Article Text

Abstract
Objective To assess the feasibility, efficacy and safety of performing exercise stress echocardiography (ESE) for the assessment of myocardial ischaemia during the COVID-19 pandemic.
Methods and results Baseline data were collected prospectively on 740 consecutive patients (mean age 61.4 years, 56.8% males), referred for a stress echocardiogram (SE), who underwent ESE between July 2020 (immediate post lockdown) and January 2021 according to national safety guidelines, in addition to patients wearing masks during ESE. Retrospective analysis was performed on follow-up data for outcomes. Propensity score matching was used to compare workload achieved during ESE pre-COVID-19, in 768 consecutive patients who underwent ESE between May 2014 and May 2015. Of the 725 (97.9%) diagnostic tests obtained, 69 (9.3%) demonstrated significant inducible ischaemia (≥3 segments) with no serious adverse events. Of the 61 patients who underwent coronary angiography, 51 (83%) demonstrated flow-limiting coronary artery disease. During a mean follow-up period of 4.6 months, one first-cardiac event was recorded.
Compliance with mask-wearing throughout ESE was seen in 98.7% of patients. Of the 17 healthcare professionals performing ESE, none contracted COVID-19 during this period. SE service performance increased to 96.8% of prepandemic levels (100%) from 26.6% at the start of July 2020 to the end of December 2020.
Propensity-matched data showed no significant difference in exercise workload between patients undergoing ESE during and prepandemic.
Conclusion Performing ESE during the COVID-19 pandemic, with safety measures in place, is feasible, efficacious and safe. It impacted on the time patients were waiting to undergo a diagnostic test and yielded appropriate outcomes.
Service evaluation authorisation of research capability number
SE20/059.
- coronary artery disease
- diagnostic imaging
- echocardiography
Data availability statement
Data are available on reasonable request. The final anonymous dataset that supports the findings of this study are available from the corresponding author, RS, on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known about this subject?
At the start of the pandemic, there was an abrupt termination of many cardiovascular diagnostic services, with very limited services resuming after the first lockdown.
The greatest disruption was seen in those procedures considered aerosolising such as exercise stress echocardiography (ESE), resulting in increasing waiting times for patients and potentially affecting outcomes adversely.
What does this study add?
This study adds data on how ESE can be performed safely and effectively while adopting safety measures, reducing the time patients need to wait for a diagnostic procedure.
How might this impact on clinical practice?
This study emphasises the role ESE plays in the assessment of myocardial ischaemia and demonstrates that it is feasible to perform ESE safely and effectively during the ongoing COVID-19 pandemic.
Resuming ESE services with safety measures in place can continue to help make timely diagnosis and enact management of coronary artery disease, improving patient outcomes.
Introduction
Cardiovascular diseases are still the leading cause of morbidity and mortality. They account for approximately 18 million deaths annually, which is significantly higher than the deaths associated with communicable diseases, including the 3.8 million COVID-19 deaths estimated as of the end of June 2021.1–3 Early diagnosis and implementation of evidence-based treatment is key to influencing outcome in patients with cardiovascular disease.4
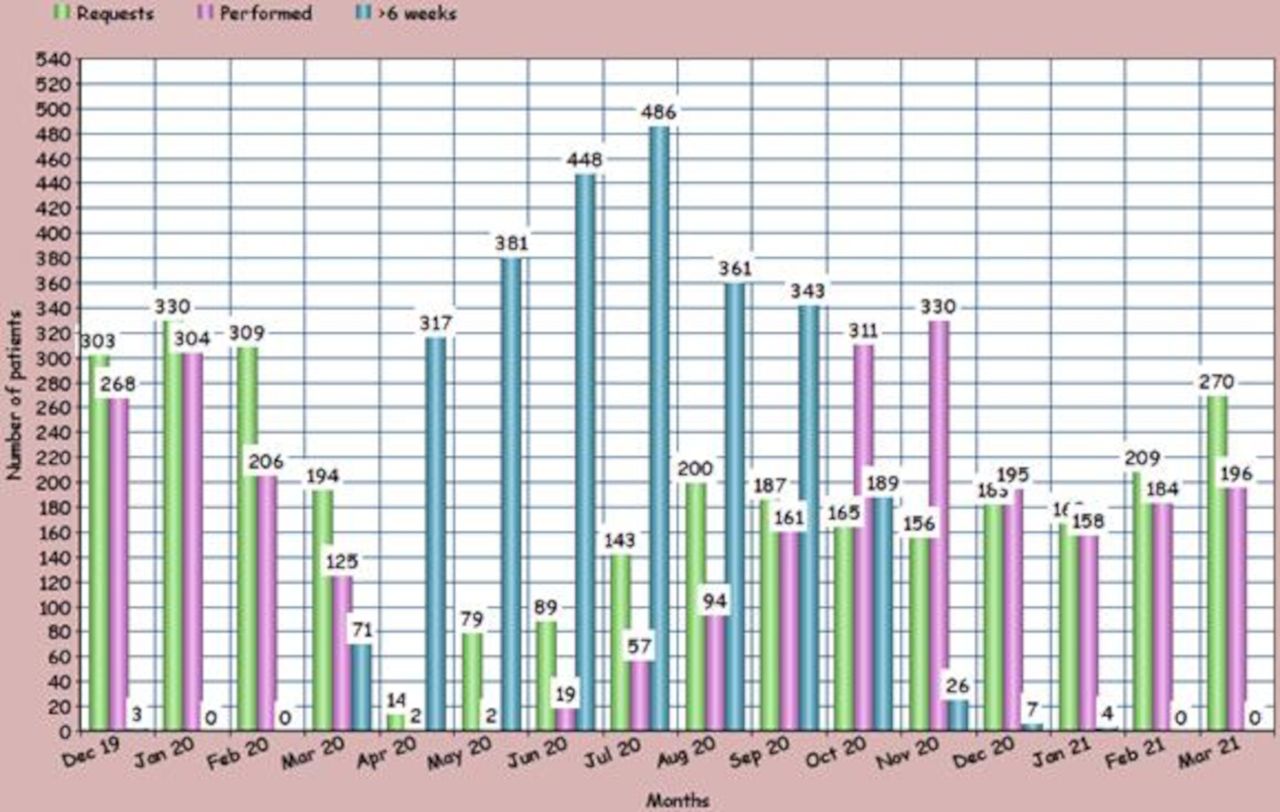
Owing to the strain on resources required to treat patients with COVID-19 and the efforts to prevent its spread, there was a marked disruption in cardiovascular diagnostic services across the world at the start of the pandemic. There was a profound reduction in diagnostic procedures performed particularly for exercise electrocardiography (84%), stress echocardiography (SE) (83%) and transoesophageal echocardiography (76%).5 This was likely due to the aerosolisation risk to staff associated with these procedures at a time when personal protective equipment (PPE) was limited.5 6 In our centre, there was a significant reduction in both the number of requests and SE performed—a drop of 83% (figure 1), especially for exercise stress echocardiography (ESE).
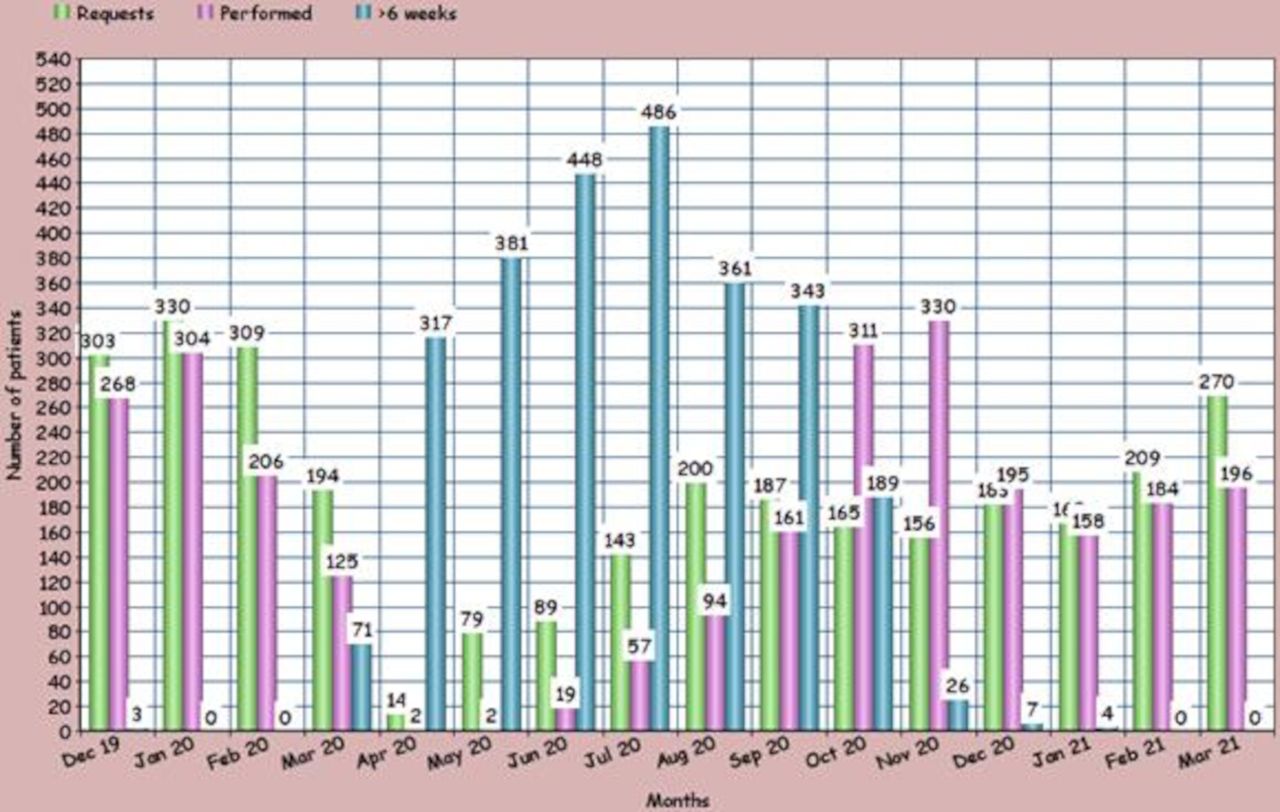
The number of referrals made for stress echocardiography reduced by 95.8% at the peak of the pandemic in April 2020 and the number of stress echocardiograms performed reduced by 99%.
In patients able to exercise with no significant left ventricular dysfunction, ESE is the preferred modality for the assessment of myocardial ischaemia because of its ability to provide information on functional capacity, exercise tolerance and symptoms.7 Additionally, procedure time with ESE is significantly less than that with dobutamine SE. We hypothesised that ESE can be performed safely and efficiently, during the ongoing pandemic, by designing a standard operating procedure incorporating national and local safety guidelines.
Methods
Study design
Between July 2020 and January 2021, immediately after the first UK national lockdown, a total number of 1047 SEs were requested. Baseline data were collected prospectively on the 740 consecutive patients undergoing ESE (cohort 1). The same dataset was collected on patients who underwent ESE prepandemic, between May 2014 and May 2015 (cohort 2), for comparison with cohort 1, in order to address the aims of this study. The data were collected as part of a service evaluation reviewed by London North West University Healthcare NHS Trust Research and Development for which individual consent was not required for inclusion of data in the study.
Patient selection
Patients referred for SE included those from the cardiology outpatient and rapid access chest pain clinics with suspected stable angina, where the chest pain was considered typical or atypical or non-anginal but there remained concerns that the chest pain could be ischaemic. Inpatients included those referred for suspected acute coronary syndrome (ACS) without cardiac enzymes rise and ECG changes or where there was a rise in cardiac enzymes but the clinical suspicion of ACS was low. Patients able to exercise without resting wall thickening abnormality (WTA) or with known fixed WTA underwent ESE. Patients unable to exercise or with new and extensive WTA underwent pharmacological stress for the assessment of viability and ischaemia.
Triage and screening of patients
Patients were prioritised based on the urgency of the referral and risk to the patient attending for the SE according to National Health Service (NHS) advice. Patients did not undergo COVID-19 antigen testing prior to attendance. Patients were screened for symptoms during booking, over the telephone, 24 hours before attendance and screened again during attendance. Patient temperature was monitored at entry points into the hospital. All patients were asymptomatic, afebrile and without clinical suspicion of COVID-19 infection.
Personal protection and ventilation
Personnel were limited to two members directly involved in performing the procedure (operator 1 and 2). Both operators wore a face-fit tested filtering facepiece 3 (FFP3) mask according to the Department of Health and Social Care’s PPE strategy.8 In addition, operator 1 (person acquiring images) wore eye protection, fluid-resistant long sleeved gown and gloves. Operator 2 wore a face-fit tested FFP3 mask, eye protection, apron and gloves. Staff members were further protected by receiving both doses of the COVID-19-Pfizer vaccine by the end of March 2021. Patients wore surgical masks covering both the mouth and nose throughout the procedure. All attempts were made to ensure adequate ventilation in the SE laboratory, moving to a room with two windows that were kept open permanently. CO2 levels were not monitored.
Stress echocardiography
Patients exercised on the treadmill according to the standard Bruce/modified Bruce Protocol. End points included reaching 85% of age-predicted maximum heart rate (HR), significant or symptomatic tachyarrhythmia or bradyarrhythmia, >1 mm ST elevation, >3 mm ST depression without symptoms, >2 mm ST depression with symptoms, systolic blood pressure rise > 230 mm Hg, development of bundle branch block, limiting symptoms and patient’s request for termination. Echocardiographic images of the left ventricle (LV) were obtained at rest in the apical four-chamber, two-chamber and three-chamber views and the parasternal long-axis and short-axis views. The same set of images was acquired immediately after peak exercise, within 60–90 s. Baseline and peak images were displayed side by side for analysis.
Following guidelines on contrast administration, where ≥2 contiguous segments were not visualised adequately during rest or during deep inspiration, mimicking cardiac motion during stress, intravenous echocardiography contrast was used.9 Images were analysed and interpreted together with two expert readers (RS, NC—consultant cardiologists).
Image analyses
Images were interpreted qualitatively for the presence, extent and location of regional wall thickening abnormalities (RWTA). A four-point score (1: normal, 2: reduced, 3: absent, 4: systolic thinning) was used. Systolic wall thickening was scored, using a 17-segment LV model.
Studies were considered normal if all 17 segments demonstrated normal RWTA at baseline and peak stress having achieved >85% or between 80% and 85% of the age-predicted maximum HR provided patients achieved ≥7 metabolic equivalents (METs).
Studies were abnormal for ischaemia with the development of RWTA in any segment at peak exercise. Significant ischaemia was classified as RWTA in ≥3 segments. Studies were non-diagnostic when image quality was insufficient for interpretation at peak exercise and inconclusive when patients were unable to exercise to a workload of at least 7 METs and achieve at least 80% of their age-predicted maximum HR in absence of symptoms or ischaemia.
Follow-up
Data were collected for coronary angiography (CA) and cardiac events, that is, cardiac death, acute coronary syndrome and unplanned revascularisation. Data were obtained from electronic hospital records and the hospital SE/CA database.
Statistical analysis
Initial analyses compared the demographic and baseline characteristics of the two cohorts (2015 and 2020). Continuous variables were all found to be normally distributed and compared between groups using the unpaired t-test. The χ2 test was used to compare between groups for the categorical variables.
Subsequently, due to expected differences in the patient demography of the two groups, analyses were performed to select matching subgroups from each cohort that would share similar characteristics. Matching was performed using propensity score matching. Initially, logistic regression was performed with year (2015 and 2020) as the outcome, and all patient demographics as predictor variables. The fitted values from this analysis (on the logit scale) for each patient were used in the propensity score matching. The propensity score matching was performed on a 1:1 basis, and was performed using the nearest neighbour method. To ensure that the matched groups were similar, patient pairs with the best matches were included in the propensity-matched dataset. Specifically, patient pairs were included in their predicted logits differed by <0.5.
The key outcome variable was rate pressure product (RPP), which was measured on a continuous scale and found to be normally distributed. The unpaired t-test was used to compare this outcome between the two cohorts. First, data from all patients were analysed, with an additional analysis performed using the matched subgroups.
Patient and public involvement
This study was done retrospectively as part of a service evaluation to assess the risk to staff conducting SE investigations during the pandemic. The research question was shaped after patients had undergone the investigation and data were collected. The study design was shaped by input from healthcare providers and researchers and the results will be communicated to help shape services across the NHS.
Results
Study population
Baseline characteristics are shown in table 1. More than half of the study population were males and a third of the patients had a history of coronary artery disease (CAD).
Baseline characteristics of the two groups exercising with and without facemasks before and after propensity score matching
Exercise stress feasibility
Nine patients (1.2%) did not tolerate wearing a mask throughout exercise and removed it briefly at some point during or after exercise. One patient was unable to wear a mask and wore a face shield. Diagnostic tests were achieved in 725 (97.9%) patients. Ultrasound contrast agents were used in 722 (97.5%) patients. ESE haemodynamics and interpretation is shown in table 2.
Results of the exercise parameters between the two groups exercising with and without facemasks after propensity score matching
ESE efficacy
Of the 69 patients with significant ischaemia, 61 patients underwent CA of which 51 (83.6%) demonstrated flow-limiting CAD (>50% diameter stenosis of one or more of left main, left anterior descending, left circumflex or right coronary arteries and their major branches)—measure of positive predictive value (PPV) of ESE. Of these 51 patients, 39 (76.5%) underwent coronary revascularisation—17 (33.3%) underwent percutaneous coronary intervention and 22 (43.1%) coronary artery bypass grafting. The remaining 12 (23.5%) with flow-limiting CAD were managed with medical therapy only. Of the 15 patients with mild ischaemia, 2 patients underwent CA, but none had coronary intervention, disease-modifying medical therapy was implemented in all 15 patients.
During a mean follow-up period of 155 (4.6 months)±44 days, one case of acute myocardial infarction was recorded.
Safety of exercise stress echocardiography
None of the staff directly involved in the ESE procedures displayed any clinical signs or symptoms of COVID-19 and tested negative during recommended twice weekly SARS-CoV-2 antigen rapid qualitative testing.
Propensity-matched analysis
The first set of analyses compared the demographic and baseline characteristics of the two groups. The results suggested statistically significant differences between the 2-year groups for age, hypertension, cholesterol, family history and systolic blood pressure. No difference was observed for diabetes, smoking and HR. Patients from the 2020 cohort were typically older than those from 2015, with a higher proportion of female patients. The 2020 cohort had a lower occurrence of cholesterol and family history, but a higher occurrence of hypertension and higher blood pressure.
Propensity score matching was used to match together individual patients from the two cohorts, however, some matches were not particularly close, therefore further restriction on the patient group was enforced to retain only those patient pairs where the matching was closest. Specifically, patients where the logits were <0.5 were included in the propensity-matched dataset. Using this strategy, 378 patients from each cohort were included.
The analyses comparing the baseline and demographic features of the two cohorts were repeated using the propensity-matched dataset only. The results of the analyses before and after propensity score matching are summarised in table 1.
By design, there was no significant difference in any of the characteristics between the groups using the propensity-matched datasets.
Following this analysis, the difference in outcome variable, rate pressure product, was compared between the two groups. The results suggested when all the data were included, there was a significant difference in outcomes between the groups. RPP values were higher in the 2020 cohort, with a mean difference of 1886 units. Analysis of the propensity-matched dataset showed no evidence in outcome between the group exercising with masks and the group without (table 2). Furthermore, no significant differences were noted in the prevalence and the extent of significant inducible ischaemia or PPV.
Effect on and recovery of ESE service
Peak pandemic number of referrals for SE decreased by 95.8% and number performed reduced by 99% (figure 1). Waiting time <6 weeks, a measure of performance, increased to 96.8% of prepandemic levels (100%) from 26.6% at the start of the study period (July 2020) to the end of the study period (January 2021) (figure 2). By the end of the follow-up period (March 2021), referrals increased 13-fold reaching 81% of the peak prepandemic levels, while waiting time <6 weeks reached 100% (figure 1).

{kind=link}
{kind=link}
Performance is measured by how many patients have been waiting <6 weeks to have a stress echocardiogram (SE) done after a referral has been generated. Immediately prior to the first outbreak of COVID-19, 100% of patients referred for SE underwent the test within 6 weeks of referral. At the height of the pandemic at the end of May 2020, that dropped to 17.2%. During the period of this service evaluation (July 2020–January 2021), there was an increase in 70.2% of performance levels.
Discussion
Very early on during the initial outbreak of COVID-19 every international echocardiography society published guidelines on strategies preventing the spread of COVID-19 during echocardiography procedures, with particular emphasis on ESE, considered an aerosol generating procedure.10 11 These measures included limiting the overall indications for SE and recommended the use of CTCA, and where SE was still being used, priority was to be given to the pharmacological modality over the exercise modality.
Despite the relatively recent guidelines regarding the application of CTCA published by the National Institute for Health and Care Excellence, European Association of Cardiovascular Imaging, American College of Cardiology (ACC) and American Heart Association (AHA),12–14 availability for CTCA remains a challenge, especially in our centre. Notwithstanding, according to both European Society of Cardiology and ACC/AHA guidelines stress echocardiography remains the initial test among other non-invasive modalities for the assessment of CAD. ESE is the first-line investigation for the evaluation of CAD in patients able to exercise, helping to uncover symptoms, assessing the level of exercise when patients become symptomatic and ischaemic and providing haemodynamic data which all have prognostic implications beyond the presence and extent of ischaemia.14 ESE is also useful in assessing the prognostic importance of valve disease particularly when symptoms are discordant with the severity of valve disease.15 Finally, ESE is a relatively rapid test compared with dobutamine SE. For these reasons, ESE is unique compared with other contemporary stress modalities, and hence the importance of developing protocols so that ESE can continue to be performed efficaciously as well as safely.
We sought to investigate the feasibility, efficacy and safety of performing ESE while adopting nationally guided safety procedures during the COVID-19 pandemic, particularly performing exercise testing with a facemask. Diagnostic studies were feasible in 98% of patients, with almost all patients able to tolerate wearing a mask during exercise stress. Efficacy was not compromised compared with pre-COVID-19 SE data and resuming ESE with a revised protocol, resulted in the number of patients waiting >6 weeks reducing to 0%. Our findings were consistent with studies performed by Barbeito-Caamano et al that found performing exercise testing wearing a facemask is feasible and does not influence the functional capacity and clinical results of patients,16 supported further by a retrospective analysis performed by Cano Carrizal and Casanova Rodríguez17 and work done by Peteiro.18
Although ESE has not been classified as an aerosol-generating procedure in the hospital setting, numerous studies showed that both inhalation and exhalation that occur during exercise produce more aerosols.19 20 Subsequently, national and local guidelines suggested improved ventilation in facilities providing ESE services. A typical hospital room requires five air exchanges per hour (one air exchange=15 min) to reduce airborne virus remaining to <1%.21 This requires a 75 min gap between the end of exercise to the entry of the next patient, significantly reducing the number of patients undergoing SE per session. Allowing for only four air exchanges makes a 75 min ESE slot feasible, allowing more patients per session but at the expense of increased residual airborne virus remaining in the room to 2%. We hypothesised that patients wearing masks throughout the procedure would help reduce the amount of potential airborne virus in the room—ensuring that levels <1% would be achieved between cases.22
Theoretically, the wearing of a mask may result in patients underperforming due to difficulty in breathing during exercise, potentially leading to suboptimal ESE results. However, our data showed that the exercise performance was not compromised compared with propensity-matched pre-COVID-19 data in terms of achieving adequate workload, proportion of patients demonstrating myocardial ischaemia and in terms of the severity of myocardial ischaemia induced. The PPV of ESE for the detection of CAD during the pre-COVID-19 and during the COVID-19 period also showed no significant difference. The safety of the protocol was also demonstrated by none of the staff testing positive for the COVID-19 or displaying symptoms.
Clinical implications
ESE can be performed efficaciously and safely. Where other imaging modalities are not available or accessible, ESE can represent the functional imaging modality of choice for the assessment of ischaemia. As ESE can be performed rapidly compared with dobutamine stress echocardiogram (DSE), it can help prevent increase in waiting times, facilitating early assessment of CAD, impacting positively on outcome.
Study limitations
This study was a retrospective analysis, although of a prospectively collected data. Patients were not followed-up to assess for the contraction of the COVID-19 virus, postprocedure.
Conclusion
By adopting relevant safety protocols during the ongoing COVID-19 pandemic, performing ESE is feasible, efficacious and safe for healthcare professionals. It has a major impact on the total number of SE that can be performed which significantly reduced waiting times.
Data availability statement
Data are available on reasonable request. The final anonymous dataset that supports the findings of this study are available from the corresponding author, RS, on reasonable request.
Ethics statements
Patient consent for publication
Acknowledgments
We thank Paul Bassett for his valuable assistance with the statistical methodology of the manuscript.
References
Footnotes
Contributors RS conceptualised the work and is the guarantor in addition to monitoring data collection, writing the statistical analysis plan, analysing data and reviewing the draft paper. RH collected and analysed the data, and drafted the paper. CB collected data. NC revised the draft paper.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests RS and RH have received speaker fees from Bracco Imaging, Milan, Italy and Lantheus Medical Imaging, Boston, USA and Philips Healthcare, Eindhoven, The Netherlands. All other authors have no conflict of interest to declare.
Provenance and peer review Not commissioned; externally peer reviewed.