Article Text

Abstract
Objective Left ventricular non-compaction (LVNC) is morphologically characterised by excessive trabeculations and deep recesses in the ventricular wall. The risk of thromboembolic disease in the paediatric patients with LVNC has not been clearly established. We conducted this systematic review to evaluate the prevalence and incidence of thromboembolism (TE) in paediatric and adult patients with LVNC and searched for risk factors for TE to explore management strategies.
Methods The primary outcome was the prevalence and incidence of TE in the patients with LVNC. The secondary outcome was the TE and mortality and heart transplantation rates between paediatric and adult patients with LVNC. We searched for studies published in MEDLINE, Embase and Cochrane Central Register of Controlled Trials between January 1950 and December 2020. A systematic search of keywords related to LVNC, anticoagulants/antiplatelets and TE was conducted. Studies that did not present original research, non-human studies, duplicated studies were excluded.
Results Fifty-seven studies met the inclusion criteria. A total of 726 paediatric and 3862 adult patients were included. The mean prevalence rates of TE in the paediatric and adult patients with LVNC were 2.6% and 6.2% (I2=0%; p<0.450 and I2=73.7%; p<0.001), respectively. The mean annual incidences of TE in paediatric and adult patients with LVNC were 1.4% and 2.9% (I2=99.4%; p<0.001 and I2=99.5%; p<0.001), respectively. Multivariate logistic regression analysis showed that TE was associated with left ventricular ejection fraction in <40% of paediatric patients (OR, 9.47; 95% CI, 1.35 to 188.23; p=0.0225).
Conclusions The prevalence and incidence rates in paediatric patients were lower than those in adult patients. TE was associated with a reduced systolic function in paediatric patients with LVNC.
- cardiomyopathies
- heart failure
- systematic reviews as topic
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Long-term outcomes of patients with left ventricular non-compaction (LVNC) are influenced by the degree of heart failure and the presence of life-threatening arrhythmias and thromboembolism. Several studies have reported that children with cardiomyopathy have an increased risk of potentially fatal thrombosis.
WHAT THIS STUDY ADDS
This is the first systematic review of thromboembolic events in LVNC. In this study, 2.6% of paediatric patients with LVNC experienced thromboembolic events, which were associated with reduced left ventricular systolic function.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE AND/OR POLICY
Anticoagulants or antiplatelets may be considered an option in those with depressed left ventricular systolic function in paediatric patients with LVNC.
Introduction
Left ventricular non-compaction (LVNC) is a type of cardiomyopathy that is morphologically characterised by excessive trabeculations and deep recesses in the ventricular wall.1 Its two-layered structure comprises a thick non-compacted layer on the endocardial side and a thin compacted layer on the epicardial side.1 The incidence of LVNC was estimated to be 0.0001%–0.0008% in children.2 In adults who underwent echocardiography, the prevalence of LVNC was reported to be 0.05%–0.14%.3 4 The clinical manifestations of LVNC vary widely from neonates to adults, which range from asymptomatic cases to end-stage heart failure (HF), potentially necessitating mechanical circulatory support and/or cardiac transplantation.5–7 The annual all-cause mortality rate from LVNC is 2.16%.8 Long-term outcomes of patients with LVNC are influenced by the degree of HF and presence of life-threatening arrhythmias and thromboembolism (TE).7 9 10 Several studies have reported that children with cardiomyopathy have an increased risk of potentially fatal thrombosis.11–13 Extensive trabeculations with multiple recesses are a distinct feature of LVNC and are an ideal environment for thrombi formation. It is believed that the increased risk of TE is attributable to the sluggish blood flow in the deep intertrabecular recesses in patients with LVNC. Nonetheless, no solid evidence supports this hypothesis. Moreover, the risk or occurrence of TE in paediatric patients with LVNC has not been discussed in detail. The treatment strategy for patients with LVNC is similar to those for other cardiomyopathies, but the prevention of TE remains controversial.
In this study, we conducted a systematic review to determine the prevalence and incidence of TE in patients with LVNC, especially in paediatric patients, and searched for risk factors for TE to explore possible management strategies.
Methods
This study was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-analyses guidelines (online supplemental table 1).14
Supplemental material
Patient and public involvement
This study does not involve direct patient participation; thus, this is not applicable to our study.
Eligibility criteria
A systematic search of keywords related to LVNC, anticoagulants/antiplatelets and TE was conducted (online supplemental table 2). TE includes pulmonary embolism, systemic embolism and stroke. Echocardiographic or cardiovascular magnetic resonance criteria were used to diagnosed LVNC according to the Chin, Grothoff, Jacquier, Jenni, Paterick, Petersen and Stöllberger criteria.1 15–20 The exclusion criteria were as follows: studies that did not involve LVNC; articles that did not present original research (conference abstracts, case series, editorials or commentaries); non-human studies (animal studies or in vitro experiments); duplicated studies; and other studies that the investigators considered irrelevant to the objective and studies investigated.
Information sources
We searched the MEDLINE, Embase and Cochrane Central Register of Controlled Trials on the Ovid platform for articles published from January 1946 for MEDLINE and January 1947 for the other databases to December 2020 with no language restrictions. The last search was performed on 3 February 2021. Experienced librarians at the National Center for Child Health and Development, who were also affiliated with Cochrane Japan (Tokyo, Japan), performed searches with the terms detailed in online supplemental table 2).
Study selection
Two investigators independently reviewed the articles. As an initial screening, the titles and abstracts of all articles were screened, and articles that met the exclusion criteria were excluded. As a secondary screening, all articles were reviewed and identified for eligibility. When discrepancies in decisions between the two investigators occurred, a third investigator hosted a face-to-face meeting to determine the eligibility.
Data extraction
The following variables were extracted from each study: number of patients, sex, mean age, follow-up period, diagnostic criteria, imaging modality for diagnosis, LV function, prevalence of TE, atrial fibrillation (AF) and ventricular tachycardia (VT), incidence of TE, anticoagulant and antiplatelet.
Outcomes
The primary outcome was the prevalence and incidence of TE in the patients with LVNC. Overall, 38 studies were reported in the data on the primary endpoint of prevalence of TE and 35 studies were reported in the data on the primary endpoint of incidence of TE. The secondary outcome was the TE and mortality between paediatric and adult patients with LVNC and the risk factors associated with TE. Paediatric patients were defined as those under 19 years old, whereas adult patients were those 19 years old or older.
Assessment of the risk of bias in the included studies
The following key domains were assessed according to the Cochrane Handbook V.5.1.021 : random sequence generation (selection bias), allocation sequence concealment (selection bias), blinding of participants and personnel (performance bias), blinding of outcome assessment (detection bias), incomplete outcome data (attrition bias), selective outcome reporting (reporting bias) and other biases. Two investigators (KH and SO) independently assessed the risk of bias of the included studies (online supplemental table 3). Disagreements were resolved by consensus.21 To reduce exclusion bias and minimise missing data, the authors of the eligible studies were contacted to resolve uncertainties and provide further data.
Data analysis
The interstudy variance was used to adjust for the heterogeneity in prevalence between studies. Heterogeneity was investigated using the I2 statistic (<40%=likely low heterogeneity; 40%–60%=possible moderate heterogeneity; >60%=possible substantial or considerable heterogeneity), which represents the proportion of total variability in the prevalence data attributable to the heterogeneity between the studies. Moreover, the χ2 test (limit=df of freedom) was performed, and p values (10% significance threshold) were assessed. Forest plots were also constructed.
The study was conducted in both children and adults. All results are summarised as mean difference for continuous variables or risk ratio and 95% CI for dichotomous variables. A meta-analysis was performed that assessed the effect on the primary endpoint and were discussed by three or more studies. Before performing meta-analysis, extracted data were transformed from SE of the mean or CI to SD. Random effects models were used to combine the outcomes from multiple studies. The potential for publication bias was assessed by examining the asymmetry of the funnel plots. Meta regression analysis was performed using linear mixed effects model. Meta-regression analysis and subgroup analysis of parameters such as left ventricular ejection fraction (LVEF), duration of follow-up and AF for TE events and mortalities were performed to explore the possible causes of heterogeneity. A prespecified sensitivity meta-analysis was performed for therapies that assessed the effect on the primary endpoint and were discussed by three or more studies. Sensitivity analysis for the primary endpoint excluding studies with antithrombotic treatment in more than 30% of patient’s population was performed to assess the robustness of the synthesised results. A pooled analysis was performed to analyse the factors associated with TE in the paediatric patients.
Continuous variables, ordinal descriptive variables and categorical variables were expressed as means±SD, medians (ranges), and numbers and percentages, respectively. Continuous variables were compared using the unpaired t-test, non-parametric Mann-Whitney U test or one-way analysis of variance, whereas categorical variables were compared using the χ2 statistics or Fisher’s exact test, as appropriate. Univariate regression tests were performed on all variables, and a multivariate logistic regression was performed on statistically significant variables (p<0.05). The variables for inclusion were carefully selected, given the number of events, to ensure parsimony of the final models. Statistical analyses were performed using the software Review Manager V.5.0 (RevMan, Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2008) and the JMP software (V.13; SAS Institute, Cary, North Carolina, USA). P value of <0.05 was considered statistically significant.
Results
Study selection and patient population
A total of 1084 articles were found from the three databases; 949 were excluded because of ineligibility on screening the titles and abstracts (figure 1). Two investigators independently evaluated the entire contents of the remaining 137 articles, and 57 were deemed eligible for our study. The quality of assessment of each study is presented in the risk-of-bias summary (online supplemental table 3).
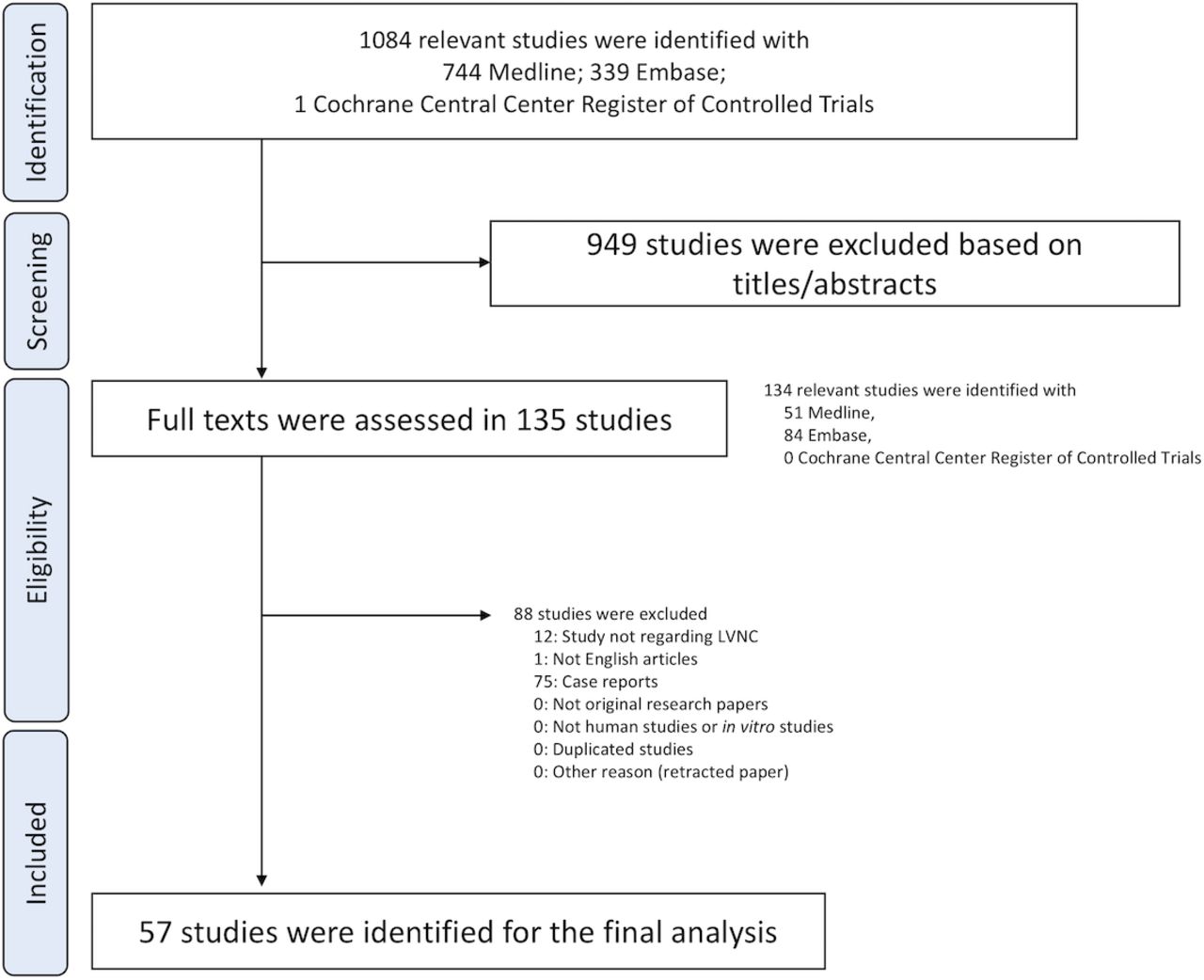
Flow diagram of the study selection. LVNC, left ventricular non-compaction.
Online supplemental table 4 shows the summaries of the studies. A total of 726 paediatric and 3862 adult patients were included. The mean ages of the paediatric and adult patients were 6.1 years (range, 0.5–18.5) and 44.0 years (range, 32.7–57.2), respectively. The mean follow-up durations of the paediatric and adult patients were 4.3 years (range, 2.6–6.1) and 4.0 years (range, 3.4–4.7), respectively. The mean proportions of men in the paediatric and adult patients with LVNC were 55.1% (95% CI, 51.6% to 58.8%) and 40.9% (95% CI, 35.6% to 46.1%), respectively.
The mean prevalence of AF in the paediatric and adult patients with LVNC was 2.6% (95% CI, −0.8% to 5.9%) and 12.9% (95% CI, 10.0% to 15.8%), respectively (online supplemental figure 1). The mean prevalence of VT in the paediatric and adult patients with LVNC were 8.8% (95% CI, 2.3% to %15.3%) and 16.0% (95% CI, 12.4% to 19.6%), respectively (online supplemental figure 1). The mean LVEF in the paediatric and adult patients with LVNC were 52.4% (95% CI, 47.5% to 57.4%) and 40.9% (95% CI, 35.6% to 46.1%), respectively (online supplemental figure 1). There were substantial statistical heterogeneities among the studies in each parameter.
Comparison of TE events between pediatric and adult patients
The mean prevalence of TE in the patients with LVNC was 6.2% (95% CI, 4.7% to 7.6%) (figure 2). There was substantial statistical heterogeneity among studies (I2=73.7%; p<0.0001). The mean prevalence of TE in the paediatric and adult patients with LVNC was 2.6% (95% CI, 1.0% to 4.1%) and 6.2% (95% CI, 4.7% to 7.6%), respectively (figure 2). The proportion of stroke in Hx of TE was 30.0%, 2.2% in children and 31.7% in adults. The proportion of stroke in TE incidents was 35.9%, 4.7% in children and 44.6% in adults. There was a low heterogeneity and substantial statistical heterogeneity among studies (I2=0%; p<0.450 and I2=73.7%; p<0.001), respectively.
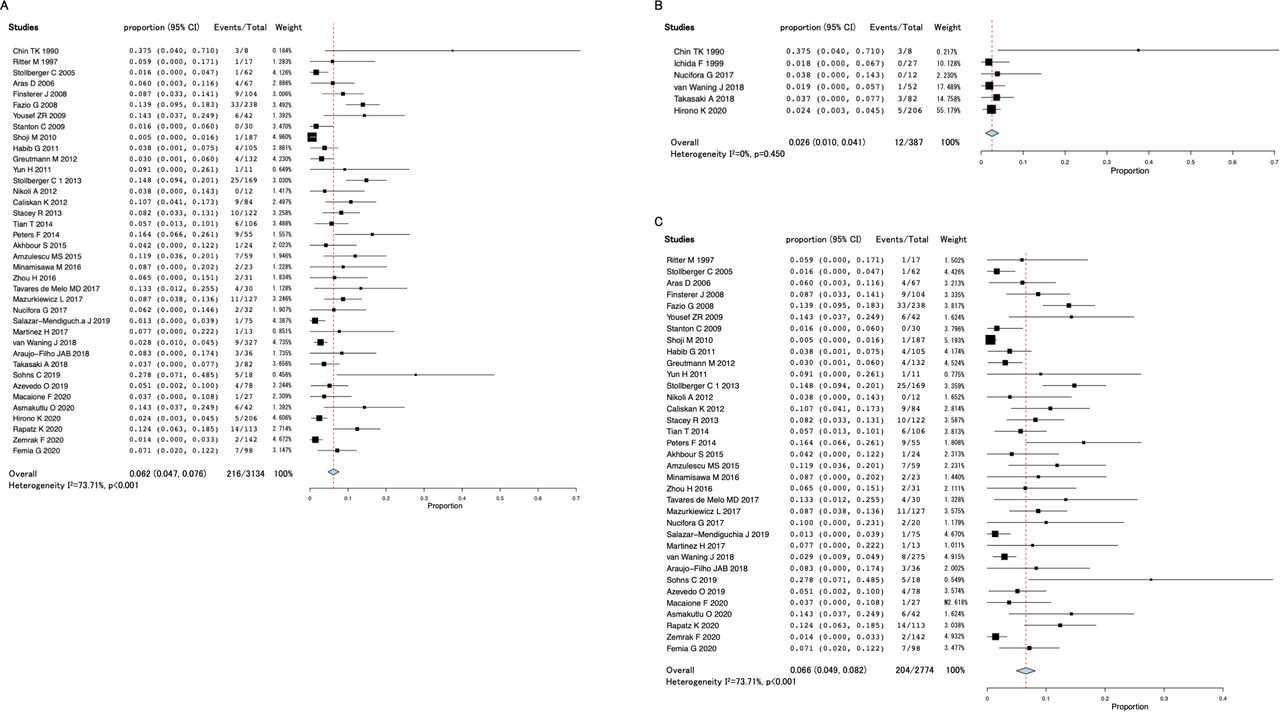
Forest plot of the mean prevalence of thromboembolism in the patients with left ventricular non-compaction (LVNC). Mean prevalence of thromboembolism in all patients (A), paediatric (B) and adult patients (C) with LVNC.
The mean incidence of TE in all patients with LVNC was 2.7% (95% CI, 2.3% to 3.0%) (figure 3), and there was substantial statistical heterogeneity among the studies (I2=99.6%; p<0.0001). The mean incidences of TE in the paediatric and adult patients with LVNC were 1.4% (95% CI, 0.9% to 2.0%) and 2.9% (95% CI, 2.4% to 3.4%), respectively (figure 3), and there was substantial statistical heterogeneity among the studies (I2=99.4%; p<0.001 and I2=99.5%; p<0.001), respectively. The results of the funnel publication bias plot for the prevalence and incidence of TE showed asymmetry that suggested publication bias existed (online supplemental figure 2).

Forest plot of the mean incidence of thromboembolism in the patients with left ventricular non-compaction (LVNC). Mean incidence of thromboembolism in all patients (A), paediatric (B) and adult patients (C) with LVNC.
Meta regression revealed that follow-up period and LVEF were associated with the prevalence of TE, whereas there were no associations between the incidence of TE and any parameters in adult patients (figure 4). Multiple regression analysis also showed that follow-up period, LVEF and the prevalence of AF were associated with the prevalence of TE, whereas there were no associations between the incidence of TE and any parameters (online supplemental table 5). Subgroup analysis showed that reduced LVEF (<40%) and longer follow-up period (>4 years) were the factors associated with high prevalence of TE, and reduced LVEF (<40%) and AF (>10%) were the factors associated with high incidence of TE (online supplemental figures 3 and 4).

Meta regression of follow-up period and left ventricular ejection fraction against prevalence of thromboembolism (TE).
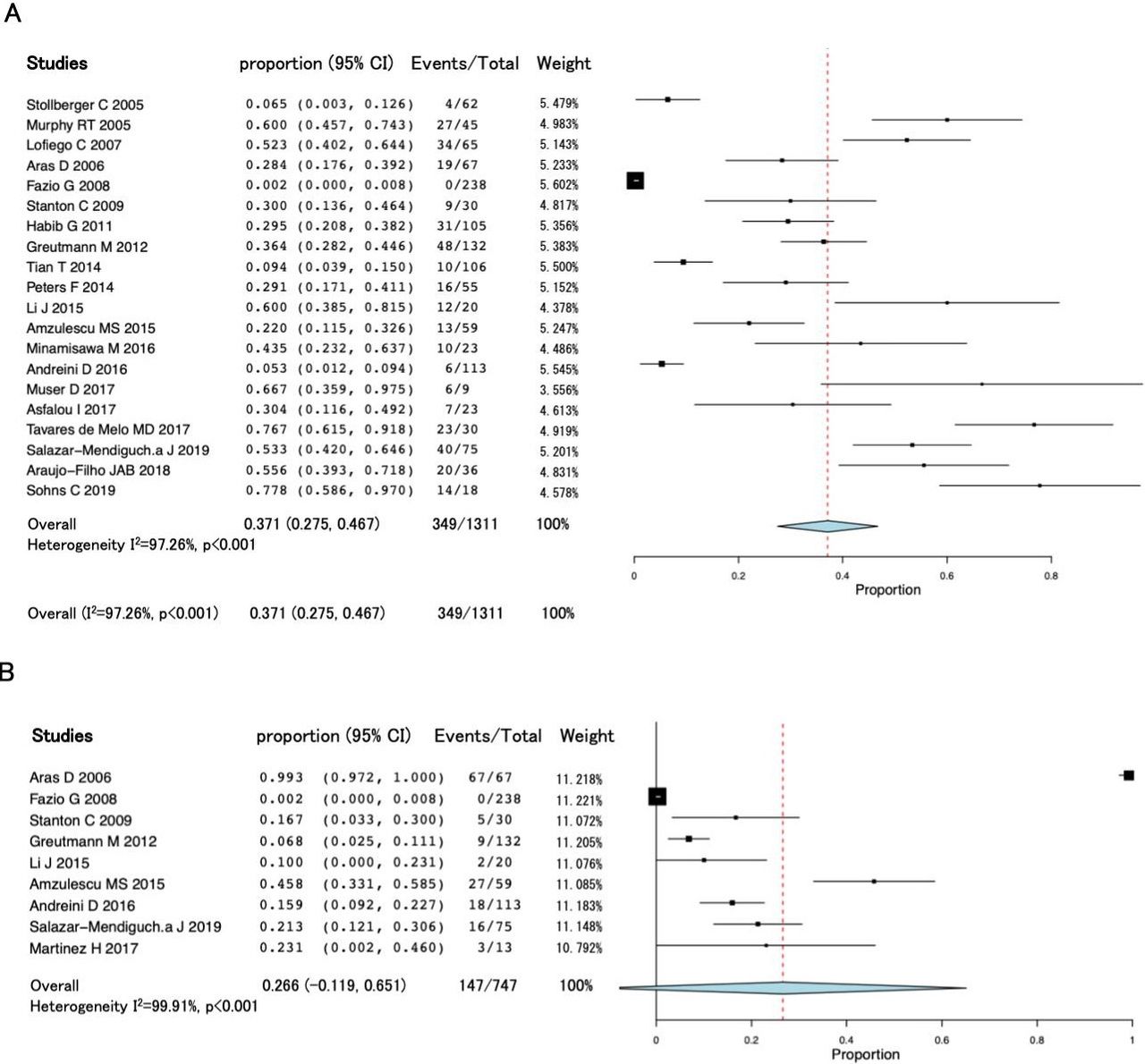
Among the adult patients with LVNC, 37.1% were receiving anticoagulant therapy (95% CI, 27.5% to 46.7%); of these, 80.5% and 19.5% received anticoagulants for primary and secondary prevention, respectively, (figure 5). Regarding anticoagulants, nine studies were used warfarin and one study used rivaroxaban. Among the adult patients with LVNC, 26.6% were receiving antiplatelet therapy (95% CI, −11.9% to 65.1%) (figure 5). Regarding antiplatelets, all studies used aspirin for antiplatelet therapy. In each parameter, there were substantial statistical heterogeneities among the studies. TE was not associated with the use of anticoagulants or antiplatelets (table 1). There were no available data regarding paediatric patients. Prespecified sensitivity meta-analysis for the primary endpoint excluding studies in which antithrombotic treatment in more than 30% of patient’s population showed that the mean prevalence of TE in adult patients with LVNC was 6.5% (95% CI, 4.9% to 8.2%), and the mean incidence of TE in adult patients with LVNC was 6.2% (95% CI, 4.7% to 7.8%) (online supplemental figure 5). These results showed that the prevalence and incidence of TE were increased compared with overall studies, suggesting that antithrombotic treatment may decrease the TE events.

Forest plot of the mean prevalence of anticoagulant and antiplatelet use in adult patients with left ventricular non-compaction (LVNC). Mean prevalence of anticoagulant use in adult patients with LVNC (A). Mean prevalence of antiplatelet use in adult patients with LVNC (B).
Univariate and multivariate logistic regression analyses of independent predictors of thromboembolism in paediatric patients with LVNC
Comparison of mortality and heart transplantation rates between pediatric and adult patients
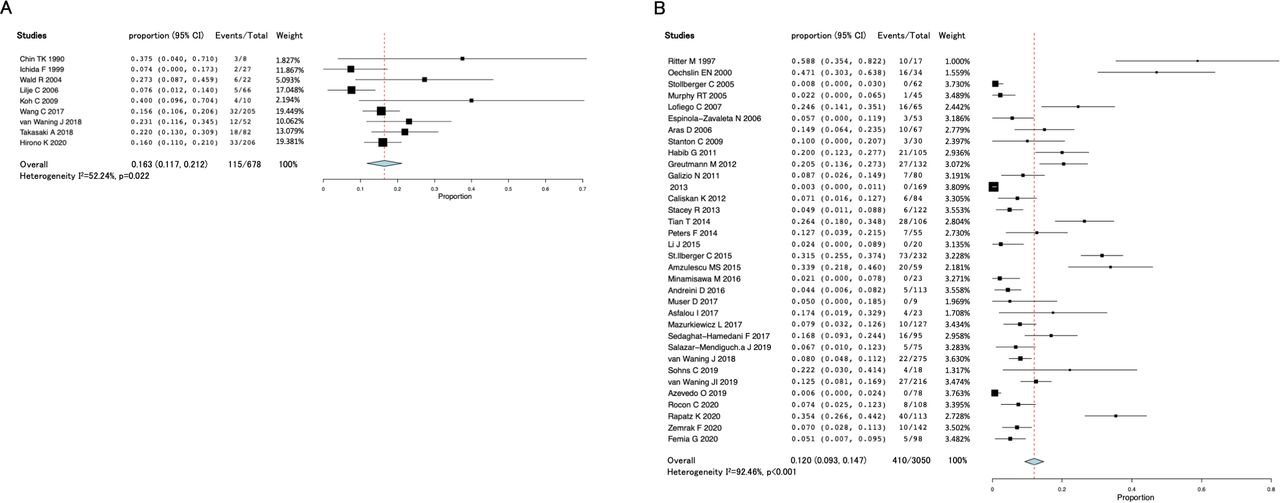
The mean mortality rates in the paediatric and adult patients with LVNC were 11.9% (I2=0%, 95% CI, 9.5% to 14.3%) and 8.9% (I2=89.62%, 95% CI, 6.7% to 11.1%), respectively (figure 6). The mean mortality and heart transplantation rates in the paediatric and adult patients with LVNC were 16.5% (I2=52.24%, 95% CI, 11.7% to 21.2%) and 12.0% (I2=92.46%, 95% CI, 9.3% to 14.7%), respectively (figure 7). Except for the mean survival rate in paediatric patients, there were substantial statistical heterogeneities among the studies in each parameter. Subgroup analysis showed that the studies with reduced LVEF (<40%) was associated with high mortality and death and heart transplantation rate (online supplemental figures 6 and 7).

Forest plot of the mean mortality rates in the paediatric and adult patients with left ventricular non-compaction. Mean mortality rates of paediatric patients (A) and adult patients (B).
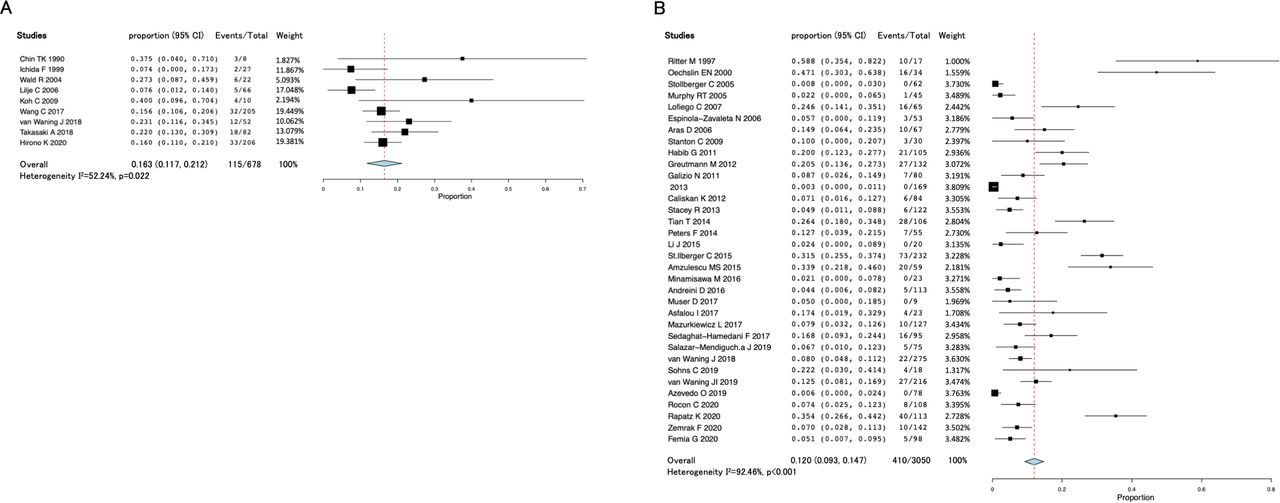
Forest plot of the mean mortality and heart transplantation rates in the paediatric and adult patients with LVNC. Mean mortality and heart transplantation rates in the paediatric patients (A) and adult patients (B).
Factors associated with TE
We analysed the factors associated with TE in the paediatric patients.1 5 7 22 Table 1 shows the univariate and multivariate risk estimates for TE. In the univariate and multivariate analyses, TE was associated with LVEF in <40% of patients (OR, 9.47; 95% CI, 1.35% to 188.2%; p=0.0225). We could not evaluate the association between AF and TE because the prevalence of AF in the paediatric patients with LVNC was relatively low, and patients with AF did not have TE (online supplemental table 6). In adults, there was no relationship between TE and any of the parameters (online supplemental table 7).
Discussion
This is the first systematic review and meta-analysis to elucidate the aetiology of TE in paediatric patients with LVNC. This study revealed that TE occurred in 2.6% of paediatric patients with LVNC, and the incidence rate of TE events was 1.6% per year. The prevalence and incidence rates in paediatric patients were lower than those in adult patients. Moreover, multivariate logistic regression analysis showed that TE was associated with LVEF in <40% of paediatric patients with LVNC (figure 8).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Schematic figure of this study. AF, atrial fibrillation; LVEF, left ventricular ejection fraction; VT, ventricular tachycardia.
The overall annual incidence rate of TE in all patients with LVNC in this study ranged from 0.08% to 0.27%; in the general adult population, it ranged from 0.11% to 0.18%, while it was 0.003% in the general paediatric population.23 The annual incidence rate of TE was 0.003% in general paediatric cohort.24 TE occasionally develops in patients with cardiomyopathies; its prevalence in patients with hypertrophic cardiomyopathy (HCM) is approximately 10%.25 In another cohort, the 5-year rate of TE events was 5.5%.26 Similarly, in another study, TE events occurred in 15% of patients with dilated cardiomyopathy (DCM),27 and intracardiac thrombi were detected in 6% of paediatric patients with DCM.28 In patients with DCM, the risk of developing TE increases when the LVEF is <20%.13 Our results showed that the mean prevalence of TE in patients with LVNC among all ages was 6.2%, which is similar to or even lower than the prevalence of other cardiomyopathies. Furthermore, the prevalence and incidence of TE events in paediatric patients were relatively lower than those in adult patients. Advanced age is also a significant risk factor for TE and acknowledged by several trials.29 30 Because AF and HF were frequently observed in our results, the incidence of TE events may be increased in adult patients.
The risk of TE due to unfavourable cardiovascular conditions, such as LV systolic dysfunction or AF, may be increased in patients with LVNC.3 The pathogenesis of TE in HF is multifactorial, with changes occurring at the molecular level in addition to abnormalities in blood flow dynamics.31 HF resulting in poor contractility and low cardiac output leads to static blood flow, which results in an inherent hypercoagulable state. Consequently, HF increases the risk of thrombus development.32 Several studies have demonstrated that the risk of TE increases as LVEF decreases.33 The annual incidence of TE in patients with HF is reported to be 1.2%–1.8%.34 Our pooled analysis showed that the prevalence of TE was 3.9% in patients with LVNC with concomitant HF. Thus, dilated and poorly contracting ventricles may promote thrombus formation within the intertrabecular recesses in the paediatric patients with LVNC.
Compared with the general population, patients with AF have a threefold to fivefold increased risk of TE.35 In the patients with HCM, AF is also the most common arrhythmia, and the prevalence of TE in patients with HCM is 20%–25%, which is fourfold to sixfold higher than that in the general population.36 However, this study could not evaluate the association between AF and TE because the prevalence of AF in paediatric patients with LVNC was relatively low, and patients with AF did not have TE.
Several studies have reported that antiplatelet therapy or systemic anticoagulation was used for patients with LVNC, as shown in our results. Stollberger et al investigated TE event rates in 62 patients with LVNC, of whom 6 had TE; of these, 5 (9.7%) had systolic dysfunction.37 They concluded that prophylaxis might be needed for patients with LVNC and systolic dysfunction. Pitta et al suggested that anticoagulants or antiplatelets should be considered in adults, especially when HF or AF was present.38 Many healthcare institutions treat adults with anticoagulant or antiplatelet therapy, especially those with a history of systolic dysfunction. Moreover, the incidence of TE decreased in patients with HF who received thromboprophylaxis when compared with those who did not.39 The incidence of TE events in children remains unclear, and anticoagulant and/or antiplatelet drugs might be an option in those with depressed LV systolic dysfunction.
Direct oral anticoagulants (DOACs) are direct thrombin and factor Xa inhibitors that allow for effective anticoagulation without the routine monitoring required with warfarin administration. Compelling data are demonstrating the efficacy and safety of DOACs when compared with warfarin for the prevention of stroke in patients with AF.40 Similarly, the treatment of venothromboembolic disease with DOACs compared with warfarin has been shown to be efficacious and safe.41 42 However, no studies are available on the preference for warfarin or DOACs in patients with LVNC. Additionally, the risk of bleeding, hospitalisation and other adverse cardiac events often negates any incremental benefit derived from DOACs. Further studies are warranted to evaluate whether DOACs are necessary and justified for the management of TE.
The multiple diagnostic criteria for LVNC were included in this study. Presently, there is no gold standard of treatment and diagnostic criteria for LVNC. The definition of LVNC was based on echocardiography and MRI results in previous studies. LVNC is usually diagnosed using a two-dimensional transthoracic echocardiogram. However, the use of advanced imaging technologies, such as MRI, is increasing. The emergence of cardiac MRI has enabled high-resolution imaging of cardiac structures. Generally, echocardiography and MRI have different false positive rates, with MRI having a higher false positive rate than echocardiography. Thus, MRI is more likely to diagnose patients with normal cardiac function and asymptomatic patients, which may affect the present results. Conversely, the current criteria for the diagnosis of LVNC on echocardiograms are unclear. Kohli et al demonstrated that there was a poor correlation among the different criteria when diagnosing LVNC by echocardiogram; however, their study only included adult patients.43 Thus, the concept of the presence of non-compaction cannot be translated to infants and children with extensive area of non-compaction. It is unknown whether these differences in the diagnostic criteria and modalities used influenced the results, which warrants further studies.
Study limitations
Our study has several limitations. First, different studies were adjusted for different confounding factors, making it challenging to compare the results across studies. Second, pooled results showed a high level of heterogeneity among observational studies. Substantial heterogeneity existed among observational TE studies in patients with LVNC. Possible explanations for the inconsistencies and high level of heterogeneity include patient samples from diverse countries and data sources, different follow-up durations, mixed study cohorts of LVNC and other patients, different risk assessment tools used, adjustment for different covariates and unmeasured confounders. Third, we did not have complete resources to review non-English publications. However, we included articles from an extensive search of broad databases and are confident that this study covered most of the high-quality and well-designed studies. Although several studies included both paediatric and adult populations, even though one of them was dominant, they could not be completely separated into each population group.
Conclusions
Compared with healthy controls, patients with LVNC have an increased risk of TE. The prevalence and incidence rates in paediatric patients were lower than those in adult patients. TE is associated with a reduced systolic function in paediatric patients with LVNC. Furthermore, advanced age appears to be a risk factor for TE. Further randomised control trials or case–control studies to establish treatment guidelines for TE in patients with LVNC are warranted.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
Ethics approval
The Research Ethics Committee of the University of Toyama approved the study protocol (I2017003), which conformed to the ethical guidelines of the 1975 Declaration of Helsinki.
Acknowledgments
The authors wish to acknowledge Hitoshi Moriuchi, Haruna Hirai and Eriko Masuda for their expert technical assistance.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors KH contributed to the conception and design of the study. FI organised the database. HO performed the statistical analysis. KH wrote the first draft of the manuscript. ST, NM, HN, KI and SO wrote sections of the manuscript. All authors contributed to manuscript revision, read and approved the submitted version. KH is the author acting as guarantor.
Funding KH and FI are supported by grants from The Ministry of Education, Culture, Sports, Science and Technology in Japan (Grant-in-Aid for Scientific Research Nos. 18K07785).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.