Article Text

Abstract
Objectives Uncertainty about the benefit of (high-intensity) statins for women remains due to under-representation of women in primary prevention trials and scarcity of sex-stratified data. This study evaluates the sex-specific relation between statin treatment and survival and the additional benefit of high-intensity statins.
Methods Electronic health record data from 47 801 patients (17 008 statin users and 30 793 non-users) without prior cardiovascular disease were extracted from thirteen Dutch outpatient cardiology clinics. Patients prescribed statins at baseline were propensity-score matched to those eligible for statin therapy (low-density lipoprotein >2.5 mmol/L) without a statin prescription. Statins were divided into low-intensity and high-intensity according to Dutch guidelines. Mortality data were obtained via linkage to the national mortality registry. Cox regression was used to evaluate the relationship between statin prescription and intensity and all-cause and cardiovascular mortality.
Results Propensity score matching created a cohort of 8631 statin users and 8631 non-users. 35% of women and 28% of men received a low-intensity statin. The beneficial effect of statins on both all-cause and cardiovascular mortality was stronger in women (HR 0.66, 95% CI 0.58 to 0.74 and HR 0.55, 95% CI 0.39 to 0.71, respectively) than in men (HR 0.89, 95% CI 0.81 to 0.95 and HR 0.93, 95% CI 0.77 to 1.08, respectively). High-intensity statins conferred modest protection against all-cause mortality (HR 0.94, 95% CI 0.88 to 1.00) and cardiovascular mortality (HR 0.86, 95% CI 0.74 to 0.98) in both sexes.
Conclusions The protective effect of primary prevention statins was stronger in women than men for both all-cause and cardiovascular mortality. High-intensity statins conferred a modest additional benefit in both sexes. Statins seem to be effective regardless of treatment intensity, especially in women.
- STATINS
- EPIDEMIOLOGY
- Electronic Health Records
Data availability statement
No data are available. All data are stored within the UMC infrastructure and cannot be made publicly available due to privacy constraints. The survival follow-up data obtained via record linkage with Statistics Netherlands are not publicly available and cannot be accessed by researchers not registered on the project.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known about this subject?
Women more often receive low-intensity statin therapy than men despite evidence that statin therapy lowers cardiovascular disease risk in a dose-dependent manner.
It remains unclear whether statin treatment is equally effective in women and men due to under-representation of women in primary prevention trials and scarcity of sex-stratified data.
This study evaluates the sex-specific relation between statin treatment and survival, and explores whether high-intensity statins confer additional benefit.
What does this study add?
Statins were effective in lowering cardiovascular disease risk, especially in women, and high-intensity regimens conferred only marginal additional benefit in both sexes.
How might this impact on clinical practice?
The current trend of preferentially prescribing women low-intensity statins does not seem to reduce the potential benefit of treatment. Future studies are needed to evaluate whether lower dosages are appropriate if higher dosages lead to side effects or otherwise negatively influence quality of life.
Introduction
Statins have been shown to effectively lower the risk of cardiovascular events by reducing low-density lipoprotein (LDL) levels, with high-intensity regiments being more effective than low-intensity variants.1 This effect is seen independently of baseline mortality risk,2 suggesting that all people at risk of cardiovascular events benefit from treatment. However, women are less likely to receive guideline-recommended statin therapy than men in both primary and secondary prevention.3–5 It has been shown that women are more likely to refuse or stop statin therapy3 6 and that healthcare professionals are also less likely to prescribe (high-intensity) statins for women.3 5 This careful approach may stem from remaining uncertainty about the benefit of statin therapy as primary prevention strategy for women due to the low number of women in primary prevention trials.7
There is some evidence to suggest that women and men may benefit equally from statin treatment.8 9 The Justification for the Use of Statins in Prevention: An Intervention Trial Evaluating Rosuvastatin trial showed that rosuvastatin reduced the risk of cardiovascular events and cardiovascular mortality in both women and men.10 In addition, data from a primary care cohort of new statin users showed that improved adherence to statins reduced the risk of hospitalisation for cardiovascular events in both men and women to a similar extent.6 While some meta-analyses of primary prevention trials confirmed that statin treatment benefits both sexes,2 10 others failed to find such positive effects.11 12 Moreover, it remains unclear whether the intensity of therapy influences outcomes. Therefore, we used regular care data from cardiac outpatient clinics to study whether receiving a statin prescription for primary prevention affects long-term prognosis in women and men without a history of cardiovascular disease. We also explored whether high-intensity statins confer additional protection over low-intensity regimens.
Methods
Study population
The Cardiology Centers of the Netherlands regular care database contains data from 109 151 unique patients that were referred for a full cardiac workup by their general practitioner on suspicion of cardiac disease between 2007 and 2018. During the first visit, information was collected on anthropometric measurements, cardiovascular risk factors, medical history, comorbidities and medication use. All patients underwent transthoracic echography and electrocardiography at rest. Stress electrocardiography and laboratory measurements were performed in approximately 75% of patients. Passive follow-up was obtained for 95.9% of the study population via linkage to the national mortality registry.
For the current study, all patients with a history of coronary heart disease, heart failure, cerebrovascular disease or congenital heart disease, or a prior or ongoing statin prescription were excluded.
Selection of statin users and non-users
Medication prescriptions were identified using pattern matching based on a combination of generic compound names and brand names. The search term was based on brand names of statins available in the Netherlands tailored to those that were prescribed within the study population. It contained the words statin, crestor, lipitor, selektine, zocor and tahor. Medication dose was extracted from the text fields and multiplied by daily frequency and dosage to obtain the daily dose per prescription. The grepl and gsub functions from the R grep package were used for the name and dose pattern matching, respectively. Statin prescription entries missing information on dose or daily frequency, prescriptions with a negative duration and one-off prescriptions were excluded. Combination preparations with ezetimibe or fenofibrate were also excluded because Dutch guidelines recommend these when prior statin-only therapy was not effective enough, so these prescriptions are unlikely to be a patient’s first statin prescription.
Statin users were defined as patients who received their first statin prescription within 31 days prior to or after their baseline visit. The 31-day window was chosen to both allow for small delays in data entry and include people prescribed statins shortly before or after their visit at the cardiac outpatient clinic, because labelling these people as non-users would introduce misclassification. Non-users were defined as patients eligible for statin therapy according to the Dutch primary prevention guidelines (LDL>2.5 mmol/L) who did not receive a statin prescription within the 31-day period.
Definition of statin intensity
The intensity of statin treatment was categorised as lower, equal or higher based on how much it lowered LDL cholesterol levels compared with the Dutch primary prevention guideline-recommended dose of 40 mg simvastatin (online supplemental table 1).13–15 We compared patients on lower intensity statin regimens (low intensity) with patients on equal and higher intensity regimens (high intensity).
Supplemental material
Outcome
Passive follow-up for all-cause mortality was available for 95.9% of the study population via linkage to the national mortality registry from Statistics Netherlands. This registry continuously collects all official cause of death reports submitted by medical doctors and coroners in the Netherlands and is updated quarterly throughout the year and at the end of each year. The cause of death is coded according to the guidelines of the WHO using the International Classification of Diseases and related Health Problems edition 10 (ICD-10). For the current analyses, all-cause mortality was available until 12 February 2020 and cause-specific mortality was available until 1 January 2020. Follow-up time for patients who were still alive was censored on 12 February 2020. All-cause mortality was defined as having a date of death recorded in the mortality registry. Cardiovascular mortality was defined as any mortality entry that was labelled with an ICD-10 code from the diseases of the circulatory system chapter (I00–I99).
Propensity score matching
We created propensity-score matched cohorts for our analyses to account for confounding by indication. We first imputed missing data on components of the propensity score using the mice16 package, resulting in five imputed datasets. We subsequently calculated the propensity score in each imputed dataset based on a set of confounding variables (online supplemental table 2) and matched one-on-one to create five new cohorts where all confounders were balanced between the two groups. We used the MatchIt17 package to calculate the propensity score and perform the matching, applying the nearest neighbours approach with a calliper width of 0.1. We assessed whether covariates were properly balanced based on the mean difference using the cobalt package. We then ran our survival analyses in each imputed matched dataset and pooled the results using the meta package.
For the analyses exploring the relationship between statin use and long-term prognosis, we propensity-score matched statin users with statin non-users. For the analyses exploring the relationship between statin intensity and long-term prognosis, we propensity-score matched low-intensity statin users with high-intensity statin users.
Statistical analyses
Continuous variables were reported as mean (SD) or median (IQR), depending on their distribution. Categorical variables were reported as number and percentage. The effect of statin prescription on long-term prognosis and the effect of statin intensity on long-term prognosis were evaluated using Cox regression in the whole propensity-matched cohort and stratified by sex. We calculated robust confidence intervals to account for the matched nature of the dataset. The presence of sex differences in treatment effect was tested using an interaction term.
Sensitivity analysis
We excluded participants with a history of cardiovascular disease, which was defined as having a cardiovascular diagnosis before baseline. However, 2000 patients (12%) were diagnosed with cardiovascular disease at baseline. To test the robustness of our findings, we repeated the main analysis excluding these 2000 patients. A new propensity score matched cohort was created with the same set of variables used in the main analysis except those related to cardiovascular disease diagnosis. We based our definition of high-intensity statin on Dutch guidelines, which resulted in a different classification than what is internationally used. To check generalisability of our results, we repeated the main analysis defining high-intensity statins as those that reduce LDL cholesterol by 50% or more (atorvastatin 40 mg or higher, rosuvastatin 20 mg or higher and simvastatin 80 mg or higher).
All analyses were performed in R (R Core Team, Vienna, Austria). A p <0.05 was considered statistically significant.
Patient and public involvement
Patients or public were not involved in any stage of the research process.
Results
Propensity score matching
We extracted data from 17 008 statin users (48% women) and 30 793 patients (57% women) eligible for statin therapy who did not receive any statins (non-users) (figure 1; online supplemental table 3). Statin users were on average older (62±11 vs 55±13 years), more often men (52% vs 43%) and had a higher median 10-year cardiovascular mortality risk (3.94 (1.68–8.36) vs 1.66 (0.45–4.77)) compared with non-users. They also more often presented with comorbidities such as hypertension (46% vs 23%) and dyslipidaemia (39% vs 7%), and were more often prescribed cardiovascular medication other than statins at baseline (80% vs 34%) compared with non-users (online supplemental table 3). Due to these pronounced differences between statin users and non-users, it was not possible to match each statin user to a non-user with a similar propensity score and individuals that could not be matched were excluded from analyses. Propensity-score matching resulted in a cohort consisting of 8631 statin users and 8631 non-users who were highly similar on all baseline characteristics (table 1).
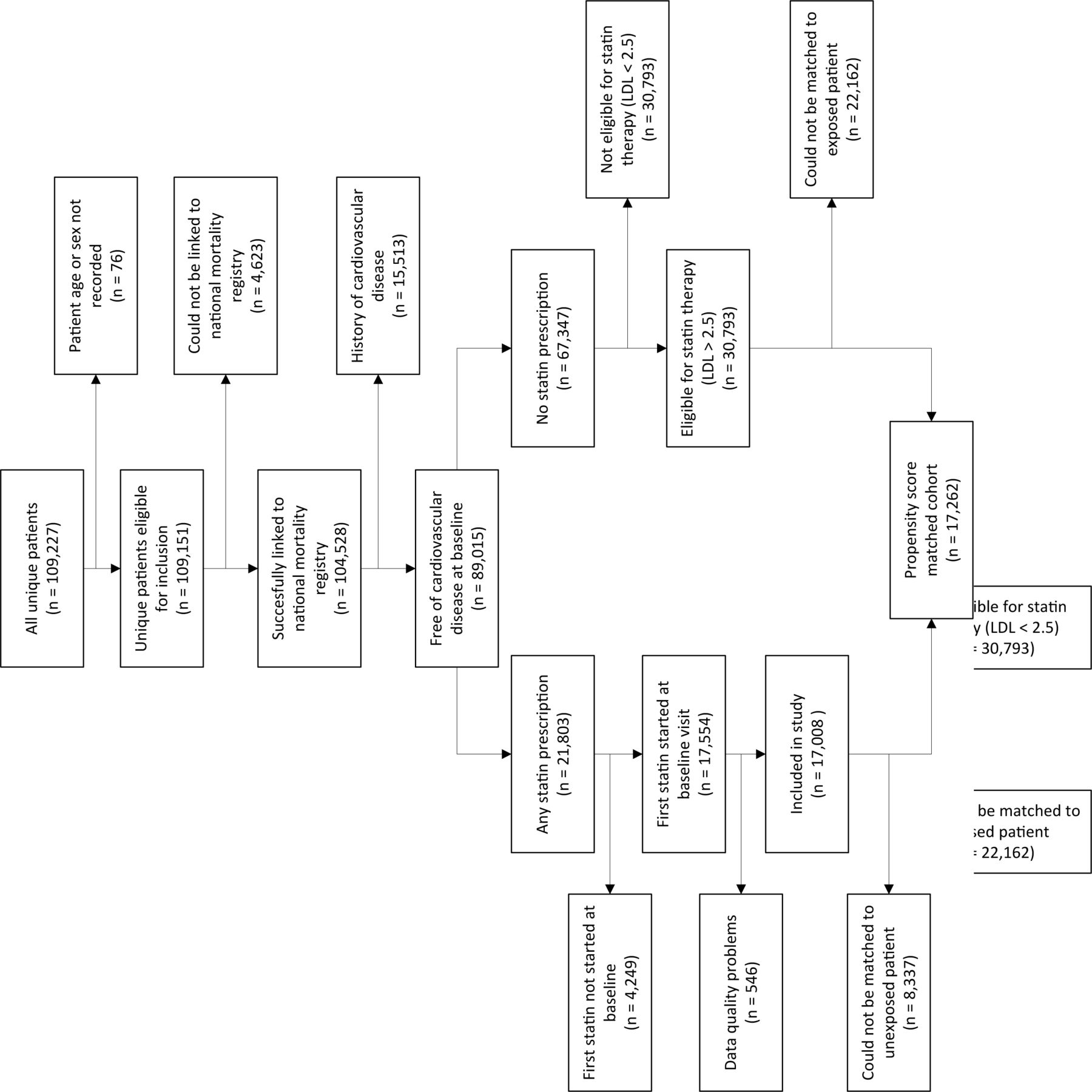
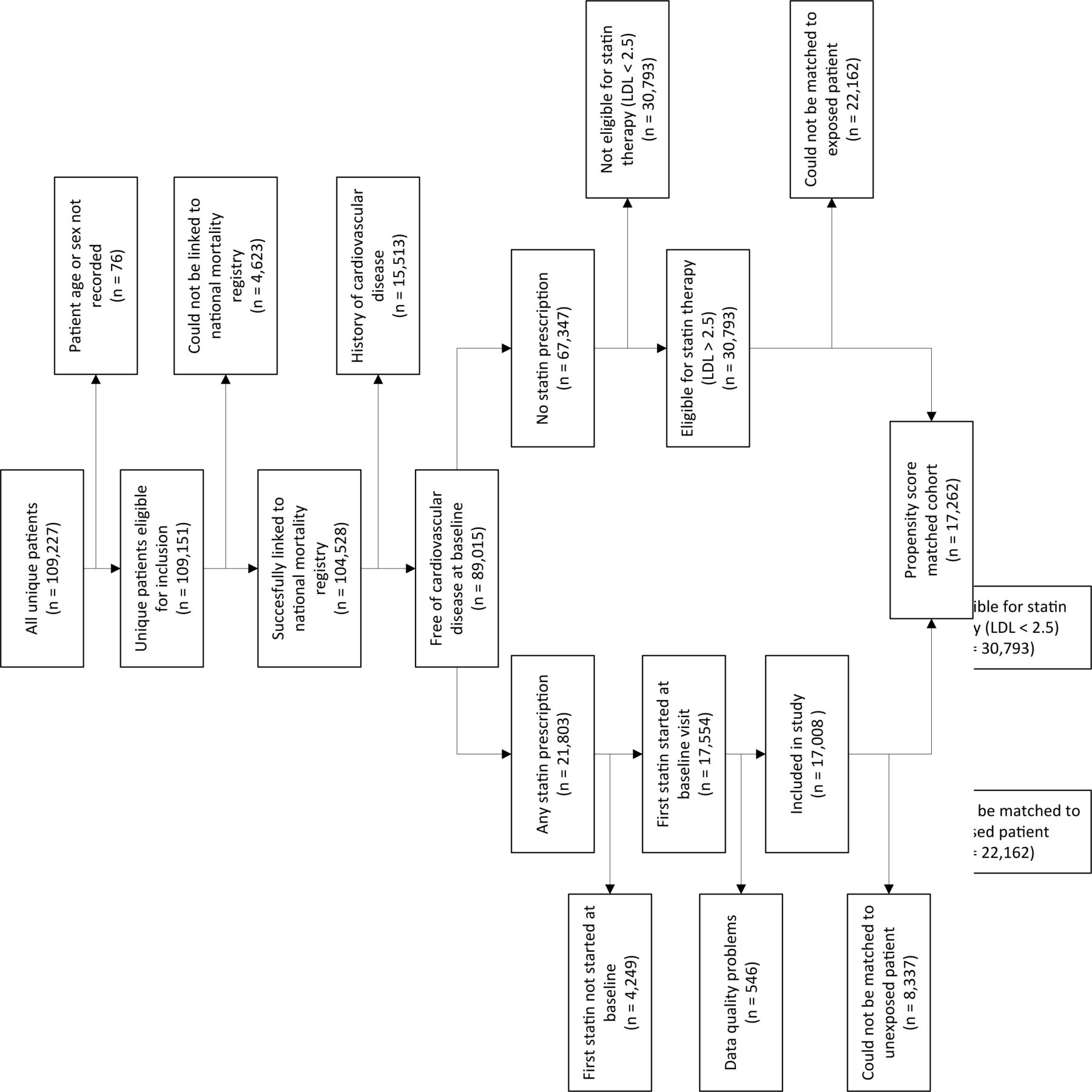{kind=link}
Flow chart describing the study population selection process. LDL, low-density lipoprotein.
Baseline characteristics of statin users and non-users after propensity score matching
Propensity-score matched study population
Female statin users were on average older than male statin users (62±10 vs 59±11 years) and more often had a low (0%–4%) cardiovascular mortality risk (61% vs 49%). They less often presented without cardiovascular complaints (36% vs 45%) and had a lower estimated glomerular filtration rate (76±24 vs 89±28 mL/min/m3). Similar differences between the sexes were seen for the statin non-users. The prevalence of comorbidities and medication use was similar between the sexes for both statin users and non-users (table 2).
Baseline characteristics of statin users and non-users after propensity-score matching stratified by sex
Statin use and mortality risk
Median follow-up in the matched cohort was 5.8 (3.5–7.9) years, during which 1035 patients (50% women) died. Cardiovascular deaths accounted for a total of 270 events (26% of total). In the whole cohort, statin use reduced the risk of all-cause mortality by 24% (HR 0.76, 95% CI 0.71 to 0.82) and the risk of cardiovascular mortality by 28% (HR 0.72, 95% CI 0.61 to 0.83). This protective effect was stronger in women, with a 34% lower all-cause mortality risk (HR 0.66, 95% CI 0.58 to 0.74) and a 45% lower cardiovascular mortality risk (HR 0.55, 95% CI 0.39 to 0.71) in statin users compared with non-users. A similar but weaker trend was seen for men, with an 11% reduction in all-cause mortality (HR 0.89, 95% CI 0.81 to 0.96) and a non-significant 7% reduction in cardiovascular mortality (HR 0.93, 95% CI 0.77 to 1.08) in statin users compared with non-users (table 3). The interaction term for sex was statistically significant for both all-cause mortality (p value for interaction=0.040) and cardiovascular mortality (p value for interaction=0.035).
Adjusted HRs with 95% CIs for the risk of all-cause and cardiovascular mortality associated with statin use stratified by sex
Statin intensity and mortality risk
Thirty-six per cent of women who were prescribed statins (n=8171) received a low-intensity statin and 26% received a high-intensity statin, compared with 29% and 28% of men who were prescribed statins (n=8837), respectively. The remainder received a statin prescription at guideline-recommended dose (38% of women vs 42% of men).
Propensity score matching resulted in a cohort of 10 688 patients (52% women) with a balanced confounder distribution (online supplemental table 4). The total number of deaths was 820 in this cohort, of which 224 were cardiovascular. Higher intensity statins conferred a small protective effect against all-cause mortality (HR 0.94, 95% CI 0.88 to 1.00) and cardiovascular mortality (HR 0.86, 95% CI 0.74 to 0.98) compared with lower intensity statins. The results were similar for women (HR 0.91, 95% CI 0.82 to 1.00 and HR 0.88, 95% CI 0.70 to 1.05, respectively) and men (HR 0.96, 95% CI 0.88 to 1.05 and HR 0.85, 95% CI 0.69 to 1.01, respectively) although not statistically significant (table 4). There was no significant interaction between sex and statin intensity for neither all-cause mortality (p value for interaction=0.73) nor cardiovascular mortality (p value for interaction=0.76).
Adjusted HRs with 95% CIs for the risk of all-cause and cardiovascular mortality associated with having a statin prescription equal to or higher than guideline-recommended intensity stratified by sex
Sensitivity analysis
Repeating our analyses in those without a cardiovascular diagnosis at baseline resulted in a matched cohort of 15 180 people (52% women). Results for all-cause mortality were similar to the main analysis in both sexes, but the protective effect of statins for cardiovascular mortality was no longer present in men (HR 1.02, 95% CI 0.86 to 1.18) when restricted to this subgroup (online supplemental table 5). Repeating our analyses with the adapted definition of high-intensity statin did not change our results (data not shown).
Discussion
This study shows that fewer women eligible for statin therapy received statins compared with men, and when they did, they more often received a low-intensity statin. Statin prescription for primary prevention reduced the risk of all-cause and cardiovascular mortality to a greater extent in women compared with men. High-intensity statins conferred modest additional protection against both mortality outcomes and this effect was similar for women and men.
The main strength of our study was the use of a clinical care database that closely reflects the current situation in clinical care, both regarding statin prescription practices and patients that are seen at such outpatient clinics. Women were well represented (52%) and the majority of patients (55%) had a low (<5%) 10-year risk of cardiovascular mortality, which is exactly the patient population for whom more evidence regarding statin efficacy is warranted. The main limitation of our study is that data collection was driven by medical need and thus not performed systematically. Residual confounding may remain despite our efforts to control for confounding by indication. This may have biased our findings towards the null because patients with a higher mortality risk have a higher chance of being prescribed (high-intensity) statins, which would reduce the difference in survival between statin users and non-users and low-intensity and high-intensity statin users. We were also unable to evaluate more short-term outcomes that may be relevant in this low-risk population such as cardiovascular events and hospitalisations, and lacked good-quality data on adverse drug reactions. We were unable to correct for potential sex differences in adherence, but this is unlikely to change the interpretation of our findings because literature suggests women have poorer adherence than men, which would lead us to underestimate the observed benefit in women.3 18
Our finding that the protective effect of statins was stronger in women compared with men corresponds to findings from previous studies looking at sex differences in statin effectiveness.2 10–12 The protective effect of statin was not seen in men after the exclusion of those diagnosed with cardiovascular disease at baseline. This is in line with findings from a meta-analysis that showed statin use for primary prevention reduced mortality in women but not men, while statin use for secondary prevention did reduce mortality in men.2 Literature also suggests low-risk patients could gain most benefit from statin treatment.2 19 This may explain both why we found such a strong effect of statin treatment in our whole cohort compared with previous trials, and why we found a stronger effect in women compared with men. Our study population had a low median 10-year cardiovascular mortality risk of approximately 3.5%. Women had a lower average mortality risk than men (2.9% vs 4.1%, respectively), and fewer women in both the statin-treated and statin-untreated group had a high mortality risk (≥10%) compared with men. Another potential explanation might be that women adhered better to lifestyle recommendations such as dietary advice provided complementary to statin treatment than men, but literature on this topic is scarce.20 In addition, our findings need to be validated. This may be difficult within a trial setting due to the long follow-up time required to accrue sufficient mortality endpoints in these relatively healthy populations. Other observational studies using real-world data may offer valuable insights, provided they are able to properly correct for indication bias. Such studies can also evaluate the generalisability of our findings. Our database only includes Dutch patients located at the unique intersection between primary and secondary care, and we had to exclude the healthiest and least healthy patients because these could not be matched to a counterpart with a sufficiently similar propensity score. It remains unclear how our findings translate to these patient groups.
Women in our dataset more often received low-intensity statins compared with men, confirming previous work.3–5 The evidence supporting equal statin prescription strategies for both sexes is growing, but higher rates of side effects in women may be the underlying reason for maintaining this careful approach to statin prescription in women. The topic of statin-related side effects is still debated. Meta-analyses suggesting no differences in adverse events between treatment and placebo arms,2 10 21 22 but others argue that statin-related side effects, especially milder ones, are very common and an important challenge in statin treatment.23 There is also some evidence for sex differences in adverse events,2 3 21 but this is not yet conclusive. Our analyses exploring the relationship between statin intensity and long-term prognosis suggested high-intensity regimens only conferred marginal additional benefit. This raises the question whether low-intensity statins could already be sufficiently effective in women, and whether the small additional benefit of high-intensity statins is proportional to the increased risk of potential side effects. These yet unanswered questions underscore the importance of clinical trials providing sex-specific data for both the efficacy of low-intensity versus high-intensity statins and adverse events rates associated with different statin intensities. Dose-finding trials could answer the question which statin dosage best balances prognosis benefits against possible harms such as side effects.
Conclusion
Fewer women received statins than men, and when they did, they were more likely to receive low-intensity regimens. The protective effect of primary prevention statins was stronger in women than men for both all-cause and cardiovascular mortality, but the additional benefit of high-intensity statins was modest and similar for both sexes. Statins seem to be effective regardless of treatment intensity, especially in women.
Data availability statement
No data are available. All data are stored within the UMC infrastructure and cannot be made publicly available due to privacy constraints. The survival follow-up data obtained via record linkage with Statistics Netherlands are not publicly available and cannot be accessed by researchers not registered on the project.
Ethics statements
Patient consent for publication
Acknowledgments
Results are based on calculations by the authors using non-public microdata from Statistics Netherlands.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors SB conceived the research question, cleaned the raw data, performed data analyses and wrote the manuscript. NCO-M conceived the research question, supported data analysis and critically reviewed the manuscript. MJ performed part of the data analyses. IIT, LH and GAS collected the raw data and reviewed the manuscript. MH critically reviewed the manuscript. HMdR conceived the research question, obtained funding, supported data analyses and critically reviewed the manuscript. HMdR acts as the guarantor for this study.
Funding This work was supported by the Dutch Cardiovascular Alliance consortium DCVA IMPRESS (2020B004) and ERC Consolidator grant UCARE (866478).
Competing interests LH, IIT and GAS are employed by Cardiology Centers of the Netherlands. All other authors declare no competing interests.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.