Article Text

Abstract
Background Poor adherence to guideline recommendations for anticoagulation in patients with acute myocardial infarction (MI) and atrial fibrillation (AF) is previously reported. The aim of the present cohort study was to assess time trends in prescription of anticoagulation therapy in a nationwide registry-based cohort of patients with acute MI and AF.
Methods All patients, registered in the Norwegian Myocardial Infarction Registry (NORMI) between 2013 and 2019 with ECG-verified AF at hospitalisation, were included in the cohort study. The primary outcome was the prescription rate of anticoagulation therapy at hospital discharge and follow-up through 2019.
Results AF was observed in 8565 (10.9% of 78369) patients registered in the NORMI from 2013 through 2019. The congestive heart failure, hypertension, age ≥75 (doubled), diabetes, stroke (doubled), vascular disease, age 65–75, and sex (female) score was ≥2 in 7845 (92%) of the hospitalised patients with AF, and in 7174 (96%) of 7440 patients discharged alive. Only 3704 (47.2%) of these patients were treated with anticoagulation prior to the MI. The prescription rate of anticoagulation therapy at discharge was 55% in 2013, increasing to 78% in 2019 (annual per cent change 6.0 (95% CI 0.7 to 11.6)). Patients prescribed anticoagulation therapy had reduced risk of all types of stroke or death at follow-up compared with patients without prescription of anticoagulation therapy (multivariate-adjusted HR 0.8, 95% CI 0.7 to 0.8, p<0.001).
Conclusions The prescription rate of anticoagulation therapy in patients with MI and AF increased during the study period, but many patients were still undertreated with respect to stroke prevention.
- anticoagulation
- stroke
- atrial fibrillation
- myocardial infarction
Data availability statement
Data may be obtained from a third party and are not publicly available. The data underlying this article were provided by the Norwegian Institute of Public Health under licence/by permission. Data will be shared on request to the corresponding author with permission of the Norwegian Institute of Public Health.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known about this subject?
Poor adherence to guideline recommendations for anticoagulation therapy in patients with acute myocardial infarction (MI) and atrial fibrillation (AF) is previously reported.
What does this study add?
The prescription rate of anticoagulation therapy in Norway in patients with MI and AF increased during the period 2013–2019, but many patients were still undertreated with respect to stroke prevention.
How might this impact on clinical practice?
Knowledge of current clinical practice may improve adherence to guideline recommendations and consequently improved treatment of patients with MI and AF.
Introduction
Atrial fibrillation (AF) is the most common sustained cardiac arrhythmia.1 The incidence of AF is increasing, and one in three middle-aged persons may develop AF during their lifetime.2 AF is associated with increased morbidity and mortality and remains one of the major causes of stroke.3 4 The European Society of Cardiology (ESC) guidelines strongly recommend treatment with anticoagulation therapy in patients with AF with an increased risk of stroke.4 However, several studies have previously demonstrated low physician adherence to this recommendation.5–7 In patients with AF and myocardial infarction (MI), the prescription of anticoagulation has been particularly challenging, since these patients also need antiplatelet treatment.7 However, the ESC guidelines underscore the importance of treatment with anticoagulation also in these patients.4
The aim of the present cohort study was to investigate time trends in adherence to the ESC guideline for prescription of anticoagulation therapy in patients with AF discharged from hospitals in Norway after MI in the period from 2013 to 2019.
Methods
The Norwegian Myocardial Infarction Registry
The Norwegian Myocardial Infarction Registry (NORMI), a part of the Norwegian Cardiovascular Disease Registry, is a national quality register. Registration into NORMI is mandatory without requiring patient’s consent. For definition of MI, the NORMI adhered to the Third and Fourth Universal Definition of Myocardial Infarction during the study period.8 9 NORMI contains information on gender, age, cardiovascular risk factors, previous diseases and medication, symptoms and clinical findings, ECG (rhythm and ischemic changes), in-hospital therapy and complications including death as well as drugs prescribed at hospital discharge. The registration and quality of the information in the register have been described previously.10 11
The Norwegian Cardiovascular Disease Registry contains information on stroke (all types) and all-cause death after hospital discharge.
Study population
All patients admitted to hospitals in Norway with acute MI between 1 January 2013 and 31 December 2019 and registered in the NORMI were considered for inclusion in this cohort study. In patients with more than one MI during the inclusion (study) period, only data from the first MI (index MI) were used. The diagnosis of AF was based at ECG findings at hospital admission.
Outcomes and follow-up
The primary outcome was the prescription rate of anticoagulation therapy at hospital discharge in patients with the combination of MI and AF and an indication for anticoagulation. The secondary outcome was a composite of all-cause mortality or non-fatal stroke (all types) during follow-up. Follow-up data were available until 31 December 2019.
Stroke risk and indication for anticoagulation therapy
The stroke risk in patients with AF was estimated based on the ESC recommended congestive heart failure, hypertension, age ≥75 (doubled), diabetes, stroke (doubled), vascular disease, age 65–75, and sex (female) (CHA2DS2-VASc) risk score tool.4 12 The CHA2DS2-VASc scores were calculated from information at hospitalisation (with addition of 1 point on discharge due to acute MI). A CHA2DS2-VASc risk score of ≥2 was considered as an indication for anticoagulation therapy.4
Patient and public involvement
This study used existing data from Norwegian national health registries. Registration into these registries is mandatory (the Norwegian Cardiovascular Disease Registry Regulation and the Norwegian Health Register Act), and consent by the patient was not required.
Statistics
Continuous variables are presented as the mean±SD or median (25th percentile, 75th percentile), and differences between groups were analysed using independent samples t tests. Categorical variables are presented as numbers and percentages, and differences between groups were analysed by the χ2 test. Time trends were analysed (log-linear model) using the Joinpoint Regression Program (V.4.0; SEER software, National Cancer Institute, USA) and are presented as the expected annual per cent changes (APC) with a 95% CI. Kaplan-Meier curves for event-free survival after hospital admission for the first MI in the study period were estimated and Cox regression analyses were used to calculate HRs with 95% CIs for the combined endpoint all-cause mortality or non-fatal stroke. Non-fatal stroke competing risk analysis with all cause death as competing event was based on Fine and Gray’s proportional subhazards model. The following covariates were included in the multivariable analyses: gender, age, smoking, previous stroke, previous MI, history of heart failure, diabetes, antihypertensive treatment, renal failure (estimated glomerular filtration rate (eGFR) <60 mL/min) and out-of-hospital cardiac arrest (prior to hospitalisation for index MI). The proportional hazard assumptions were checked with the proportional-hazards assumption test based on Schoenfeld residuals and log-log plot of survival. A p value of <0.05 was regarded as statistically significant. The data were analysed using STATA, V.17 (StataCorp LLC, College Station, Texas).
Results
From 1 January 2013, through 31 December 2019, 78 369 patients with MI were registered in the NORMI (figure 1). AF was identified in ECG at hospitalisation in 8565 (10.9%) patients. The yearly proportion of patients with MI with AF was stable throughout the study period. The prevalence of AF increased with age (<50 years, 1.6%; 50–59 years, 2.5%; 60–69 years, 5.5%; 70–79 years, 12.0% and ≥80 years, 20.9%). A total of 7845 (92%) patients with AF had CHA2DS2-VASc risk score ≥2 at hospitalisation. Of 7440 patients with AF discharged alive, 7174 (96%) had CHA2DS2-VASc risk score ≥2.

Patients admitted to hospitals in Norway with myocardial infarction from 2013 to 2019. CHA2DS2-VASc, congestive heart failure, hypertension, age ≥75 (doubled), diabetes, stroke (doubled), vascular disease, age 65–75, and sex (female).
Clinical characteristics at hospital discharge after MI in patients with AF and CHA2DS2-VASc risk score ≥2 are described in table 1.
Clinical characteristics at hospital discharge in patients with myocardial infarction, atrial fibrillation and CHA2DS2-VASc risk score ≥2, Norway 2013–2019, n=7174
Anticoagulation therapy
Among the 7845 patients with AF and CHA2DS2-VASc risk score ≥2 at hospitalisation, 3704 (47.2%) patients used anticoagulation therapy prior to the MI. Among the 7174 patients with AF and CHA2DS2-VASc risk score ≥2 discharged alive from hospital after MI, 4809 (67.0%) patients were prescribed anticoagulation therapy. Patients with a previous diagnosis of hypertension or heart failure were more likely to be discharged with anticoagulation therapy compared with patients discharged without anticoagulation therapy, but we found no differences regarding gender, diabetes and previous stroke (table 1).
The use of anticoagulation therapy increased during the study period with an APC of 3.1 (95% CI 0.1 to 0.6) and 6.0 (95% CI 0.7 to 11.6) pre and post-MI, respectively (figure 2). In 2013, 55% of the patients with AF and CHA2DS2-VASc risk score ≥2 discharged alive from hospital after MI were prescribed anticoagulation therapy, and in 2019, the proportion has increased to 78%.

Proportion of patients with atrial fibrillation prescribed anticoagulation therapy prior to and after hospitalisation for acute myocardial infarction, Norway 2013–2019.
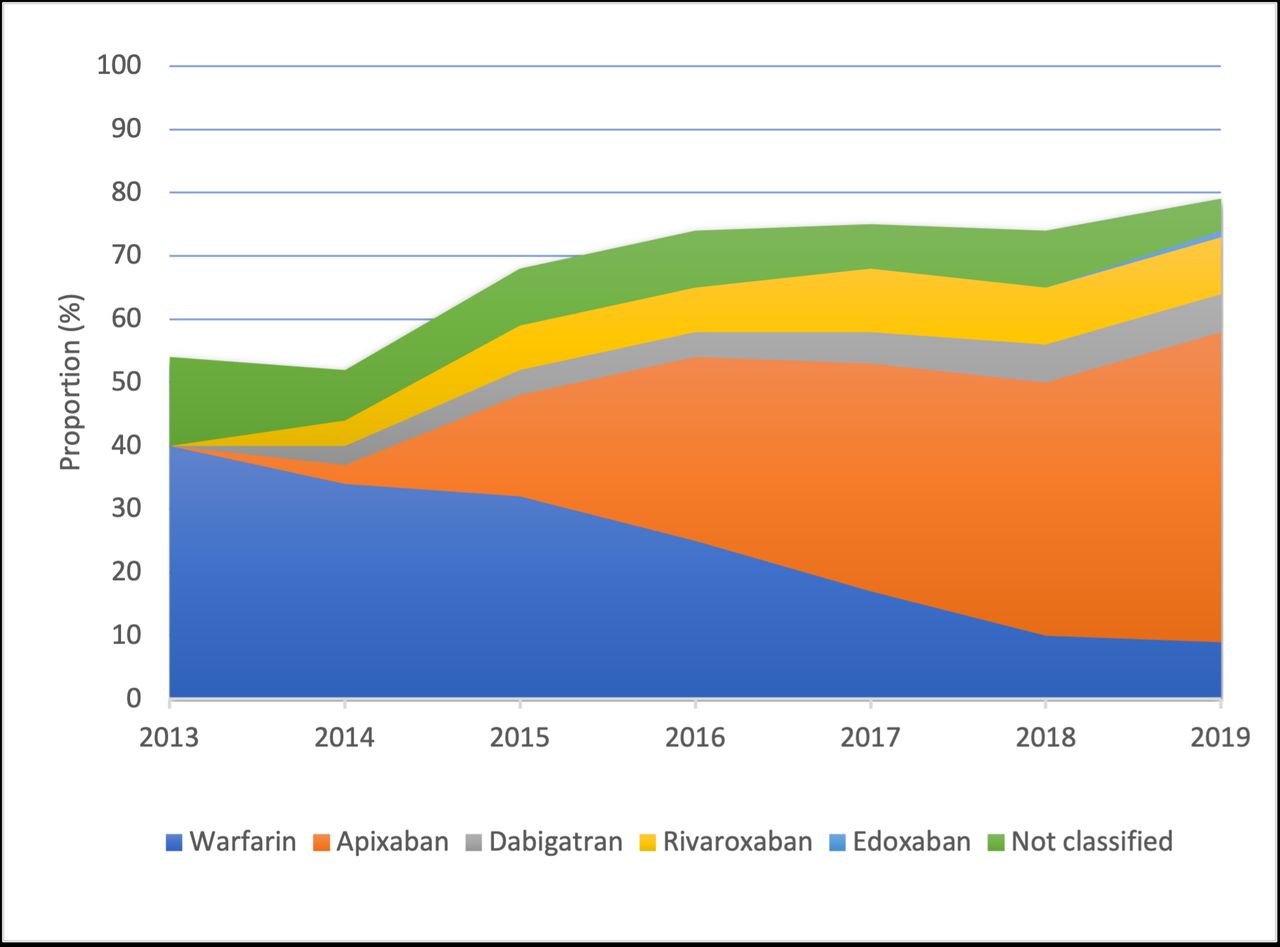
The prescription of different anticoagulation drugs at hospital discharge during the study period is presented in figure 3. Warfarin was the preferred anticoagulation therapy in the beginning of the study period, while most patients were prescribed a non-vitamin K oral anticoagulant (NOAC) at the end of the period.
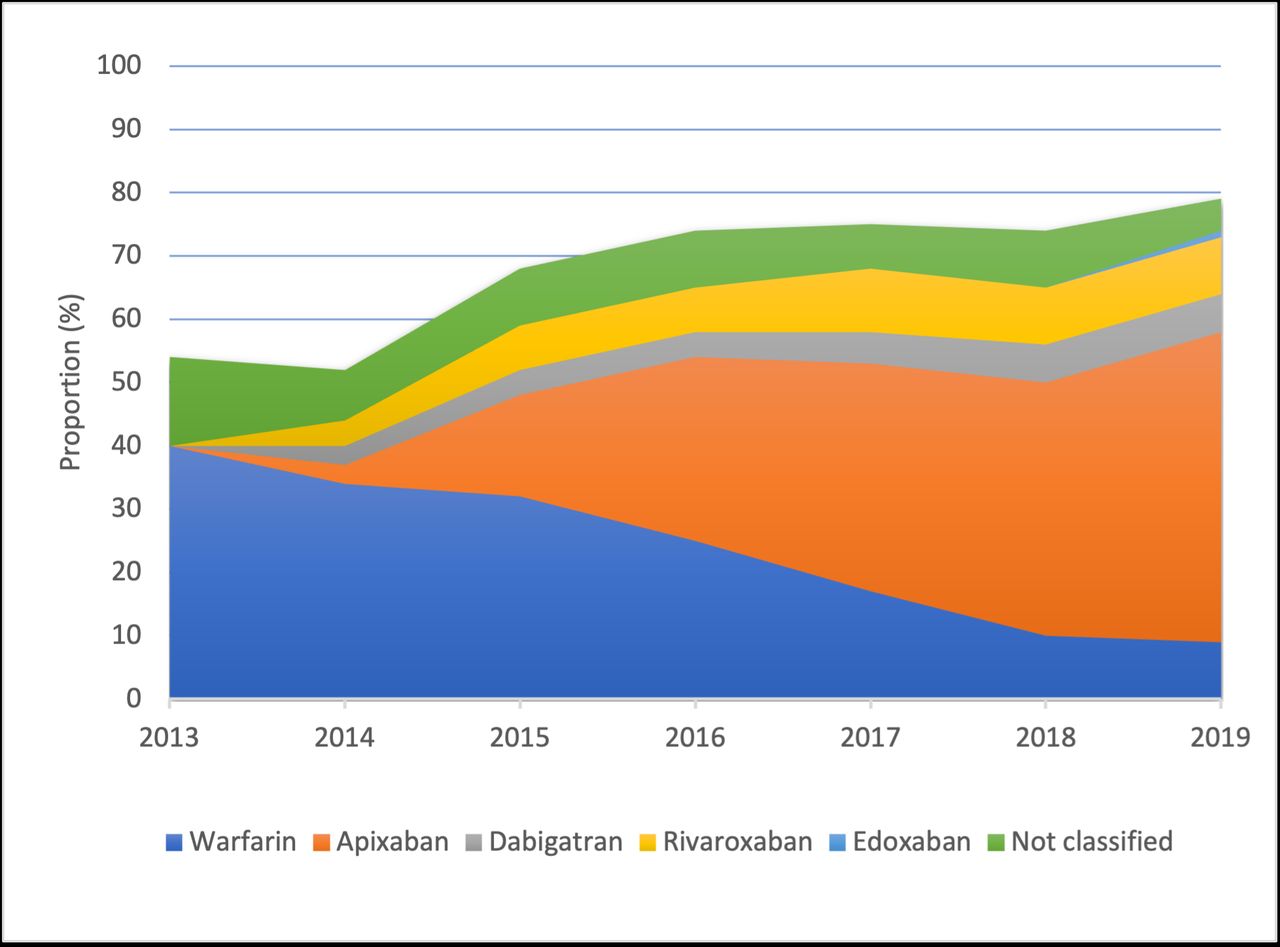
Prescription of different anticoagulation drugs after hospitalisation for acute myocardial infarction in patients with atrial fibrillation, Norway 2013–2019.
Single antiplatelet therapy and dual antiplatelet therapy in combination with anticoagulation therapy were prescribed to 3323 (46.3%) and 1753 (24.4%) of the 7174 patients discharged alive with MI, AF and CHA2DS2-VASc risk score ≥2, respectively.
Event-free survival
Patients were followed up for a median duration of 639 days (25th, 75th percentile 183, 1339).
A total of 1343 (57.4%) patients with AF and CHA2DS2-VASc risk score ≥2 discharged alive from hospital after MI without anticoagulation therapy died or suffered a stroke during follow-up, while 2167 (45.1%) patients discharged with anticoagulation therapy died and/or suffered a stroke (table 2). Patients prescribed anticoagulation therapy had a reduced risk of all types of stroke or death (multivariate-adjusted HR 0.8, 95% CI 0.7 to 0.8, p<0.001) compared with patients without a prescription of anticoagulation therapy (figure 4). Subdistribution HR for non-fatal stroke (all type) with all cause death as competing event was 0.8 (95% CI 0.6 to 1.1, p=0.116) for patients with versus patients without a prescription of anticoagulation therapy.
Long-term outcomes* in patients with myocardial infarction, atrial fibrillation and CHA2DS2-VASc risk score ≥2, Norway 2013–2019, n=7174

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Event-free survival in patients with myocardial infarction and atrial fibrillation, Norway 2013–2019.
Discussion
In this nationwide study of patients with acute MI admitted to hospitals in Norway from 2013 to 2019, the prevalence of ECG-verified AF at hospitalisation was 10.9%. Of 47.2% of the patients with AF and CHA2DS2-VASc risk score ≥2 used anticoagulation therapy prior to the MI, and 67.0% of the patients with CHA2DS2-VASc risk score ≥2 discharged alive were prescribed anticoagulation therapy. The prescription rate of anticoagulation therapy increased with 6.0% per year during the study period, from 55% in 2013 to 78% in 2019. Patients without prescription of anticoagulation therapy at hospital discharge had increased risk of stroke (all types) or all-cause death compared with patients with anticoagulation therapy.
More than half of the patients with AF at hospitalisation in this study were not treated with anticoagulation therapy prior to the MI. AF confers a fivefold increased risk of stroke on average, and 20%–30% of all strokes are attributed to this arrhythmia.4 Anticoagulation therapy effectively reduces the risk of stroke, but low prescription rates of anticoagulation therapy have repeatedly been reported.4–7 13 14 Up to one-third of AF cases are undiagnosed due to the asymptomatic and intermittent nature of AF.4 15 The ESC guideline recommends screening for AF in patients at increased risk of stroke and AF screening is cost-effective in the high-risk population.4 16 However, there is currently limited long-term continuous ECG recording equipment available that is suitable, affordable and sufficiently easy to use for screening purposes.17 New and more effective diagnostic tools to identify AF will probably be more generally available in the future.18
Acute MI confers an excess risk of thromboembolic complications in patients with AF.19 The ESC guidelines recommend anticoagulation therapy in most patients with AF and MI (ie, patients with CHA2DS2-VASc risk score ≥2).4 20 21 Although the proportion of patients prescribed anticoagulation therapy increased significantly during the study period, many patients were discharged from hospital without such treatment. The combination of antiplatelet drugs with anticoagulation therapy results in twofold to threefold increase in risk of bleeding complications, and the choice of antithrombotic treatment requires careful consideration of stroke risk, the risk of a new MI and the risk of bleeding.22 23 Many patients with MI and AF are old, have additional comorbidities and consequently increased risk of death and stroke due to other reasons as well as increased bleeding risk, probably explaining the reduced utilisation of guideline-recommended therapy.
Several studies have described increased risk of stroke and death after MI in patients with AF compared with MI in patients without AF.24 Warfarin effectively reduces the risk of stroke and mortality in patients with AF, but its use is limited by the narrow therapeutic interval.25 26 NOACs are associated with a similar, or even larger, reduction in risk of stroke as warfarin, and also lower risk of major bleeding.27 Despite NOAC is recommended in the guidelines, as many as 9% of the patients discharged with anticoagulation therapy were prescribed warfarin in 2019. The observed shift in treatment from warfarin to NOACs in this study is probably part of the explanation for the increased use of anticoagulation therapy. Improved outcome in patients prescribed anticoagulation therapy compared with patients without anticoagulation therapy in this study highlights the importance of adherence to international guidelines in treatment of patients with MI and AF.
The main strengths of this study are the large and unselected population comprising nearly all patients hospitalised with MI in Norway from 2013 to 2019, and a nearly complete follow-up. However, there are several important limitations associated with the study design and the NORMI. This study was an observational study, making it impossible to demonstrate causal associations between treatment and outcomes. Only MIs that led to hospitalisation were registered in the NORMI. A few hospitals did not deliver complete data for the whole period, but the coverage compared with the Norwegian Patient Register was >90%.10 The NORMI did not have complete coverage for all variables. We only obtained deidentified data from the NORMI and the Norwegian Cardiovascular Disease Registry and could not verify the information through medical records at the individual patient level. The NORMI does not have all the necessary variables to calculate the risk of bleeding and fraility.28 29 Furthermore, drug dosages and drug compliance of anticoagulation therapy after discharge from hospitals were not available. Consequently, we have only been able to adjust for a limited number of covariates. Unmeasured confounders still exist. The findings of the study must be interpreted with caution and generalisation of the results should be avoided.
In conclusion, the prescription rate of anticoagulation therapy in patients with MI and AF with an indication for anticoagulation therapy increased during the study period. However, still many patients with MI and AF did not receive guidelines recommended treatment with anticoagulation therapy and had a higher risk of stroke or death during follow-up. This study highlights an area with potential for improvement in the treatment of acute MI.
Data availability statement
Data may be obtained from a third party and are not publicly available. The data underlying this article were provided by the Norwegian Institute of Public Health under licence/by permission. Data will be shared on request to the corresponding author with permission of the Norwegian Institute of Public Health.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by The Norwegian Regional Committee for Medical and Health Research Ethics North (REK 2016/170). This study used existing data from Norwegian national health registries. Registration into these registries is mandatory (the Norwegian Cardiovascular Disease Registry Regulation and the Norwegian Health Register Act), and consent by the patient was not required.
References
Footnotes
Contributors JJ accepts full responsibility as guarantor for the finished work, had access to the data, and controlled the decision to publish. JJ and SH were responsible for the conception of the study, and the analysis and interpretation of data. JJ drafted the manuscript. AHP contributed to the analysis and interpretation of the data and critically revised the manuscript. ELS critically revised the manuscript. All gave final approval and agreed to be accountable for all aspects of work ensuring its integrity and accuracy.
Funding This work was supported by South-Eastern Norway Regional Health Authority, Hamar, Norway.
Disclaimer The funder has no role in the design and conduct of the study, in the collection, analysis, and interpretation of the data, and in the preparation, review, or approval of the manuscript.
Competing interests JJ has received speaking fees from Amgen, AstraZeneca, BMS, Boehringer Ingelheim, Novartis, Pfizer and Sanofi. He is shareholder in Appsens AS and is employed in the company. ELS has received speaking fees from Pfizer. AHP has no conflicts of interest. SH has received speaking fees from Boehringer Ingelheim, BMS, Pfizer and Sanofi.
Provenance and peer review Not commissioned; externally peer reviewed.