Article Text

Abstract
Objective To collate existing qualitative research examining patients’ medication-taking experiences in secondary prevention of acute myocardial infarction (AMI) and produce new knowledge, a systematic review and meta-synthesis of patient qualitative studies was conducted.
Method A systematic review found nine reports suitable for inclusion. Themes found by the report authors and report characteristic data were extracted. Reports were assessed for quality. A meta-synthesis using thematic coding and constant comparison method produced higher order themes, and these were used to construct a statement organised by theme using specific examples from the included studies.
Results All patients discussed their medication-taking in thematic categories of beliefs about medication and illness, personal ability and interpersonal factors. Themes differed between classes of medication and between patients, suggesting tailored interventions to medications and individual patients would be appropriate. Some themes overlapped with those discussed by the broader group of cardiovascular patients, but some themes were unique to this myocardial infarction patient group, again indicating that a tailored approach is appropriate for this patient group.
Conclusion The themes of beliefs about medication and illness, personal ability and interpersonal support provide tangible starting points for addressing adherence issues. The concept of medication-taking had unique elements within the post-AMI group of patients, and between classes of medication. While these themes were grouped into more generalised higher-order constructs, there were differences between patients within the themed group, indicating that themes are useful as a guide, but individual-level patient support is appropriate.
- myocardial infarction
- cardiac rehabilitation
- education
- medical
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known about this subject?
Following an acute myocardial infarction, patients find it difficult to adhere to prescribed medication intended to improve their long-term health outcomes. An effective, practical adherence aid is yet to be developed, despite existing research into patients’ experiences of medication-taking. These individual studies arguably lack external validity, which a meta-synthesis could help address.
What does this study add?
This study collates and synthesises qualitative research to elucidate similarities of themes across existing studies to give a rigorous, detailed understanding of medication-taking following an acute myocardial infarction.
How might this impact on clinical practice?
Improving understanding of medication-taking following an acute myocardial infarction allows researchers and practitioners to focus on developing more appropriate medication adherence interventions to assist patients’ adherence and therefore improve their clinical outcomes.
Introduction
Following an acute myocardial infarction (AMI), medical treatment includes a life-long regime of taking five medications, risk factor control and lifestyle changes in order to prevent secondary myocardial infarction or further cardiac events.1 However, medication adherence has been measured to be around 60% in this patient group,2 showing a similar pattern across drug classes and falling as treatment duration continues.3 Poor adherence leads to increased risk of mortality and shortened patient survival,4 re-hospitalisation,5 and incurs increased healthcare costs.6
A Cochrane Review of medication adherence interventions concluded that they are often complex and of little effect.7 Within the larger group of cardiovascular secondary prevention patients, the use of short message service (SMS) texts, a combined pill and healthcare professional support have been found to be beneficial to adherence.8 In the post-AMI patient group, interventions have assisted adherence to cardiac rehabilitation course completion, but not medication adherence,9 while telephone or web-based prompts have a positive effect on adherence.10 The patient perspective of this phenomena is under-researched, and validated theory does not exist, so current interventions to assist medication adherence are based on presumed principles. Qualitative methods are underused in cardiovascular research,11 but could assist in creating a theoretical model and developing an appropriate intervention, the effectiveness of which could then be assessed using quantitative instruments.
This systematic review and meta-synthesis will provide a new account of this phenomena, by organising existing knowledge through comparison and thematic grouping. The aim is to investigate the existing qualitative research of medication-taking post-AMI and summarise themes across all studies, the differences and scope of our present knowledge. To date, this is the first systematic review of medication-taking in secondary prevention of AMI and makes an important contribution to understanding the issues faced by patients in order to develop appropriate interventions to assist their medication-taking.12
Methods
Protocol
This review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses.13 The PROSPERO, Cochrane Library and Joanna Briggs Institute registries were searched for existing work on 7 June 2021, and no systematic reviews of medication-taking post-AMI were found. The protocol for this study was not registered.
Databases and search strategies
A search strategy was developed in collaboration with the academic department’s subject librarian, using keywords within the fields of qualitative studies, medication-taking and AMI. Databases searched were PubMed, Scopus, PsycInfo, Web of Science and the Cochrane Library.
The PICOS tool defined the inclusion criteria for selecting items14 (table 1). The titles and abstracts of the resulting papers were screened against the inclusion criteria for selection. The full text of the selected papers was read in detail before final selection.
Study inclusion criteria based on PICOS tool
Following final selection, a snowball search of each article’s reference list and the ‘cited by’ function using PubMed was used to screen for other potentially relevant articles.
Study selection and data extraction
The search was conducted by HP and AR individually, and then compared and discussed. The search result data were recorded and organised using the EndNote web-based software.
Reporting checklists of included studies
All included studies were critically considered against the consolidated criteria for reporting qualitative research (COREQ) 32-point reporting checklist15 for qualitative studies. This checklist was used to examine how thoroughly the authors had reported the criteria of their studies. This assessment was carried out by HP and AR individually, then compared and discussed.
Synthesis of results
The participant characteristic data and main themes reported by the original authors of each study were extracted and organised using Microsoft Word.
Thematic meta-synthesis was used to organise the findings of the search, chosen as the aim was to describe a specific concept.16 According to this meta-synthesis method, the extracted themes were given line-by-line coding, compared with one another and grouped into common themes of a higher order and finally grouped under more encompassing super-ordinate categories17 (table 2). Comparison tables of thematic groups were produced using Microsoft Word. The original papers were then used to add detail back into a prose statement organised according to the super-ordinate categories.
Themes about medication-taking coded into higher order themes and super-ordinate categories
All data relevant to the study are included in this article or uploaded as online supplemental information 1.
Supplemental material
Patient and public involvement
Patients and the public were not directly involved in the design, analysis, or reporting of this research. This study is intended to be accessible to the public through Open Access publication and forms the foundation of future work by the authors to produce practical interventions that will be further researched through patient involvement and disseminated to wider patient communities.
Results
Study selection
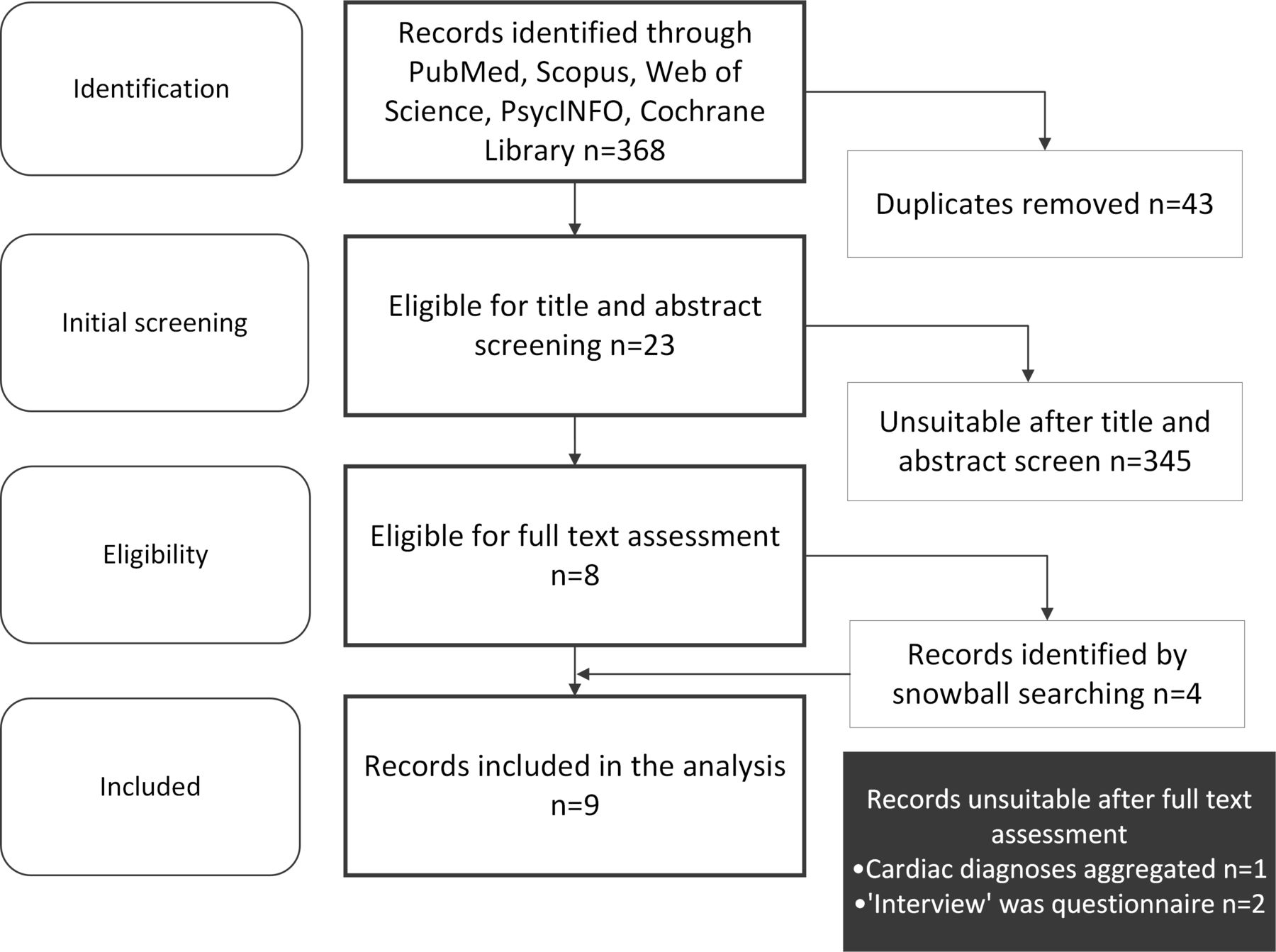
The database searches produced 368 citations, of which 43 duplicates were removed to leave 325 articles for title and abstract screening. This produced 23 eligible articles for full-text screening. Following this, eight articles were included in the review collection.
Snowball searching generated four further eligible articles, one proceeded into full-text review, and was subsequently added to the final review collection which now totalled nine (figure 1).
{kind=link}
PRISMA flowchart of the study selection process. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
There were four super-ordinate thematic categories across the studies: medication beliefs, illness beliefs, personal and interpersonal factors.
Medication beliefs
In summary, patients described positive or negative effects of medication, and balancing the need with their concerns over taking it. They took medication to remain healthy,18 to not foreshorten their life19 and to feel safe.20 The side-effects of medication were described by patients as a bodily effect that needed to be dealt with in itself20 and were not considered to be related to their cardiac issue. The side-effects caused pain, intruded into their lives and were a barrier to their health.21 Similarly, the benefit of medication was unclear along with how it linked to their diagnosis.22 They mentioned conflicting feelings, such as medication being an intrusion but also producing feelings of safety and were balancing the necessity versus their concerns over taking medication.23 The concept of a future recurrence was a reason for medication-taking,23 and medication was seen to be preventative.23
Patients conceptualised medication classes differently, giving dissimilar reasons for discontinuation between classes of medication, for example, those stopping clopidogrel were confused about the treatment duration, and those who discontinued cholesterol lowering medication talked about seeking more natural alternatives.24 Also, patients pitched the side-effects of one medicine against another, as those who discontinued taking clopidogrel described the side-effects of their cholesterol-lowering medication as painful and interfering with life.24
Illness beliefs
Patients’ perception of their own cardiac illness varied; some felt they were in good health,21 or not serious,21 some had neutral feelings,24 or felt their condition was worsening.21 They had differing beliefs about their susceptibility to a further myocardial infarction and were balancing feeling healthy against feeling ill.23 When patients considered their illness to be more severe, they used a friend or family member as reference for comparison to their own illness.24 They considered the possibility of a recurrent event, which could be prevented by taking medication.23 Some patients felt depression following their cardiac event affected their medicine-taking.19
Some believed that their health was out of their personal control, discussing that genetics made it inevitable,21 family history was outside their control,19 or the will of God played a role.23
Several studies featured patients who discontinued one class of medication, finding similarities and differences in illness beliefs between patients. Similar across classes of drugs, patients discontinuing medication had an inaccurate self-perception, a worsening of their condition or denied their illness.21 They showed a reluctance to engage in lifestyle changes, absolving that their previous positive health measures had not prevented their first AMI.19 The severity of illness was perceived to be greater by patients who discontinued taking clopidogrel compared with those who discontinued cholesterol reducing medication.24 Some patients who discontinued cholesterol-reducing medication believed they did not have a cholesterol issue, instead linking cholesterol-lowering medication to patients with high cholesterol, and not seeing the link to their own multi-faceted cardiac condition.24
Personal adherence factors
Personal factors that affected medication-taking were linked to cognition; remembering and understanding their medication dosages. Themes that were elicited included memory,19 memory, attention and decision processes,18 continuity, reinforcement and forgetfulness.23 Linked to this was poor perception,21 patients missing the cues given,21 being confused or receiving information inaccurately.24 The use of a pill-box was given as an example of an adherence aid.18
The ability to self-regulate behaviour was discussed in several studies as a general theme,18–20 and specifically described as patients talked of the discipline required to maintain their own medication,21 their pre-existing beliefs as influences,19 their belief in their own capability, as well as regulating their exercise and eating habits,19 with reinforcement and consequences as an aid to adherence. Similarly, patients stated willpower, a sense of competency and personal preference as influencing their adherence.23
The emotional work required to take medication was described as a toll by patients,19 some discussed the notion of denial of their condition,21 as well as the negative feelings of mistrust21 or distrust of the doctors providing their healthcare.24
Personal identity featured as patients mentioned the incongruity of seeing themselves as patients,18 and comparison to other patients.19 Some felt that medication was forced on them.20 Economic poverty affected medication adherence, with the cost of medication a barrier,21 24 as well as living in a deprived area.23
Interpersonal adherence factors
Medication-taking was helped by healthcare professionals, who provided support,23 reassurance20 and communication.18 Patients blamed poor communication by professionals and poor inter-professional communication as a reason for discontinuing clopidogrel.25 The transition period following hospital discharge was a precarious time for their understanding20 and receiving conflicting information added to confusion about treatment and illness severity. Also, clopidogrel non-adherent patients cited a lack of care continuity, lack of communication and inadequate education as factors.21
Patient’s adherence was strengthened by having knowledge,23 and lack of knowledge was stated as contributing to non-continuation of clopidogrel,21 specifically knowledge about treatment duration and drug purpose.25
Support from family influenced medication-taking,23 26 and a lack of prompt from family and friends featured for non-adherers.21 Cardiac rehabilitation was stated as an influence on adherence,23 and some non-adherers were unaware of the existence of cardiac rehabilitation programmes.21
Discussion
The aim of this study was to define the patient experience of taking medication following an AMI using thematic meta-synthesis of qualitative studies. In relation to medication adherence, patients discussed their illness beliefs, medication beliefs, personal and interpersonal factors.
Using meta-synthesis to collate and interpret the results, the claim for applicability to settings outside of the context each individual study is tentatively strengthened. Similarly, this meta-synthesis makes no claim of generalisability, but is intended to provide a resource to focus further work into theory development for testing in clinical practice.
We have highlighted the themes that patients discussed, but within these themes, patients produced a breadth of specific details, sometimes opposing, suggesting that adherence work should be done at an individual level for personalised assistance, in line with patient-centred medication adherence support advocated by the National Health Service (NHS) clinical guidance.27
The factors extracted in this review relate to the WHO dimensions of medical adherence; namely social/economic-related, healthcare system-related, therapy-related, condition-related and patient-related factors that affect adherence.28
A notable finding is that taking medication reminds patients of their illness, and they attribute bodily effects to medication side-effects and not their original health issue. Patients’ perception of illness varied, both in terms of severity compared with other patients and within themselves, and they balanced ideas of their healthiness with that of their illness.
Medication was seen as protective, and health-maintaining, with the concept of a future event a driver towards medication-taking. However, some patients balanced these beliefs with other more negative arguments that justified their choice to discontinue medication. This shows work is still needed to communicate positive health effects to patients, with dialogue needed to enable patients to voice their concerns. In other studies of medication adherence in chronic illness, patients are more adherent if their perceived need to take medication is greater than their concern over taking them.26 The ambiguity of medication effects could be an issue for post-AMI patients who are asymptomatic or attributing symptoms as side-effects of medication. Practitioners should be aware of this issue when addressing patients’ concerns about their medication.
The themes of knowledge, memory and social support from both family and professionals are important because they are tangible psychosocial factors that can be addressed using behaviour change techniques to assist patients.29
Scientific rigour and quality of results of this paper were strengthened by sourcing from peer-reviewed journals, and the COREQ checklist used as a valid and reliable measure of quality. No studies were deemed ineligible due to their quality, with scoring used as a guide for comparison, rather than an arbitrary cut-off.30
To show the coverage of studies included, it is worthwhile to highlight their epistemological positions.29 Four studies were closest in theoretical paradigm to the aim of this study.18 20 23 26 Two studies assessed the experience following the interventions of support via phone discussion and booklet respectively.19 22 In the trio of related studies,21 24 25 the context was patients who received coronary stent insertion as a result of their AMI. They also appear to have used the same cohort of patients, showing similar numbers and age range, perhaps limiting the breadth of results. Two studies used the Theoretical Domains Framework to organise the themes of their results,18 19 and so were already organised into a higher order domain than the primary interpretations presented in all other studies.
The studies reviewed were biased towards white male participants, with gender not reported, and from English-speaking developed nations with integral academic and healthcare systems. Only one study mentioned purposive sampling to balance ethnicity and socioeconomic status.19
There are two literature reviews that this research builds on. The first was a systematic review of all qualitative literature on medication adherence,31 organised using Theoretical Domains Framework. This found three themes, medication-related burden, medication-related beliefs, which then fed into medication-related practices. There is a clear overlap with our study of medication-related beliefs and illness-related beliefs.
The second study of interest is a literature review of medication-taking behaviour for secondary prevention across patients of all types of coronary heart disease,32 which concluded that medication-taking behaviour was a result of medication-related and disease-related beliefs, and related to clinician relationships, pre-existing health beliefs, socioeconomic and cultural environment, interaction with health systems and influence of partner and family. Again, there is overlap of the broad themes between this paper and ours. This second review included seven studies of AMI patients, four of which were selected in our review. A further five studies that we included were published later.
The authors of the study above found a number of unique themes including chronicity of illness,32 a greater emphasis on fatalism, and patient confusion that they had been cured. Our study adds to this as we found the specific threat of a future event influenced patients’ behaviour, and our study picked up depression as a feature of decisions which was absent in this second review. Of interest is one study of a Gujarati Hindu cohort33 who discussed a significant belief in fate and the will of God, similar to that included in our study.23
This difference in findings supports the argument for tailoring interventions to a specific AMI diagnosis to help guide thematic concepts and predict individual issues. Additionally, acknowledgement of similar experiences assists empathy and developing professional trust.
The authors of this review have a study in publication that is also relevant.34 Our study found that patients discussed similar personal factors to those identified in this paper, for example, the assimilation of medication into their lifestyle, knowledge in general and disruption to routine. Under the theme of illness beliefs, we found that patients considered the future, compared themselves to others, and were keen to distinguish themselves from the notion of a ‘typical’ AMI patient.
Conclusion
This systematic review and meta-synthesis of medication-taking to prevent further AMI has found that patients expressed varied beliefs relating to medication and their illness. Most importantly, patients differed in the concept of their own health and how it related to their cardiac illness, and the effect of taking medication on their bodies and how this influenced their health. They were supported by family and professional help, and their own knowledge, memory and capability assisted their medication-taking.
These findings indicate that intervention work should be done at an individual level, due to personal variation in beliefs, and also at drug class level, as patients conceptualised drug classes differently.
Healthcare professionals can use beliefs about medication and illness as starting points for intervention work, and be observant during everyday practice that patient knowledge, communication and continuity of care are important to help patients with medication-taking following an AMI.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
Ethics approval
No ethical approval was required as data was collected and analysed from previously published studies in which informed consent was obtained from study participants by the study primary investigators.
Acknowledgments
With thanks to Jackie Skinner for assistance with the search strategy.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @HannahPiekarz, @ProfDonyai
Contributors HP responsible for overall content and guarantor of the work; study design, systematic search, data extraction, meta-synthesis, manuscript writing. AR contributed to systematic search and data extraction. CL contributed to study design and manuscript review. PD contributed to study design, manuscript writing and manuscript review.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.