Article Text

Statistics from Altmetric.com
Physical inactivity in contemporary obesogenic environments induces cardiac maladaptations, which causes a higher risk of atrial fibrillation (AF).1 Light-to-moderate physical activity (PA), however, is associated with a lower incidence of AF.1–3 Conversely, the long-term practice of strenuous endurance exercise increases the risk of AF in younger, middle-aged and older populations, particularly in highly competitive athletes,4 depicting a U-shaped curve (see figure 1).1 5 The precise causative mechanism/s of exercise-induced AF is still unknown.6 This type of exercising produces structural and functional cardiac adaptations, higher levels of oxidative stress, inflammation and adrenergic activation, ultimately predisposing to atrial fibrosis and AF.1

{kind=link}
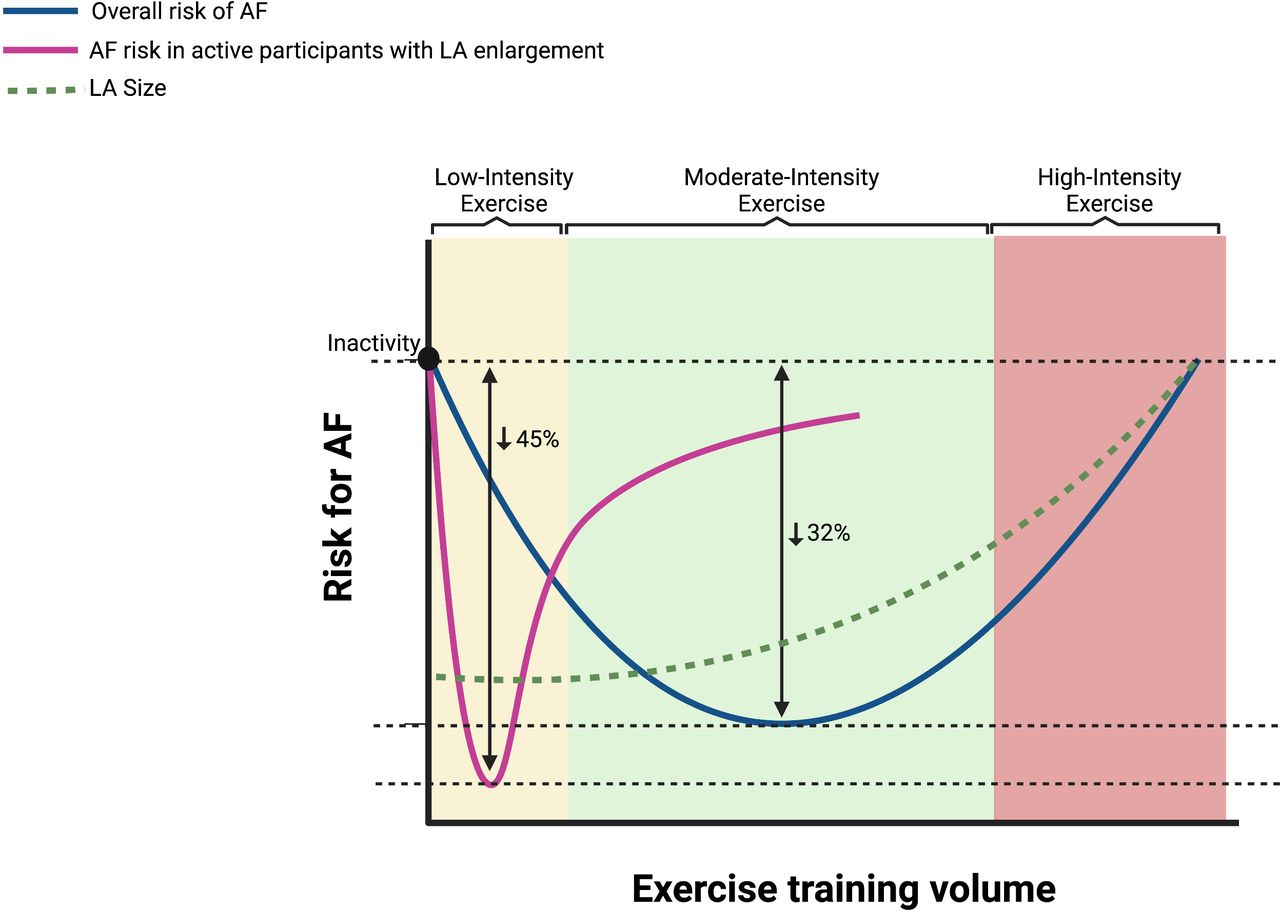
Legend dose–response association between physical activity volume, AF risk, and left atrium enlargement based on Heitmann et al results. AF, atrial fibrillation; LA, left atrium.
Left atrium (LA) dilation or LA enlargement (LAE) is thought to be a potential causative mechanism of exercise-related AF.7 8 In addition, there are likely differences in the aetiology and clinical presentation of AF between endurance athletes and the general (non-athletic) population, that is, ‘classical AF’,9 10 so much so that we described that ‘exercise-induced’ AF, which we coined as ‘Paroxysmal Atrial Fibrillation in Young and Middle-Aged Athletes’ syndrome, usually shows a number of features that are common to most affected athletes.9
Some studies have previously demonstrated more pronounced LAE in the most trained athletes, especially in long-term strenuous endurance exercisers.11 12 We evaluated LA volumes with late gadolinium enhancement MRI (LGE-MRI) in former elite endurance athletes (n=10) and sedentary control subjects (n=5).11 The values of LA volumes corrected for body surface area were significantly higher in athletes compared with control subjects (58±14 mL/m2 vs 39±14 mL/m2, respectively; p=0.026). Recently, Trivedi et al also reported altered LA function between athletes with and without AF, as well as the difference between groups in LA/left ventricle (LV) ratio.13 Importantly, LAE has been independently associated with an increased risk of all-cause mortality in patients with normal LV filling pressure and preserved LV ejection fraction.14 15
Heitmann and colleagues,16 from the University of Norway, as part of the Tromsø Study 1994–2016, reported that moderately active individuals had 32% lower AF risk than inactive, while those with LAE had 38% higher AF risk compared with participants with normal LA size (figure 1). However, the increased AF risk with LAE was attenuated by PA; compared with inactive participants with LAE, the AF risk was 45% lower among active with LAE (see figure 1). AF risk in active participants with LAE did not differ from active with normal LA size. Noticeably, the authors also observed a 79% higher risk of AF in males than in females, as well as those participants ≥65 years had a 2.6-fold higher risk of AF compared with participants<65 years.
There is growing evidence that long-term strenuous aerobic (or ‘endurance’) exercise (eg, marathon/ultra-marathon running) is associated with higher risk of AF (particularly lone AF) compared with age-matched inactive referents17–21 and such increased risk also affects young people.17 22 The association might be particularly strong in elite athletes, although there is still some controversy.12 23 However, the risk of exercise-induced AF might decrease as the population ages17 22 and is overall offset by known beneficial effects of vigorous exercise, that is, attenuation of cardiovascular (CV) disease (CVD) risk factors17 and improved CV health.24 Potential causative factors for de novo development of AF in previously healthy long-term exercisers include LAE/fibrosis, increased parasympathetic tone and inflammation.25–28 Yet more mechanistic research is needed to unveil the actual cause–effect relationships. In contrast, light-moderate PA/exercise (eg, walking/brisk walking) would have an opposite, beneficial effect on AF risk, particularly in old adults.22 29 30
Overall, in agreement with the results reported by Heitmann and colleagues, LAE is one important factor associated with the onset of AF. The study conducted by Heitmann and coworkers increases the evidence on how physical activity or exercise intensity can be implicated in LAE, and hence, in preventing or increasing the risk of suffering AF. Until now, it has not been demonstrated that there is a genetic association of exercise with AF but only that it is related to CV adaptations and/or maladaptations in response to long-term and high-intensity training and/or competition. It seems reasonable to monitor cardiac remodelling and be aware of AF symptoms in these individuals. Finally, there is little evidence to date on the adverse CVD complications, including stroke, of AF in highly trained athletes, with or without LAE, that are well-known complications in many typical patients with AF.
Ethics statements
Patient consent for publication
Ethics approval
This study does not involve human participants.
References
Footnotes
Contributors FS-G and CL have contributed equally in writing this manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Commissioned; internally peer reviewed.
Linked Articles
- Cardiac risk factors and prevention