Article Text

Abstract
Objective Patients with low-flow, low-gradient aortic stenosis (LFLG AS) and reduced left ventricular ejection fraction (LVEF) are known to suffer from poor prognosis after transcatheter aortic valve implantation (TAVI). This study aimed to develop a simple score system for risk prediction in this vulnerable subset of patients.
Methods All patients with LFLG AS with reduced EF and sufficient CT data for aortic valve calcification (AVC) quantification, who underwent TAVI at five German centres, were retrospectively included. The Risk prEdiction in patients with Low Ejection Fraction low gradient aortic stenosis undergoing TAVI (RELiEF TAVI) score was developed based on multivariable Cox regression for all-cause mortality.
Results Among all included patients (n=718), RELiEF TAVI score variables were defined as independent predictors of mortality: male sex (HR 1.34 (1.06, 1.68), p=0.013), underweight (HR 3.10 (1.50, 6.40), p=0.0022), chronic obstructive pulmonary disease (HR 1.55 (1.21, 1.99), p=0.001), pulmonary hypertension (HR 1.51 (1.17, 1.94), p=0.0015), atrial fibrillation (HR 1.28 (1.03, 1.60), p=0.028), stroke volume index (HR 0.96 (0.95, 0.98), p<0.001), non-transfemoral access (HR 1.36 (1.05, 1.76), p=0.021) and low AVC density (HR 1.44 (1.15, 1.79), p=0.0012). A score system was developed ranging from 0 to 12 points (risk of 1-year mortality: 13%–99%). Kaplan-Meier analysis for low (0–1 points), moderate (2–4 points) and high RELiEF TAVI score (>4 points) demonstrated rates of 18.0%, 29.0% and 46.1% (p<0.001) for all-cause mortality and 23.8%, 35.9% and 53.4% (p<0.001) for the combined endpoint of all-cause mortality or heart failure rehospitalisation after 1 year, respectively.
Conclusions The RELiEF TAVI score is based on simple clinical, echocardiographic and CT parameters and might serve as a helpful tool for risk prediction in patients with LFLG AS and reduced LVEF scheduled for TAVI.
- transcatheter aortic valve replacement
- aortic valve stenosis
- echocardiography
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known about this subject?
Patients with low-flow, low-gradient aortic stenosis (LFLG AS) and reduced left ventricular ejection fraction (LVEF) suffer from poor prognosis after transcatheter aortic valve implantation (TAVI), especially when compared with patients with high-gradient AS. However, data on strong predictors of outcome in this complex subset of patients are scarce.
What does this study add?
Based on a large retrospective registry, the present study was able to define simple clinical, echocardiographic and CT parameters at baseline, that were independently associated with adverse outcome of patients with LFLG AS and reduced LVEF after TAVI. By integrating these parameters, the The Risk prEdiction in patients with Low Ejection Fraction low gradient aortic stenosis undergoing TAVI (RELiEF TAVI) score was developed as a tool for risk discrimination in patients with LFLG AS and reduced LVEF scheduled for intervention.
How might this impact on clinical practice?
The RELiEF TAVI score consists of simple baseline clinical, echocardiographic and CT parameters and might help identify patients with acceptable outcome after TAVI within the vulnerable subset of patients with LFLG AS and reduced LVEF. Moreover, it might be used as a tool to identify those patients, in whom TAVI may be considered futile. Consequently, the RELiEF TAVI score may facilitate decision-making in patients with LFLG AS and reduced LVEF.
Introduction
For the majority of patients with severe symptomatic aortic stenosis (AS), transcatheter aortic valve implantation (TAVI) has become the standard therapy within recent years.1 According to the 2021 European Society of Cardiology/European Association for Cardio-Thoracic Surgery guidelines for the management of valvular heart disease, severe AS can be categorised into different subtypes with respect to the transvalvular gradient (Pmean), the flow status across the aortic valve (as assessed by stroke volume index (SVI)) and left ventricular ejection fraction (LVEF).2 While patients with high-gradient AS (Pmean ≥40 mm Hg) experience the largest benefit after TAVI, those with low-flow, low-gradient (LFLG) AS and reduced LVEF (Pmean <40 mm Hg, aortic valve area (AVA) ≤1 cm², LVEF <50%, SVI ≤35 mL/m²) have a markedly poorer prognosis with mortality rates of 30%–50% or higher already at 2 years after treatment.3–6 Consequently, clinical decision-making in these patients is challenging because strong predictors of outcome following TAVI for this subset of patients have not yet been adequately determined.
The aim of the current study was to develop a simple score system for risk prediction based on clinical, echocardiographic and CT parameters at baseline derived from a large multicentre cohort of patients with LFLG AS and reduced LVEF undergoing TAVI (Risk prEdiction in patients with Low Ejection Fraction low gradient aortic stenosis undergoing TAVI (RELiEF TAVI) score).
Material and methods
Study design and data acquisition
The study was designed as a retrospective analysis of data derived from five German high-volume TAVI centres. All clinical endpoints were adjudicated according to the Valve Academic Research Consortium-2 (VARC-2) criteria after 30 days. Echocardiographic outcome was derived from in-house transthoracic echocardiography (TTE) at discharge. Survival data were obtained from in-house information as part of clinical routine follow-up. All patients provided informed consent to the procedure and data acquisition. It was not appropriate or possible to involve patients or the public in the design, or conduct, or reporting, or dissemination plans of our research. The study was approved by the local institutional review boards and performed in accordance with the declaration of Helsinki.
Study population
Between 2008 and 2019, a total of 9150 patients were treated with TAVI at all participating TAVI centres. For all patients, the decision to perform TAVI was made by an interdisciplinary heart team. After excluding patients who underwent planned valve-in-valve procedures, combined percutaneous mitral valve treatment, patients treated with investigational transcatheter heart valves (THVs) and those with insufficient CT data for the quantification of aortic valve calcification (AVC), we identified 718 patients fulfilling the echocardiographic criteria for severe LFLG AS with reduced LVEF.
Study endpoints
The primary endpoint was defined as all-cause mortality after 1 year. Secondary endpoints were cardiovascular mortality and a combined endpoint of all-cause mortality or heart failure (HF) rehospitalisation after 1 year.
Definition of LFLG AS with reduced ejection fraction
Severe LFLG AS with reduced LVEF was defined as an AVA ≤1.0 cm2, transvalvular gradient <40 mm Hg, SVI ≤35 mL/m2 and LVEF <50% assessed by means of resting TTE. AVAs were calculated by using the continuity equation.7 SVI was calculated by means of cross-sectional left ventricular outflow tract (LVOT) area and LVOT velocity time integral.2
CT measurements
Quantification of AVC was performed by calcium volume scoring on contrast-enhanced CT images using a dedicated software (3mensio Structural Heart V9.1, Pie Medical Imaging, Maastricht, Netherlands). An empirical threshold of 550 Hounsfield units (HU) was used for AVC assessment in the majority of patients for the purpose of discrimination between calcium and contrast medium. The threshold was only adjusted in exceptional cases in order to properly distinguish calcium from contrast agent. Calcification was separately assessed in the annular plane and the LVOT, as described before.8 AVC was defined as the total calcium volume detected in the annular plane sector. AVC density (AVCd) was defined as the ratio of AVC (mm3 calcium) per aortic annulus area (cm2). Distribution of AVCd measurements for each centre is demonstrated by density curves in online supplemental figure S1. Low AVCd was defined as the lowest sex-specific AVCd tertile in the derivation cohort, that is, AVCd ≤62.45 mm3 calcium/cm2 for male patients and AVCd ≤51.04 mm3 calcium/cm2 for female patients. Calcification of the LVOT was assessed separately. Low LVOT calcification was defined as LVOT calcium load ≤10 mm3, as described before.9
Supplemental material

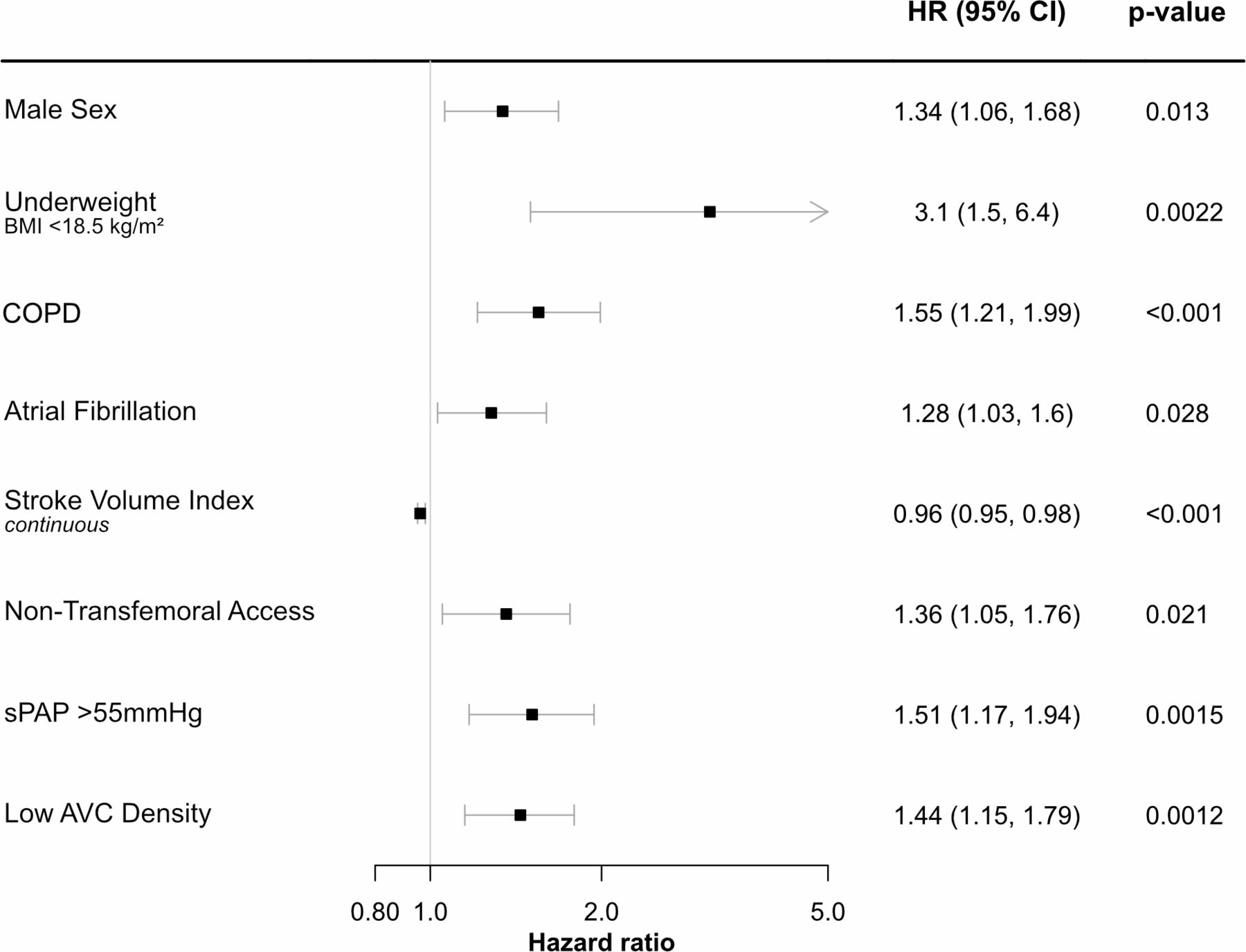
Forest plot for all independent predictors of outcome. HRs for all-cause mortality after multivariable adjustment. AVC, aortic valve calcification; BMI, body mass index; COPD, chronic obstructive pulmonary disease; sPAP, systolic pulmonary artery pressure.
Statistical analysis
Sex-specific AVCd tertiles were calculated in the overall study population. Boundaries for sex-specific AVCd tertiles are given in online supplemental table S1. Variables entering the score system were selected in a two-step selection process. Variables that showed p values <0.1 in the univariable Cox regression analysis (1) were used in a forward selection process based on Akaike Information Criteria (2). The variables of the best performing multivariable model were used for risk score calculation. In order to assign risk points to the selected variables and to predict mortality rates by risk score points, we followed the method used by the Framingham Heart Study. One score point was reflected by 0.29 regression units. Underweight was defined as body mass index (BMI) <18.5 kg/m2.10
For validation, a bootstrap correction with 500 bootstraps was performed. Survival curves were produced using the Kaplan-Meier method and curve differences were tested using the log-rank test. Model performance was assessed by calibration and discrimination. The c-index for all endpoints was calculated for the RELiEF TAVI score and for an established risk score system, the European System for Cardiac Operative Risk Evaluation (EuroSCORE) II.11 All statistical analyses were performed using R V.4.0.3 (R Foundation for Statistical Computing, Vienna, Austria).
Results
Baseline characteristics and outcomes
Clinical, echocardiographic and CT baseline parameters as well as procedural characteristics and outcome data of the overall study population (n=718) are given in table 1. The investigated patients were predominantly men and of advanced age with a median of 81.0 years (IQR 76.4, 84.7). Cardiovascular comorbidities (ie, atrial fibrillation, severe pulmonary hypertension, prior myocardial infarction, prior stroke or extracardiac arteriopathy) and non-cardiovascular comorbidities (ie, chronic obstructive pulmonary disease (COPD), diabetes or impaired renal function) were present in a large proportion of the study population, translating into elevated surgical risk (EuroSCORE II 7.0% (IQR 4.1, 12.4)). Of note, 21.5% of the overall study population presented with New York Heart Association (NYHA) functional class IV. The majority of patients was treated via transfemoral access (83.1%) with either balloon-expandable (40.9%) or self-expandable (55.8%) THVs. Additional procedural data and outcomes are given in online supplemental table S2.
Baseline characteristics, procedural aspects and outcomes
30-Day VARC-2 and late clinical outcomes
Within 30 days after TAVI, disabling stroke, major or life-threatening bleeding, need for new pacemaker implantation or ≥moderate paravalvular leakage occurred in 2.6%, 9.5%, 13.6% and 4.3% of the patients. Procedural and 30-day mortality rates were 1.1% and 7.7%, respectively (table 1). Over the median follow-up time of 2.95 (95% CI 2.66 to 3.21) years, death occurred in 371 cases. Cardiovascular death and HF rehospitalisation occurred in 84 and 126 patients, respectively. Among the study population all-cause mortality rate 1 year after TAVI was 29.1%.
RELiEF TAVI score development
Uni- and multivariable Cox regression analyses for all-cause mortality in the total patient population as well as score point assignment are given in table 2. After multivariable analysis male sex (HR 1.34 (95% confidence interval (CI): 1.06 to 1.68), p=0.013), underweight (HR 3.10 (95% CI: 1.50 to 6.40), p=0.0022), COPD (HR 1.55 (95% CI: 1.21 to 1.99), p<0.001), pulmonary hypertension >55 mm Hg (HR 1.51 (95% CI: 1.17 to 1.94), p=0.0015), atrial fibrillation (HR 1.28 (95% CI: 1.03 to 1.60), p=0.028), non-transfemoral access (HR 1.36 (95% CI: 1.05 to 1.76), p=0.021) and low AVCd (HR 1.44 (95% CI: 1.15 to 1.79), p=0.0012) remained independent predictors of mortality, while SVI (continuous) (HR 0.96 (95% CI: 0.95 to 0.98), p<0.001) was independently predictive of survival. Figure 1 shows a forest plot for all independent predictors of outcome.
Univariable and multivariable Cox proportional regression analysis for all-cause mortality and RELiEF TAVI score development
All parameters included in this multivariable Cox regression model were selected as score variables and, according to their predictive weight, score points were assigned to each score variable: Male sex (one point), COPD (two points), atrial fibrillation (one point), underweight (BMI <18.5 kg/m2) (four points), low SVI (≤24.9 mL/m²) (one point), pulmonary hypertension >55 mm Hg (one point), low AVCd (male: ≤62.45 mm3 calcium/cm2; female: ≤51.04 mm3 calcium/cm2) (one point) and non-transfemoral access (one point). The RELiEF TAVI score is summarised in figure 2 and ranges from 0 (estimated risk of 1-year mortality: 13%) to 12 points (estimated risk of 1-year mortality: 99%). Online supplemental figure S2 depicts the distribution of score points across the study population.
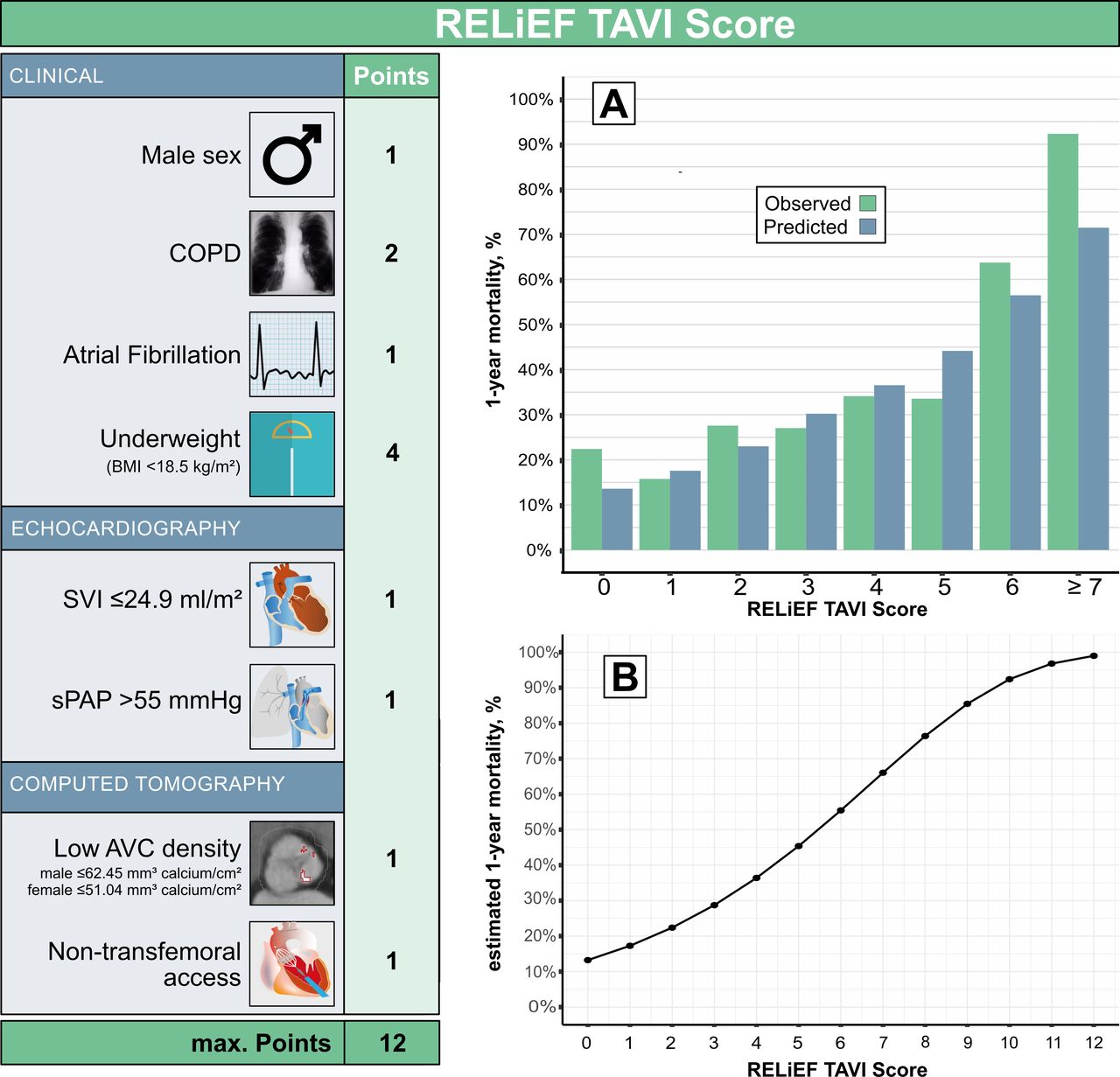
The RELiEF TAVI score. Variables, score point assignment and prediction of 1-year all-cause mortality risk. AVC, aortic valve calcification; BMI, body mass index; COPD, chronic obstructive pulmonary disease; RELiEF TAVI, Risk prEdiction in patients with Low Ejection Fraction low gradient aortic stenosis undergoing TAVI; sPAP, systolic pulmonary artery pressure; SVI, stroke volume index; TAVI, transcatheter aortic valve implantation.
Risk discrimination
Figure 3 demonstrates predicted mortality by the RELiEF TAVI score and observed mortality for each score point in the study population. While observed 1-year mortality in study patients with 0 points was 22.4%, mortality after 1 year reached 92.3% in study patients with 7 or more RELiEF TAVI score points. All patients with more than 7 points died within 1 year after TAVI.

Observed mortality and predicted 1-year all-cause mortality by the RELiEF TAVI score. RELiEF TAVI, Risk prEdiction in patients with Low Ejection Fraction low gradient aortic stenosis undergoing TAVI; TAVI, transcatheter aortic valve implantation.
Kaplan-Meier analyses for the primary endpoint of all-cause mortality after 1 year as well as the secondary endpoint of cardiovascular mortality after 1 year and the combined endpoint of all-cause mortality or HF rehospitalisation after 1 year are given in figure 4 according to low (0–1 points), moderate (2–4 points) and high RELiEF TAVI score (>4 points).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Kaplan-Meier analysis for different study endpoints according to low (0–1 points), moderate (2–4 points) and high RELiEF TAVI score (>4 points). (A) 1-year all-cause mortality, (B) 1-year cardiovascular mortality, (C) 1-year all-cause mortality or HF hospitalisation. HF, heart failure; RELiEF TAVI, Risk prEdiction in patients with Low Ejection Fraction low gradient aortic stenosis undergoing TAVI; TAVI, transcatheter aortic valve implantation.
Regarding the primary endpoint, patients with high RELiEF TAVI score had the highest 1-year all-cause mortality rate compared with patients with moderate or low RELiEF TAVI score (46.1% vs 29.0% vs 18.0%, p<0.001). Log-rank tests for post hoc pairwise comparisons also demonstrated significant differences in mortality rates between low versus moderate RELiEF TAVI score (p=0.0058), moderate versus high RELiEF TAVI score (p<0.001) and low versus high RELiEF TAVI score (p<0.001) (figure 4A).
The secondary endpoint of cardiovascular mortality after 1 year and the combined endpoint of all-cause mortality or HF rehospitalisation after 1 year also occurred significantly more often in patients with high RELiEF TAVI score (29.3% and 53.4%) compared with patients with moderate (16.2% and 35.9%) or low (7.0% and 23.8%) RELiEF TAVI score (p<0.001 for both endpoints) (figure 4B,C).
Risk prediction
The c-index of the RELiEF TAVI score was 0.62 (95% CI: 0.59 to 0.68) for all-cause mortality, 0.66 (95% CI: 0.61 to 0.75) for cardiovascular mortality, 0.64 (95% CI: 0.55 to 0.70) for HF rehospitalisation and 0.61 (95% CI: 0.57 to 0.66) for the combined endpoint of all-cause mortality or HF rehospitalisation, all after 1 year. After internal bootstrap validation, c-indices of the RELiEF TAVI score were 0.60 (95% CI: 0.57 to 0.66) for all-cause mortality, 0.64 (95% CI: 0.59 to 0.73) for cardiovascular mortality, 0.63 (95% CI: 0.54 to 0.59) for HF rehospitalisation and 0.59 (95% CI: 0.56 to 0.64) for the combined endpoint after 1 year. Compared with the established EuroSCORE II, the RELiEF TAVI score was superior regarding the prediction of all-cause mortality (EuroSCORE II: 0.57 (95% CI: 0.52 to 0.61)), HF rehospitalisation (EuroSCORE II: 0.58 (95% CI: 0.48 to 0.66)) and the combined endpoint (EuroSCORE II: 0.56 (95% CI: 0.53 to 0.60)), but not regarding cardiovascular mortality (EuroSCORE II: 0.70 (95% CI: 0.63 to 0.77)).
Discussion
In the present study, which comprises a large multicentre dataset of patients with LFLG AS and reduced LVEF undergoing TAVI, a simple risk score system (RELiEF TAVI score) based on clinical, echocardiographic and CT parameters was developed and internally validated.
Characteristics of patients with LFLG AS and reduced LVEF undergoing TAVI
The limited prognosis of TAVI patients with LFLG AS and reduced LVEF has been shown in several previous studies. According to these data, patients presenting with LFLG AS and reduced LVEF suffer from a vast burden of cardiac as well as non-cardiac comorbidities.3–6 This is also demonstrated in the present study as a large proportion of patients presented with LVEF <30%, NYHA functional class IV, prior myocardial infarction, atrial fibrillation, concomitant mitral and tricuspid regurgitation, pulmonary hypertension, diabetes mellitus as well as peripheral artery and pulmonary disease. Although the rate of device success was high and procedural complication rates were low, all-cause mortality at 30 days and 12 months in the current study was still high with 7.3% and 29.1%, respectively. Thus, in contrast to the universal trend to perform TAVI in patients with AS at lower risk, the subset of patients with LFLG AS and reduced LVEF clearly remains a high-risk population, in whom—compared with patients with non-LFLG AS—excess mortality after TAVI has to be anticipated.12 13
Outcome predictors in patients with LFLG AS and reduced LVEF undergoing TAVI
Outcome predictors among TAVI patients with LFLG AS and reduced LVEF have so far been assessed in national and international registries. By using data from the German Aortic Valve Registry, a prospective national registry including a total of 359 patients with LFLG AS and reduced LVEF that underwent TAVI, Lauten et al found peripheral artery disease, pulmonary hypertension and prior myocardial infarction to be independent predictors of mortality among patients with LFLG AS and reduced LVEF.5 The FRANCE 2 registry is a French national TAVI registry, that included 502 patients with LFLG AS and reduced LVEF. Amabile et al found that transapical access, pre-TAVI angina, advanced kidney failure, atrial fibrillation and moderate to severe aortic regurgitation after TAVI were independent outcome predictors in patients with LFLG AS and reduced LVEF included in the FRANCE 2 registry.14 In contrast to our study, in both national registries, SVI was not integrated in LFLG AS definition and neither CT nor dobutamine stress echocardiography (DSE) data were available for analysis. Moreover, the number of patients with LFLG AS and reduced LVEF was substantially higher in the present study (n=718). The True or Pseudo-severe Aortic Stenosis (TOPAS) registry is a prospective multicentric study including a total of 287 patients with LFLG AS and reduced LVEF undergoing TAVI. Of these, 234 patients underwent DSE prior to TAVI. Independent outcome predictors after TAVI in the TOPAS registry were COPD and low haemoglobin levels.3 Substudies of the TOPAS study identified right ventricular dysfunction and tricuspid regurgitation as important factors limiting prognosis of patients with LFLG AS and reduced LVEF.15 16 The present study, however, comprises a larger patient cohort compared with the TOPAS registry and represents the first analysis including both, SVI and AVC burden as assessed by CT. Beside male sex, we identified COPD, underweight, atrial fibrillation, pulmonary hypertension, non-transfemoral access, low AVCd and low SVI to be independently associated with mortality. The adverse impact of each of these variables on outcomes in the general TAVI population has been well described.3 8 17–22 Low SVI, atrial fibrillation, pulmonary hypertension and COPD may be interpreted as surrogates for advanced chronic cardiac and non-cardiac illness, whereas non-transfemoral access is a marker for increased procedural risk. Underweight in elderly patients is a known surrogate parameter for frailty and has been associated with inferior outcome.23 In contrast, AVCd is a diagnostic parameter, which strongly correlates with AS severity.24 25 Since it is completely independent from transvalvular flow, its diagnostic value has been described particularly for patients with LFLG AS and reduced LVEF.26 27 In a study investigating outcomes of medically managed patients with severe AS, high AVCd was independently associated with excess mortality.28 Conversely, in a recent publication of patients with LFLG AS and reduced LVEF treated with TAVI, we showed that patients with high AVCd experience larger benefits compared with patients with low AVCd.8 Hence, the therapeutic benefit of eliminating AS with TAVI might be less pronounced in patients with low AVCd. The present study confirms the diagnostic and prognostic importance of CT based AVC assessment in patients with LFLG AS and reduced LVEF.
Clinical value of the RELiEF TAVI score
Based on simple clinical, echocardiographic and CT baseline parameters, we developed a new score system for the prediction of outcome in patients with LFLG AS and reduced LVEF scheduled for TAVI. In the present study, patients with LFLG AS and reduced LVEF with high RELiEF TAVI score (>4 points) had a more than twofold increase in all-cause mortality or HF hospitalisations, a more than 2.5-fold increase in all-cause mortality alone and a fourfold increase in cardiovascular mortality at 1 year after TAVI compared with those with low RELiEF TAVI score (0–1 points). Moreover, the RELiEF TAVI score was superior the established EuroSCORE II regarding risk prediction of all-cause mortality and HF readmissions and provided a reasonable discriminative performance with only minor discrepancies between score-predicted and observed mortality rates. Given these results, the RELiEF TAVI score may serve as an additional tool to guide clinical decision-making in patients with LFLG AS and reduced LVEF. An important limitation of the present study is that we cannot provide data on medically treated patients with LFLG AS, which would allow for a comparison between TAVI and the natural course of AS in this high-risk patient population. Yet, in patients with a RELiEF TAVI score 7 or more, accounting for less than 2% of the total study cohort, the mortality rate 1 year after TAVI was in excess of 90%. In such patients, who are at advanced stages of cardiac and non-cardiac comorbidities and present with only borderline AS according to CT (eg, according to guideline-supported thresholds (non-contrast CT) or, if unavailable, according to presented AVCd tertiles (contrast-enhanced CT)), treatment with TAVI may be considered futile, since these patients are very unlikely to experience prognostic benefit from the procedure. The majority of patients with LFLG AS and reduced LVEF, however, presents with low (22.9%) or moderate RELiEF TAVI score (62.2%), has a markedly better prognosis and, thus, is more likely to benefit from TAVI. This assumption is supported by data from a post hoc analysis of the randomised Partner A trial showing that TAVI improves outcome in the overall patient cohort with LFLG AS and reduced LVEF compared with medical treatment alone.4 Moreover, the ongoing TAVR UNLOAD randomised controlled trial (NCT02661451), comparing TAVI with medical therapy in patients with moderate AS and systolic HF, will shed even more light on the optimal treatment strategy for patients with LFLG AS and reduced LVEF.29
Limitations
There are several limitations inherent in the present analysis in addition to its retrospective design. First, AVCd was quantified by using contrast-enhanced CT images. The presented sex-specific prognostic cut-offs for low AVCd may therefore underlie certain restrictions. Second, another limitation of this study is the lack of a medically treated control group of patients with LFLG AS. Future studies will have to verify our results by using non-contrast CT images and including medically treated patients with LFLG AS. Third, the main limitation of our study remains that DSE was not part of the routine assessment for LFLG AS severity. Hence, we cannot rule out that patients with pseudo-severe AS were included in the study population. Therefore, it might be possible that low AVCd represents a surrogate parameter of pseudo-severe AS and that its adverse impact on outcome could have been partially foreseen by unveiling pseudo-severe AS with DSE. However, as contractile reserve is only present in about half of patients with LFLG AS and reduced LVEF, DSE is often non-diagnostic and guideline-recommended DSE cut-offs like peak stress Pmean ≥40 mm Hg or peak stress AVA ≤1.0 cm2 have failed to predict outcome among patients with LFLG AS and reduced LVEF under medical treatment.3 30 Moreover, there is accumulating data supporting that aortic valve replacement may be beneficial in patients with pseudo-severe AS, which might further weaken the importance of DSE in patients with LFLG AS and reduced LVEF.31 Fourth, the inclusion of baseline laboratory parameters (ie, NT-proBNP or troponin) into score systems for risk prediction in patients with LFLG AS and reduced LVEF represents an interesting approach, which was not practicable for the present study.
Conclusions
Based on data from a large multicentre registry, the RELiEF TAVI score is a novel risk prediction tool for patients with LFLG AS and reduced LVEF scheduled for TAVI. The score consists of simple clinical, echocardiographic and CT parameters at baseline and may help identify patients with LFLG AS and reduced LVEF at high risk for mortality or cardiovascular events after TAVI. The RELiEF TAVI score could serve as an important tool to facilitate decision-making in this complex subset of patients with AS.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by Ethik-Kommission der Ärztekammer Hamburg, ID: PV4304 Participants gave informed consent to participate in the study before taking part.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @SebLudwig1
Contributors SL and NS are responsible for the overall content. SL is acting as guarantor. SL and NS contributed to conceptualisation. SL, AG and NS contributed to methodology. AG contributed to formal analysis. SL, AG, MS, DW, J-MS, AS, MA, VM, DF, HS, TR, MP, LC, NS contributed to investigation, resources, data curation. SL and NS contributed to original manuscript preparation. AG, MS, DW, J-MS, AS, MA, VM, DF, HS, TR, MP, LC contributed to manuscript review and editing. SL and AG contributed to visualisation.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests SL reports non-financial support from Edwards Lifesciences. MS reports non-financial support from Abbott Vascular, Biotronik, Boehringer Ingelheim, Boston Scientific, Edwards Lifesciences, Nicolai Medizintechnik, OrbusNeich Medical, personal fees from Abiomed, Amgen, AstraZeneca, Bayer Healthcare, Bristol-Myers Squibb, Boston Scientific, Medtronic, Philips and Shockwave Medical, grants from Philips. DW reports personal fees from AstraZeneca, Bayer, Berlin-Chemie and Novartis. J-MS is proctor for Medtronic and Boston Scientific, received research grants and speaker honoraria from Edwards Lifesciences, Medtronic and Boston Scientific. DF is consultant for Edwards Lifesciences and Medtronic and received research funding from Edwards Lifesciences. TR received speaker honoraria from Boston Scientific, Edwards, Medtronic, Abbott. LC is proctor and consultant for Edwards Lifesciences and Boston Scientific and consultant for Medtronic and Abbott Vascular. NS reports personal fees from Boston Scientific and non-financial support from Abbott and Edwards Lifesciences.
Provenance and peer review Not commissioned; internally peer reviewed.