Article Text

Abstract
Background The clinical significance of peak troponin levels following ST-elevation myocardial infarction (STEMI) has not been definitively established. The purpose of this study was to examine the relationship between peak high-sensitivity cardiac troponin T (hs-cTnT) and all-cause mortality at 30 days and 1 year, and left ventricular ejection fraction (LVEF) in STEMI.
Methods A single-centre retrospective observational study was conducted of all patients with STEMI between January 2015 and December 2017. Demographics and clinical data were obtained through electronic patient records. Standard Bayesian statistics were employed for analysis.
Results During the study period, 568 patients presented with STEMI. The mean age was 63.6±12 years and 76.4% were men. Of these, 535 (94.2%) underwent primary percutaneous coronary intervention, 12 (2.1%) underwent urgent coronary artery bypass and 21 (3.7%) were treated medically. Mean peak hs-cTnT levels were significantly higher in those who died within 30 days compared with those who survived (12 238 ng/L vs 4657 ng/L, respectively; p=0.004). Peak hs-cTnT levels were also significantly higher in those who died within 1 year compared with those who survived (10 319 ng/L vs 4622 ng/L, respectively; p=0.003). The left anterior descending artery was associated with the highest hs-cTnT and was the most common culprit in those who died at 1 year. An inverse relationship was demonstrated between peak hs-cTnT and LVEF (Pearson’s R=0.379; p<0.00001).
Conclusions In STEMI, those who died at 30 days and 1 year had significantly higher peak troponin levels than those who survived. Peak troponin is also inversely proportional to LVEF with higher troponins associated with lower LVEF.
- STEMI
- PRIMARY PCI
- Biomarkers
Data availability statement
Data are available upon reasonable request. All data relevant to the study are included in the article or uploaded as supplementary information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Existing studies have examined the relationship between cardiac troponins and mortality in patients with acute coronary syndromes, but with varying results. Recent literature suggests there is no prognostic value to peak troponin T sampling in patients with ST-elevation myocardial infarction (STEMI) treated with primary percutaneous coronary intervention.
WHAT THIS STUDY ADDS
This study establishes a significant link between high-sensitivity peak troponin T levels and both all-cause mortality and ventricular dysfunction in patients with STEMI. We studied all acute STEMI cases over a 3-year period at a single centre, and found higher peak high-sensitivity cardiac troponin T levels in patients who died at 30 days and 1 year post hoc, as well as in those with subsequently reduced left ventricular ejection fraction.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE AND/OR POLICY
We suggest that this justifies performing troponin T sampling at 24–48 hours post-admission as an effective non-invasive method for stratifying patients’ risk of mortality and ventricular dysfunction.
Background
Atherosclerotic cardiovascular disease contributes substantially to morbidity and mortality worldwide. Recent epidemiological data from the Global Burden of Disease study estimates that approximately 9 million deaths were attributed to ischaemic heart disease in 2017, making it the leading cause of global mortality, a position it has retained for greater than two decades.1
High-sensitivity cardiac troponin T (hs-cTnT) assays have been recognised for improving diagnostic accuracy in the early detection of acute myocardial infarction and for their potential in risk stratification for patients with acute coronary syndromes.2 Several studies have demonstrated worse clinical outcomes with higher troponin levels in patients with non-ST-elevation myocardial infarction (NSTEMI).3–5 However, the clinical significance of peak troponin levels in patients following STEMI is less certain and requires further research.5 6 Most previous studies on the prognostic value of cardiac troponins in patients with STEMI derived from prospective clinical trials, often with highly selective inclusion/exclusion criteria or small sample size, thus not reflecting the entire spectrum of STEMI presentations in daily practice.7–9 Other studies focused on admission levels of troponin or values at specific time points instead of peak values.10–12 In this study we aimed to characterise the predictive value of peak hs-cTnT levels in relation to all-cause mortality and left ventricular function in a real-world cohort of patients with STEMI.
Methods
Study design and population
This was a retrospective, observational study of patients who were admitted to a single centre from January 2015 to December 2017 with acute STEMI. This 24-hour primary percutaneous coronary intervention centre serves a population of approximately 473 000 residents in the mid-west of Ireland. Patients with STEMI were identified as per standard diagnostic criteria at presentation and entered prospectively into a local STEMI database.13 Inclusion criteria were the diagnosis of acute STEMI, existing angiography and an hs-cTnT value documented on index admission. Patients with a final primary diagnosis of unstable angina, NSTEMI or false-positive STEMI were excluded from the study population. Baseline demographic and angiographic data were obtained by review of electronic medical records and patient charts. The peak hs-cTnT value measured within hospitalisation on an electrochemiluminescence immunoassay, Elecsys Troponin T-high sensitive by Roche Diagnostics, was recorded.
Outcomes
The primary endpoint of this study was all-cause mortality within 30 days and 1 year of the index admission. Left ventricular ejection fraction (LVEF) at discharge, mortality data and hospital readmissions for non-culprit repeat revascularisations within 1 year were identified from echocardiographic and angiographic reports, and electronic patient records.
Statistical analysis
Patients are divided into two groups as survivors and non-survivors in accordance with 1-year outcomes. Continuous variables are expressed as the mean (±SD) or median [IQR], and categorical variables as a number and percentage (%). The normality of data distribution was analysed with the Kolmogorov-Smirnov test. Univariate analysis was performed using the Mann-Whitney U test for continuous variables, and Fisher’s exact test for categorical variables between the survivor and non-survivor groups. Standard Bayesian statistical analysis was performed; one-way analysis of variance (ANOVA) was used to compare the means of three or more variables. Pearson correlation was performed to determine an association between statistically significant continuous variables and peak troponin T levels. All statistical analyses were performed using IBM SPSS Statistics V.25. Hypothesis testing was two-tailed, and a p value of ≤0.05 was accepted as statistically significant.
Patient and public involvement
Individual patients and/or the public were not directly involved in the design or conduct or reporting of this study.
Results
Baseline characteristics
Of the 646 STEMI alerts from January 2015 to December 2017, 568 patients (186 in 2015, 194 in 2016 and 188 in 2017) were classified as true STEMIs, had available angiography and hs-TnT measurements and were included in the final analysis. Baseline characteristics for the entire cohort, stratified by survival or mortality, are shown in table 1. The mean age was 63.6±12 years, and 434 patients (76.4%) were men. Two hundred and twenty-four patients (39.4%) had suffered from an anterior infarction. Five hundred and thirty-five patients (94.2%) received primary percutaneous coronary intervention, 12 (2.1%) had urgent coronary artery bypass and 21 (3.7%) were treated medically. Mean creatinine was 95.6±76.1 µmol/L. Compared with the survivor group, patients in the non-survivor group exhibited greater age, higher creatinine (170.7±122.1 µmol/L vs 88.3±65.6 µmol/L, p<0.001), and worse LVEF (40% vs 50%, p<0.001; Cramer’s V 0.179, p=0.011). Mortality rate was marginally higher in women than men (13 (9.7%) vs 37 (8.5%)), but this difference was not statistically significant (p=0.727). Coronary culprit vessels included: 220 (38.7%) left anterior descending artery (LAD), 227 (40.0%) right coronary artery (RCA), 95 (16.7%) left circumflex artery, 7 (1.2%) left main stem, 1 (0.2%) ramus intermedius and 18 (3.2%) multi-vessel involvement or indeterminate culprit. The LAD was the culprit vessel for the majority of patients in the non-survivor group and the RCA was the most frequent culprit vessel in the survivor group (p=0.009).
Baseline characteristics among patients with STEMI and association with 1-year mortality (N=568)
High-sensitivity cardiac troponin T levels and clinical outcomes
Among all patients with STEMI, the median peak hs-cTnT was 3110 ng/L and mean was 5124 ng/L (range 20–57 875 ng/L) (reference range <14 ng/L). Peak hs-cTnT was measured at a median of 1 [0–1] day from admission. The all-cause 30-day and 1-year mortality rate was 6.2% and 8.8%, respectively, for the entire cohort. As shown in table 2, 99 patients (17.9%) were readmitted for 1-year non-culprit vessel revascularisation, and the LAD was the most frequently revascularised vessel within this group.
Clinical outcomes in patients with STEMI within 1 year (n=568)
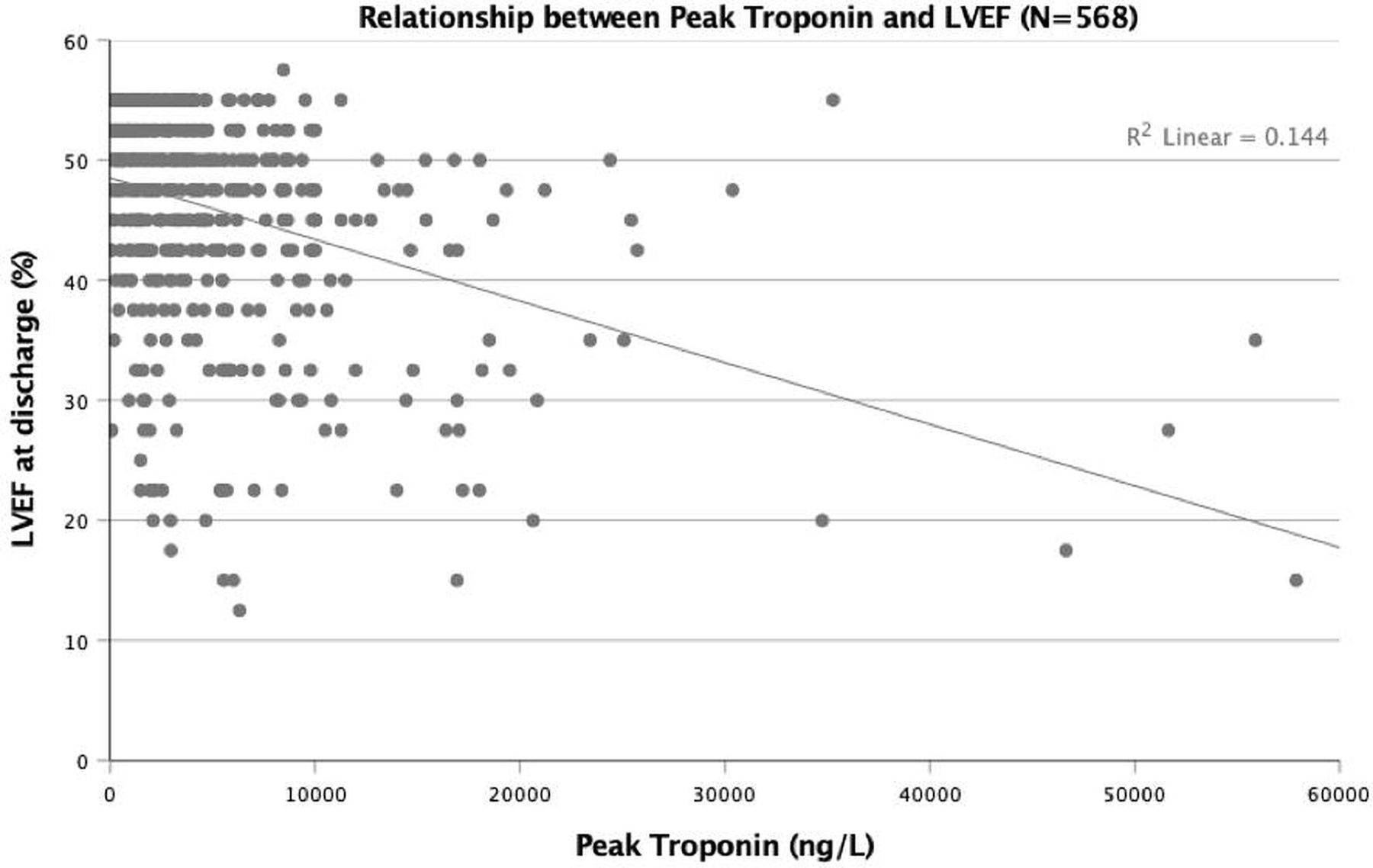
Mean peak hs-cTnT levels were significantly higher in the 1-year non-survivor group compared with the survivor group (10 319 ng/L vs 4622 ng/L, respectively; p=0.003). Peak hs-cTnT levels were also significantly higher in those who died within 30 days compared with those who survived (12 238 ng/L vs 4656 ng/L, respectively; p=0.004; table 3). One-way ANOVA analysis identified significant differences in peak troponin between culprit vessels; LAD was associated with the highest hs-cTnT (figure 1). A moderate relationship between peak hs-cTnT and LVEF was also demonstrated (Pearson’s R=0.379, p<0.00001; figure 2).

Differences in peak troponin between culprit vessels at index admission. Left anterior descending (LAD) was associated with the highest high-sensitivity cardiac troponin T. RCA, right coronary artery.

{kind=link}
{kind=link}
Peak troponin has a moderate relationship with left ventricular ejection fraction (LVEF), Pearson’s correlation, r=−0.379; p<0.01.
Peak troponin-T levels among patients with STEMI and association with 30-day mortality (n=568)
Discussion
In this study we investigated whether hs-cTnT, a myocardial contractile protein, predicts all-cause mortality and left ventricular dysfunction in a nationally representative Irish population of patients with acute STEMI. Our results suggest that peak hs-cTnT is independently associated with an increase in all-cause mortality and a reduction in LVEF.
Cardiac troponins have been known to correlate with surrogate markers of worse prognosis, including larger infarct size, poor left ventricular remodelling and microvascular obstruction.14 15 However, at a time when primary percutaneous coronary intervention (PCI) has become the standard of care across the world, there is little evidence of an independent relationship between hs-cTnT levels and clinical outcomes in patients with STEMI. Several studies have examined the relationship between troponin and mortality, but with conflicting results reported with respect to outcome prediction from cardiac troponin levels.6–9 Kurz et al performed serial hs-cTnT measurements on 82 patients presenting with acute STEMI, finding that a single hs-cTnT measurement on Day 4 post-STEMI was independently associated to mortality, target vessel revascularisation and recurrent myocardial infarction at a mean follow-up of 205 days. In 2013, Boden et al assessed the prognostic value of serial hs-cTnT levels at 6-hour intervals following STEMI in 188 patients, observing that the 24-hour hs-cTnT value after onset of symptoms was the best predictor of adverse outcomes of all-cause mortality, defibrillator implantation and heart failure, at 1 year post-STEMI follow-up. Correspondingly, our study also found peak hs-cTnT values to commonly present at 24 hours after symptom onset. In comparison, a study by Buber et al on 175 patients with STEMI found that peak levels of high-sensitivity cardiac troponin I (hs-cTnI) at 8 hours were independent predictors of all-cause mortality, repeated myocardial infarction and in-hospital heart failure. Collectively, these studies have offered key insights into the role of cardiac troponins in STEMI. However, most of these earlier studies focused on strict gender or age groups, cardiac troponin-I or examined smaller sample sizes, invariably excluding patients with multiple comorbidities. Conversely, the large population studied here consisted of a broad range of unselected patients with STEMI at a tertiary care hospital, resembling more real-world clinical scenarios in daily practice and reducing selection bias. In contrast to previous investigations, a recent study by Cediel et al9 demonstrated that peak levels of both hs-cTnI and hs-cTnT assays do not provide significant prognostic information in the prediction of major adverse cardiovascular and cerebrovascular events at 30 days or 1 year of follow-up in consecutive patients with STEMI treated with primary PCI (n=1260). Notably, pre-procedural hs-cTn levels were excluded from the analysis in this study.9
Limitations
The data presented in this study is non-randomised and should be interpreted within the inherent limitations of a registry-based study. Our single-centre, retrospective approach prevented absolute control of indeterminate confounding factors, which may have contributed to the observed association between hs-cTnT and all-cause mortality. In accordance with the study’s retrospective design, we used an existing electronic medical record of patient data without additional verification or secondary adjudication of diagnoses. The use and interpretation of echocardiography, coronary angiography and revascularisation was not standardised, but rather, left to each treating physician; therefore, there will have been some variance in the recorded degree of significant coronary artery disease or quantifiable change in LVEF at follow-up. Finally, the mortality rate in our population at a single-centre was too low to perform subgroup analyses delineating the causes of mortality; however, this is in keeping with similar studies in the modern era of primary percutaneous intervention.6 16
Conclusions
In this STEMI cohort, patients who died at 30 days and 1 year had significantly higher peak troponin levels than those who survived. Peak troponin also had a strong negative correlation with LVEF, where higher troponin levels were associated with lower LVEF. While the cost-effectiveness of performing routine troponins in STEMI is debatable, there may be a justification for performing a single troponin sample at ~24–48 hours post admission to non-invasively stratify patients according to risk of mortality and left ventricular dysfunction.
Data availability statement
Data are available upon reasonable request. All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
Ethics approval
The local Research Ethics Committee, the Quality and Safety Department under the UL Hospitals Group and Health Service Executive in Ireland, approved this study.
Footnotes
Presented at This study was presented as an abstract at the Irish Cardiac Society Annual Scientific Meeting & AGM, Thursday, 17 October 2019 to Saturday, 19 October 2019, in Galway, Ireland.
Contributors NK carried out the initial analyses, drafted the manuscript and reviewed and revised the manuscript. AB contributed to study design, analyses and interpretation of data and reviewed and revised the manuscript. CO, AI, AI and SA contributed to conception and design of the study, and reviewed the manuscript. CA and CC recruited patients for the study, contributed to the Cardiology STEMI database and reviewed the manuscript. TJK conceptualised and designed the study, supervised data analyses and collection, critically reviewed and revised the manuscript, and is the guarantor. All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.