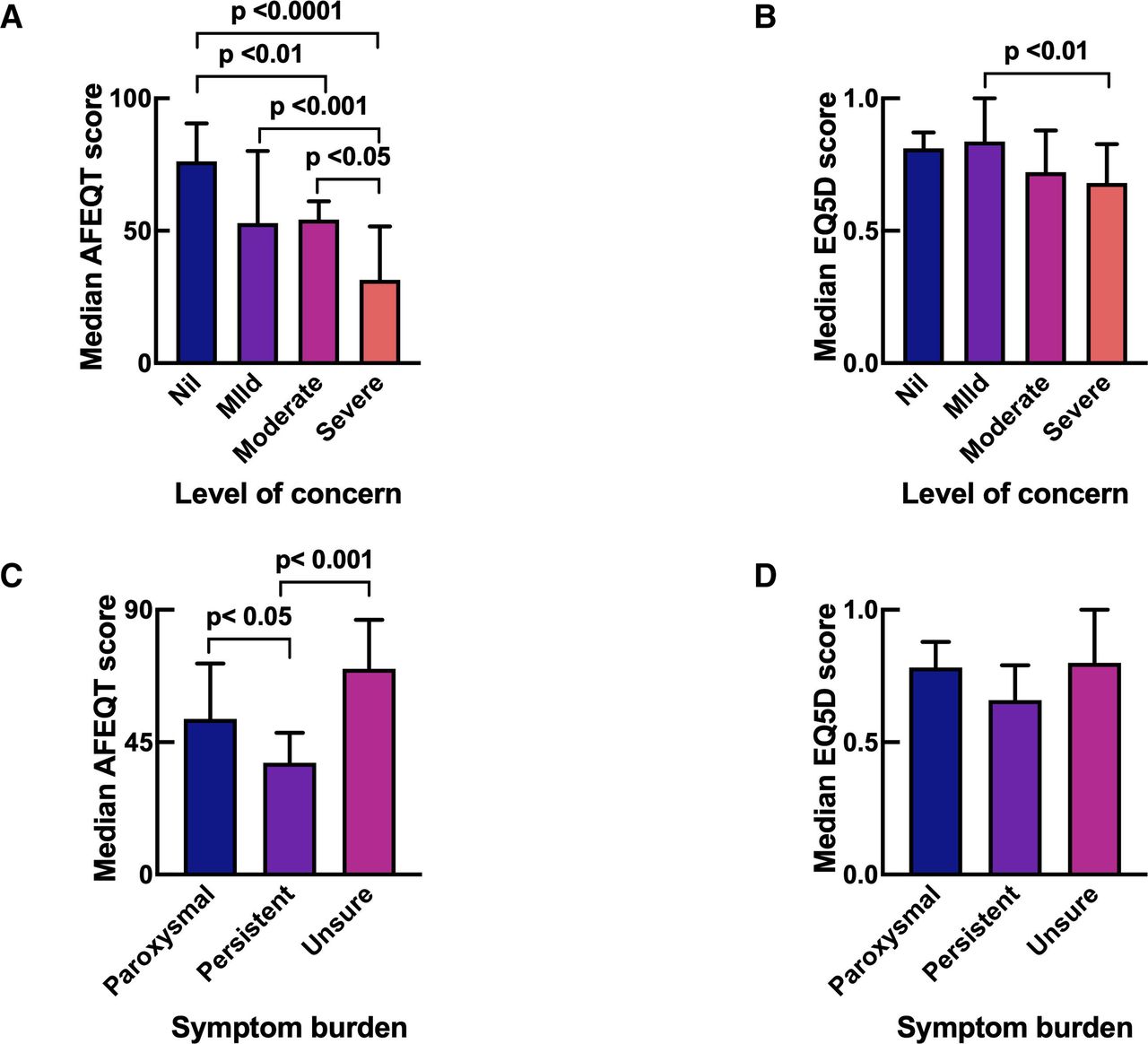
The bespoke questionnaire allowed us to better understand factors underlying the QoL of patients awaiting AF ablation. There was a strong association between patients who expressed a greater degree of concern regarding the potential delays to their AF ablation due to COVID-19 demonstrated and lower median AFEQT (figure 2A) and EQ5D scores (figure 2B). There was also a link between AF symptom awareness and the AFEQT scores. Those who could not report their exact pattern of AF had higher AFEQT scores (69.9; 44–86.6) than patients who knew they had persistent AF (38; 26.4–48.2; p<0.001), or paroxysmal AF (52.9; 30.3–71.8) (figure 2C). Although EQ5D scores were lower in those with persistent AF, the differences to the other groups were not statistically significant (figure 2D).
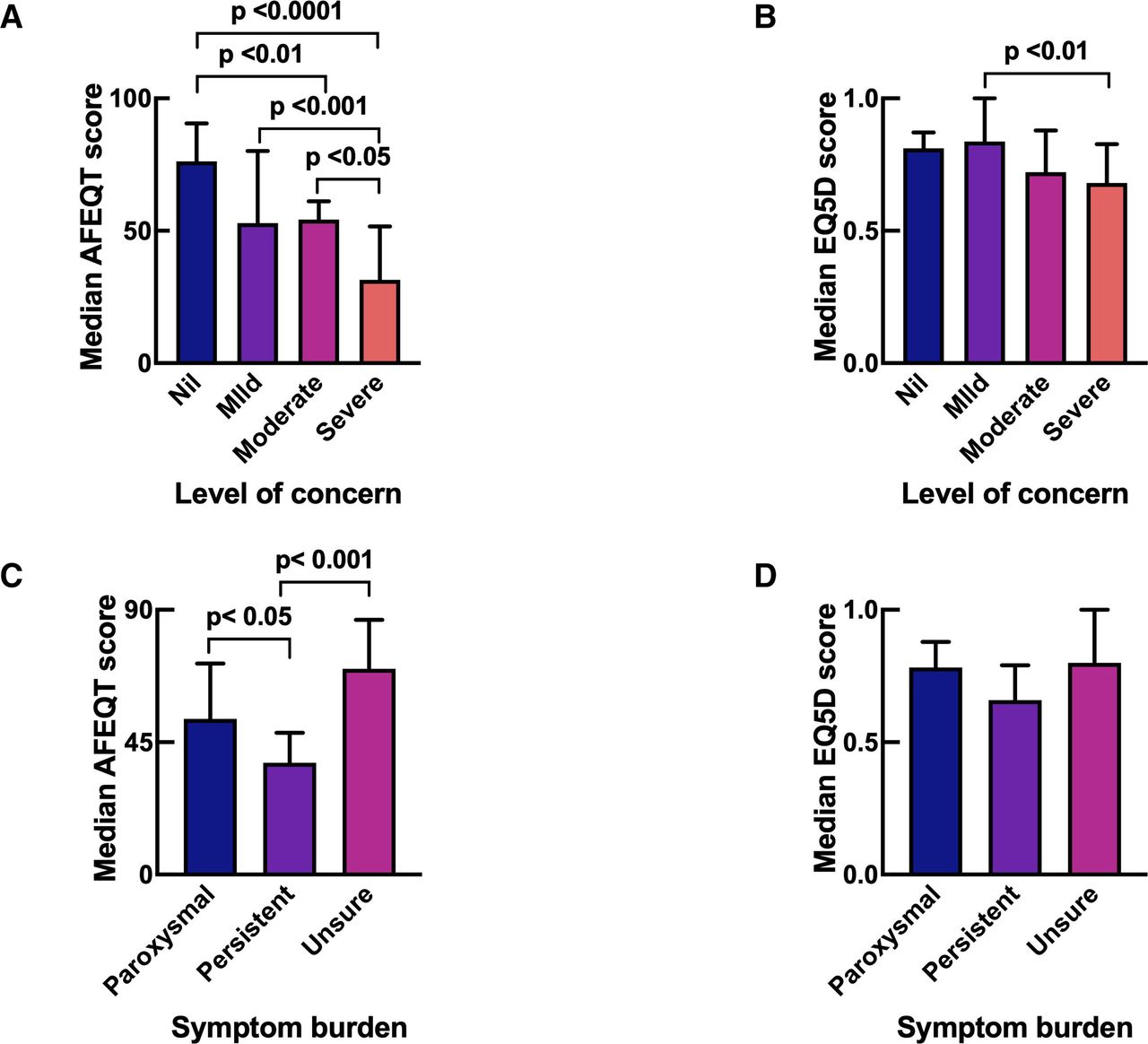
Quality of life scores. Median Atrial Fibrillation Effect on QualiTy of Life (AFEQT) (A) and EuroQol 5D (EQ5D-5L) (B) scores in patient expressing varying degrees of concerns regarding the impact of COVID-19 on their planned AF ablations; n=115 (excluding three incomplete entries). Median AFEQT (C) and EQ5D (D) scores and symptom burden; n=117 (excluding one incomplete entry). Statistical significance determined by one-way analysis of variance.
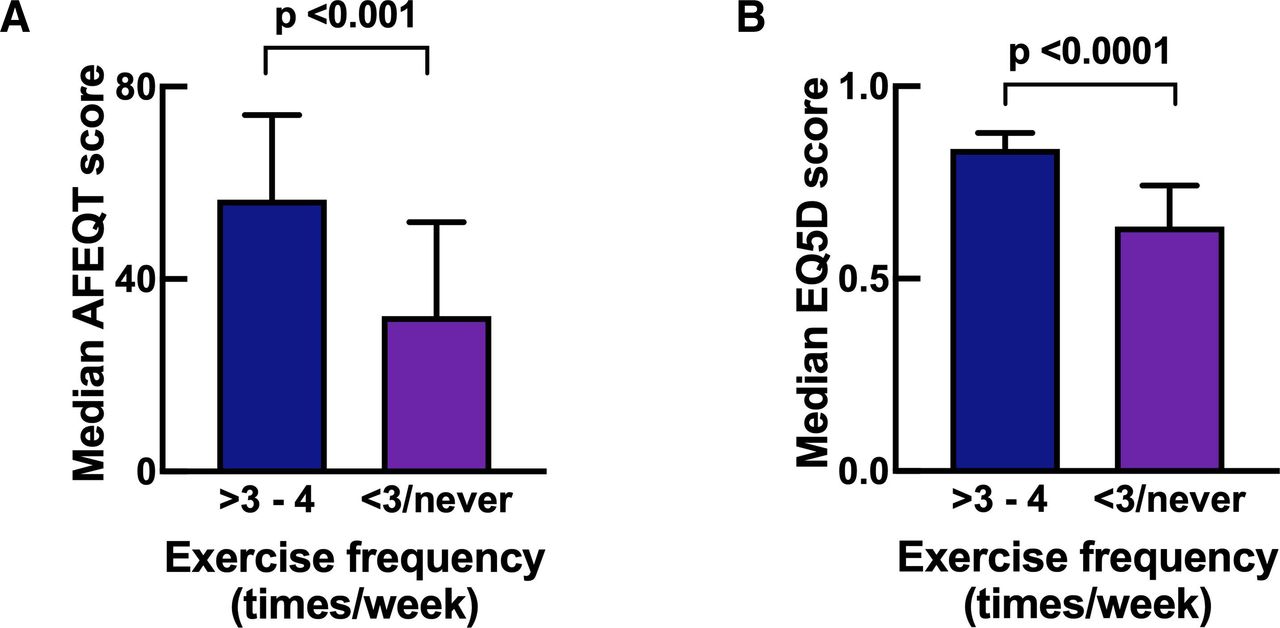
Patients who reported being able to carry out a 30 min period of moderate exercise at least 3–4 times per week demonstrated significantly better median AFEQT (56.5; 41.2–74.1; p<0.001) and EQ5D (0.84; 0.74–0.88; p<0.0001) scores compared with median AFEQT (32.3; 22.8–51.9) and EQ5D (0.64; 0.40–0.74) scores in patients who reported exercising less than 3–4 times per week or never exercised (figure 3A,B).

Relationship between exercise frequency and quality of life scores. Median Atrial Fibrillation Effect on QualiTy of Life (AFEQT) (A) and EuroQol 5D (EQ5D-5L) (B) scores in patients awaiting AF ablation who exercised more or less than 3–4 times per week. The blue bar represents patients who exercise more than 3–4 times per week. The purple bar represents patients who exercised less than 3–4 times per week; n=117 patients (one patient excluded for incomplete entry). Statistical significance determined by t-test.
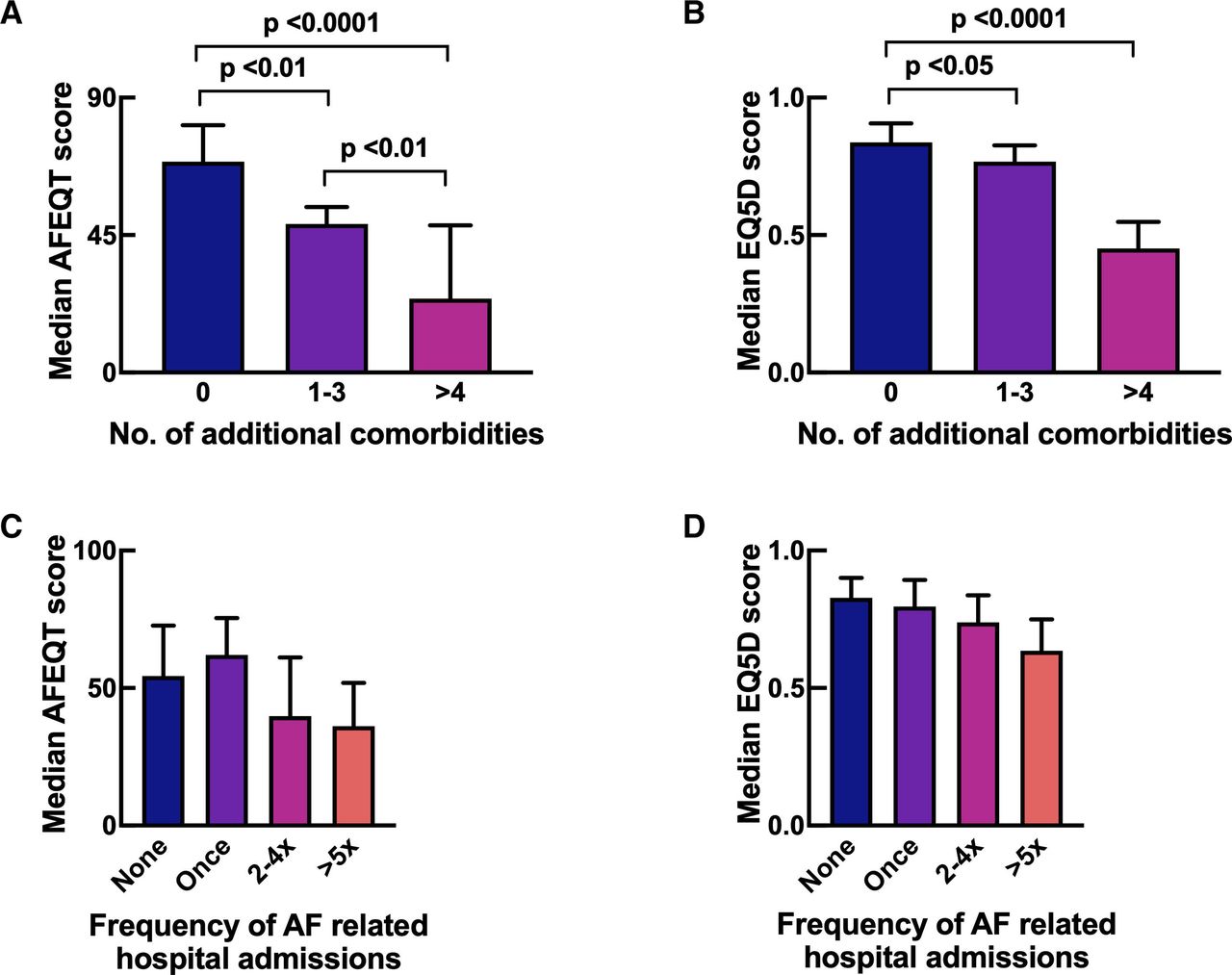
As expected QoL scores were reduced in patients with higher levels of comorbidity. Patients with no additional comorbidities demonstrated significantly higher median AFEQT scores (69; 55.8–82.7) compared with patients with one to three additional comorbidities (48.6; 31.5–68.8; p<0.01) and patients with more than four comorbidities (24.2; 16.7–43.5; p<0.0001) (figure 4A). There were also significant differences in the EQ5D scores for these groups (figure 4B).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Quality of life scores, comorbidities and hospital admissions. Median Atrial Fibrillation Effect on QualiTy of Life (AFEQT) (A) and EuroQol 5D (EQ5D-5L) (B) scores in relation to the number of additional comorbidities in patients awaiting AF ablation. Frequency of lifetime AF-related hospital admission and median AFEQT (C) and EQ5D (D) scores in patients awaiting AF ablation; n=118 patients. No., number. Statistical significance determined by one-way analysis of variance.
We looked at the relationship between the number of previous AF-related hospital admissions and QoL scores. There was a trend towards lower median AFEQT and EQ5D scores in patients with more hospital admissions (figure 4C,D), although the differences were not statistically significant.
Discussion
The use of formalised QoL scores, such as AFEQT and EQ5D, provides additional insights for the physician into the impact of AF on a patient’s QoL. While the EQ5D represents a more generic questionnaire with a broader view on patient’s QoL, the AFEQT represents a more AF-specific comprehensive evaluation of patient’s perceptions of their symptoms, functional impairment, treatment concerns and satisfaction with treatment15 and thus possibly the reason we observed stronger statistical significance with AFEQT scores in our work. Our study shows that although doctors experienced in AF management do accurately assess priority for AF ablation based on clinic letters, that in a proportion of cases additional important information that helps with patient-specific assessment can be gained from the use of the AFEQT. The addition of an AFEQT score at the time of the initial clinical assessment may have highlighted the significant impact of AF on certain patients, allowing appropriate prioritisation of their procedures. Cardiologists often focus on AF symptoms when assessing priority for ablation but it is clear that concerns about treatment and the effect of AF on activities, which may not be as easily assessed are also key in patient assessment. While it is not clear that an earlier procedure would have prevented hospital admission for the three patients who were categorised as routine (C3) but had very low (<40) AFEQT scores (median 21.6), previous trial data have shown that ablation does reduce hospitalisation.5 16
The QoL surveys have also highlighted the highly symptomatic nature of patients on a National Health Service waiting list for AF ablation with a median AFEQT score of 50.9 (IQR 29.6–70.4). This is considerably lower than the AFEQT scores at recruitment in the Catheter Ablation vs Antiarrhythmic Drug Therapy for Atrial Fibrillation (CABANA) trial (median 63). The highly symptomatic nature of the patients waiting for ablation despite drug therapy, and the total duration of AF symptoms, shows that despite increases in UK AF ablation rates,17 there remains a large number of patients with symptomatic AF who could benefit from catheter ablation.
The bespoke questionnaire also offers some insights into factors other than AF that affect QoL. In particular, the links with exercise and concerns about COVID-19 are areas of interest. Not surprisingly concern about COVID-19 linked closely with the ‘concerns’ aspect of the AFEQT. However, the association of more frequent exercise (>3–4 levels per week) with a reduced level of concern about AF on the AFEQT, but not with the symptoms section of AFEQT is a further interesting insight. Patients with AF undergoing a cardiac rehabilitation programme have shown improvements in QoL scores and reduced anxiety.18 Yoga therapy can improve symptoms in paroxysmal AF, and reduce anxiety and depression scores.19 Our data substantiate the beneficial effects of exercise in patients with AF.
Ablation services were greatly reduced during the peak of the COVID-19 pandemic. As services resume, the use of AFEQT may help in prioritisation of the most symptomatic patients. Lifestyle management by encouraging regular exercise,20 in addition to weight loss21 and reduced alcohol intake,22 is also likely to be useful in those awaiting ablation.
Limitations
Some aspects of our study design deserve consideration. This is a retrospective study from a single high volume cardiac electrophysiology centre. Questionnaires were sent out to all patients on the waiting list in August 2020. However, the patient prioritisation system only came into practice in July 2020 due to COVID-19 which meant some patients did not have a priority category. Despite this, we have demonstrated (online supplemental file 3) that the demographic details were similar in both groups. We had to exclude three patients due to incomplete entries on the QoL questionnaires with further exclusions of a small number of patients for incomplete entries on the main questionnaire.
The bespoke questionnaire which was curated in partnership with the AFA has not been previously validated. Additionally, we need to consider the potential effect of patient bias when completing the questionnaire if they felt it may place them higher in the waiting list.
Conclusion
To our knowledge, this is the first study which has evaluated the impact of COVID-19 specifically on AF ablation services. The QoL of patients awaiting AF ablation procedures is significantly impaired. While physician assessments are accurate in prioritising patients awaiting AF ablation, the addition of formal patient-completed QoL assessment such as with AFEQT, is likely to help identify the most symptomatic patients at risk of emergency hospital admissions.
Concerns over COVID-19 are strongly associated with reduced QoL, with some patients not seeking medical attention with symptomatic AF when they would normally do so which is worrying.
We have also observed that QoL scores were better in patients who exercised at least 3–4 times per week. The association of reduced exercise and impaired QoL is complex and may be related to physical symptoms or concerns about AF and COVID-19.
The COVID-19 pandemic has impacted AF ablation services and highlighted the need for improvements in patient assessment and prioritisation.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
Acknowledgments
Atrial Fibrillation Association (AFA) for their contribution to the bespoke questionnaire. A related abstract on this was accepted as an e-poster for EHRA 2021 and includes a supplement in EP Europace (https://doi.org/10.1093/europace/euab116.292).
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Presented at An abstract of this study was presented as an e-poster at the European Heart Rhythm Association Congress 2021 and the abstract published in the EP Europace Supplement (https://academic.oup.com/europace/article/23/Supplement_3/euab116.292/6283060).
Contributors CP: conceptualisation, investigation, data curation, methodology, formal analysis, writing (original draft and editing); HA: data collection; RS: data source, project administration, writing (editing); RA: data source, writing (editing); JEPW: data source, writing (editing); ZB : data source, writing (editing); VL: writing (editing); SMa: data source, writing (editing); SMo: data source, writing (editing); MH: data source, writing (editing); DG: data source, writing (editing); DT : conceptualisation, investigation, data curation, analysis, resources, supervision, guarantor, project administration, methodology, writing (original draft and editing).
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.