Article Text

Abstract
Background The diagnosis of infective endocarditis (IE) is based on the modified Duke/European Society of Cardiology (ESC) 2015 clinical criteria. The sensitivity of the criteria is unknown in South Africa, but high rates of blood culture negative endocarditis (BCNIE), coupled with a change in the clinical features of IE, may limit the sensitivity.
Methods The Tygerberg Endocarditis Cohort study prospectively enrolled patients with IE between November 2019 and June 2021. A standardised protocol for organism detection, with management of patients by an Endocarditis Team, was employed. Patients with definite IE by pathological criteria were analysed to determine the sensitivity of the current clinical criteria.
Results Eighty consecutive patients with IE were included of which 45 (56.3%) had definite IE by pathological criteria. In patients with definite IE by pathological criteria, 26/45 (57.8%) of patients were classified as definite IE by clinical criteria. BCNIE was present in 25/45 (55.6%) of patients and less than three minor clinical criteria were present in 32/45 (75.6%) of patients. The elevation of Bartonella serology to a major microbiological criterion of the modified Duke/ESC 2015 clinical criteria would increase the sensitivity (57.8% vs 77.8%; p=0.07).
Conclusion The sensitivity of the modified Duke/ESC 2015 clinical criteria is lower than expected in patients with IE in South Africa, primarily due to the high rates of Bartonella-associated BCNIE. The elevation of Bartonella serology to a major microbiological criterion, similar to the status of Coxiella burnetii in the current criteria, would increase the sensitivity. The majority of patients with definite IE by pathological criteria had less than three minor criteria present.
- Endocarditis
- Echocardiography
- Delivery of Health Care
Data availability statement
Data are available on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known about this subject?
The sensitivity of the modified Duke/European Society of Cardiology 2015 clinical criteria for the diagnosis of infective endocarditis (IE) is unknown in South Africa, a country with high rates of blood culture negative IE and low prevalence of Coxiella burnetii-associated IE.
What does this study add?
The sensitivity of the current clinical criteria is lower than expected in a South African cohort of patients with IE by pathological criteria. The lower than expected sensitivity is due to the high rates of Bartonella-associated IE coupled with a low incidence of minor criteria in patients with IE.
How might this impact on clinical practice?
The elevation of Bartonella serology to a major microbiological criterion, similar to the status of Coxiella burnetii in the current criteria, may increase the sensitivity of the current clinical criteria.
Introduction
The clinical diagnosis of infective endocarditis (IE), despite advances in both imaging technologies and techniques of culturing organisms, remains challenging.1 Current clinical diagnosis of IE is based on the modified Duke/European Society of Cardiology (ESC) 2015 clinical criteria for the diagnosis of IE, with the presence of typical imaging features of IE and the identification of a causative organism (predominantly from blood cultures) the two major components of the criteria.2 In the absence of both major criteria being present, either one major criterion with three or more of the minor criteria or no major criteria with all five minor criteria would classify patients as definite IE.2 3
The gold standard for the diagnosis of IE remains histopathological examination revealing active endocarditis or the presence of microorganisms within either a vegetation or valve tissue.2 The Duke criteria, with a reported sensitivity of 70%–80%, misclassify a number of patients with confirmed IE by pathological criteria, as possible IE.2–5 This is driven primarily by a lower sensitivity in patients with blood culture negative IE (BCNIE), prosthetic valve endocarditis (PVE) and device-related endocarditis (DRE).2 4 Modifications were made to the original Duke criteria to increase the sensitivity of the clinical criteria in these groups of patients. The modified Duke criteria elevated positive serology for Coxiella burnetii to a major microbiological criteria and expanded the major imaging criteria to include transoesophageal echocardiography (TEE).4 6 Coxiella burnetii, an obligate intracellular bacterium that cannot be cultured on synthetic culture media, is the the most common cause of BCNIE in European cohorts and its serological addition to the modified Duke criteria has increased the sensitivity of the criteria in these cohorts.2 4 Subsequent to the modified Duke criteria, the modified Duke/ESC 2015 clinical criteria were introduced; this expanded the major imaging criteria to include typical imaging features by cardiac computerized tomography (CT) with or without 18-fluorodeoxyglucose positron emission tomography (18FDG-PET).2 4 This expansion of the major imaging criteria were specifically introduced to increase the sensitivity of the criteria in patients with PVE or DRE.2 The minor criteria have remained mostly unchanged since the introduction of the Duke criteria, although many of the clinical features retained in the minor criteria are rarely encountered in patients with IE today.1 7
In South Africa, IE is characterised by high rates of BCNIE (up to 60%) and very low rates of Coxiella burnetii-associated IE which means that the majority of patients with IE will not fulfil the major microbiological criteria.1 8–11 The high rates of BCNIE in South Africa appear to be related to a combination of antibiotic use prior to blood culture sampling and causative organisms that are difficult to culture, particularly the Bartonella species.8 9 12 13 The classification of patients with BCNIE into definite or possible IE according to current clinical criteria therefore often hinge on the presence of a number of minor criteria.2 A decrease in the number of patients with predisposing heart disease14 coupled with the observed decrease in the presence of Roth spots, Janeway lesions and Osler nodules is a likely reason for the higher proportion of possible IE (up to 35%) reported in more recent cohorts when compared with older cohorts of patients treated for IE in South Africa.8 9
Recently, Bartonella species has emerged as an important cause of BCNIE in the Western Cape region of South Africa.12 13 The gold standard for the microbiological diagnosis of Bartonella-associated IE is PCR and sequencing of the bacterial 16S rRNA gene performed directly on the affected valve tissue.12 Bartonella serology, performed on venous blood samples, may suggest active Bartonella infection but does not confirm Bartonella-associated IE. In the setting of patients with clinical and imaging features of IE with negative blood cultures, an IgG titre above 1:128 and/or IgM titre above 1:40 is suggestive of infection with Bartonella species and makes it a likely cause of BCNIE.12 15 Positive serology for Bartonella species in patients with BCNIE, in contrast to positive serology for Coxiella burnetii, currently represents only a minor criterion in the current modified Duke/ESC 2015 clinical criteria.2
A prospective cohort of patients, presenting with IE in our region, was analysed to describe the typical clinical features observed. From this cohort, a group of patients with definite IE by pathological criteria2 was selected to determine the sensitivity of modified Duke/ESC 2015 clinical criteria and determine possible causes of misclassification.
Methods
Study design and participants
Consecutive patients presenting with IE to the Division of Cardiology, Department of Medicine at Tygerberg Hospital in Cape Town, South Africa, between November 2019 and June 2021 were prospectively enrolled in the Tygerberg Endocarditis Cohort study as previously described.12 13 ,14Patients with known or newly diagnosed malignancy were excluded. The Division of Cardiology at Tygerberg Hospital is a public sector tertiary referral centre that serves a population of approximately 2.4 million people.16 Patients with features of IE presenting to hospitals within the referral network are referred to Tygerberg Hospital for definitive care.17 The Division of Cardiology is categorised as a high volume centre for the diagnosis and management of IE.18 Patients were managed by an Endocarditis Team following diagnostic and management criteria as set out by current guidelines.2
Clinical evaluation
All patients were evaluated by at least one member of the Endocarditis Team on presentation and clinical features, specifically the presence of criteria for the diagnosis of IE, were documented. Thereafter patients were evaluated daily, the presence and timing of any major adverse events (death, embolic events and renal failure requiring dialysis) documented and antimicrobial therapy tailored as microbiology results became available. A weekly Endocarditis Team meeting was held to review all current cases and discuss management decisions.
Echocardiographic evaluation
Enrolled patients underwent transthoracic echocardiography with the majority of patients also undergoing TEE.19 20 In addition to a standard echocardiographic evaluation,19 20 a detailed assessment of the underlying heart and valvular structure, with a specific focus on the presence of underlying predisposing heart disease or endocardial abnormality, was performed.2 5 14 21–27
Additional imaging
Cardiac CT with or without 18FDG-PET scanning as well as cardiac MRI were performed at the discretion of the Endocarditis Team.
Microbiological assessment
A standardised stepwise protocol for organism detection was utilised to identify the common causative organisms of IE and to minimise the rate of BCNIE.1 12 Blood cultures were collected and processed according to current international guidelines and as previously reported.2 12 If no pathogen was isolated from blood cultures after 5 days of incubation, patients were defined as having BCNIE.
All patients with BCNIE underwent further testing(all tests performed in parallel), including:
Serology was performed using indirect immunofluorescence assays (IFA) for detection of IgM and IgG antibodies to Bartonella henselae and Bartonella quintana (FOCUS Diagnostics, Cypress, California, USA). An IgG titre above 1:128 and/or IgM titre above 1:40 was considered positive for Bartonella henselae and Bartonella quintana.12 15 Specific antibodies to Coxiella burnetii were also determined by IFA, with an IgG phase 1 titre above 1:800 considered positive.2 Enzyme immunoassays were performed to detect IgM and IgG antibodies to Brucella species, Legionella pneumophila (EUROIMMUN, Lübeck, Germany) and Mycoplasma pneumoniae (EUROIMMU).
Broad range PCR and sequencing was performed on negative blood culture bottles for detection of the bacterial 16S rRNA and fungal ITS2 genes.
BACTEC Myco/F Lytic vials(Becton Dickinson, San Jose, California, USA) were collected for the isolation of Mycobacteria, including Mycobacterium tuberculosis (MTB) and non-tuberculous Mycobacteria.
Testing for antinuclear antibodies and anti-cardiolipin antibodies.
A sample of heart valve tissue was collected from all patients who underwent surgery (or at post mortem) and this was submitted for:
Bacterial and fungal culture.
Broad range PCR and sequencing of 16S rRNA and ITS2.
Histopathological examination to detect bacteria and fungi, as well as histopathological features of IE.
Statistical analysis
Statistical analysis was done using SPSS V.27 for iOS and JASP (V.0.14.1) for iOS.
Continuous variables were reported as mean with SD if normally distributed, alternatively as median with IQR. Categorical variables were reported as counts and percentages. To compare the diagnostic sensitivities of the modified Duke/ESC 2015 clinical criteria and our proposed elevation of Bartonella serology to a major microbiological criterion, the χ2 test was performed. For all analyses, two-sided tests of significance were performed with an alpha of 0.05.
Results
A total of 80 consecutive patients with IE were included with the characteristics at diagnosis summarised in table 1. Histopathological samples were available in 43 of 46 patients who underwent surgery and from two post mortems performed. Definite IE by pathological criteria was confirmed in all 45 of these cases. In patients with definite IE by pathological criteria, 26/45 (57.8%) of patients were classified as definite IE by clinical criteria (table 2). BCNIE was present in 25/45 (55.6%) of patients and more than two minor clinical criteria were present in the minority of patients (24.4%). Aetiologies associated with the misclassification of patients as ‘possible IE’ by clinical criteria are summarised in table 3. The elevation of Bartonella serology to a major microbiological criterion of the modified Duke/ESC 2015 clinical criteria would have increased the sensitivity to accurately diagnose definite IE (57.8% vs 77.8%;p=0.07) (figure 1).
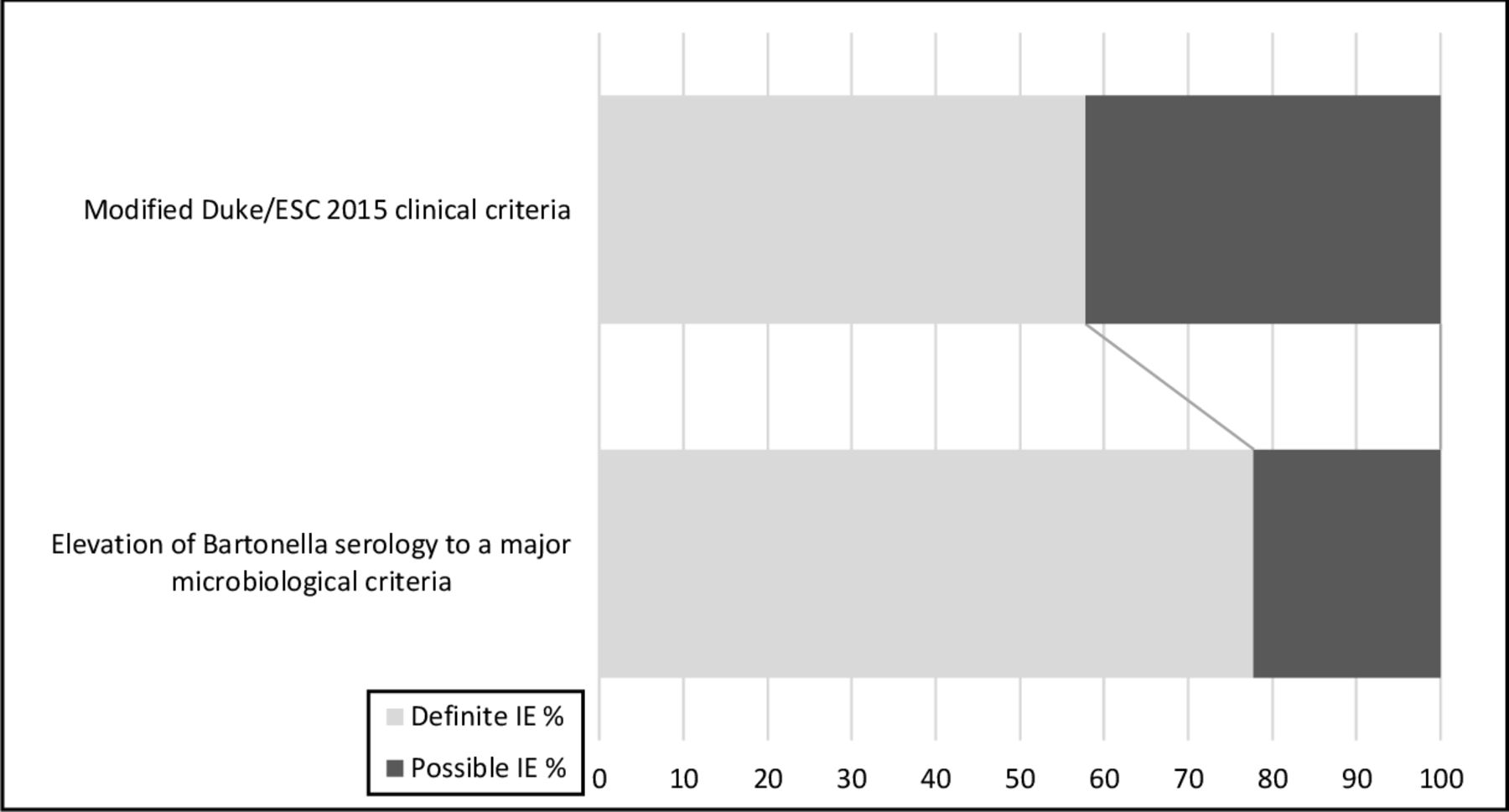
Sensitivity of the modified Duke/ clinical criteria with and without the elevation of Bartonella serology to a major microbiological criterion in patients with confirmed IE by pathological criteria (n=45). ESC, European Society of Cardiology; IE, infective endocarditis.
Baseline characteristics at diagnosis
Modified Duke/ESC 2015 clinical criteria in patients with definite infective endocarditis by pathological criteria and those without histology available
Causes of misclassification of patients with BCNIE as possible rather than definite endocarditis by the modified Duke/ESC 2015 clinical criteria
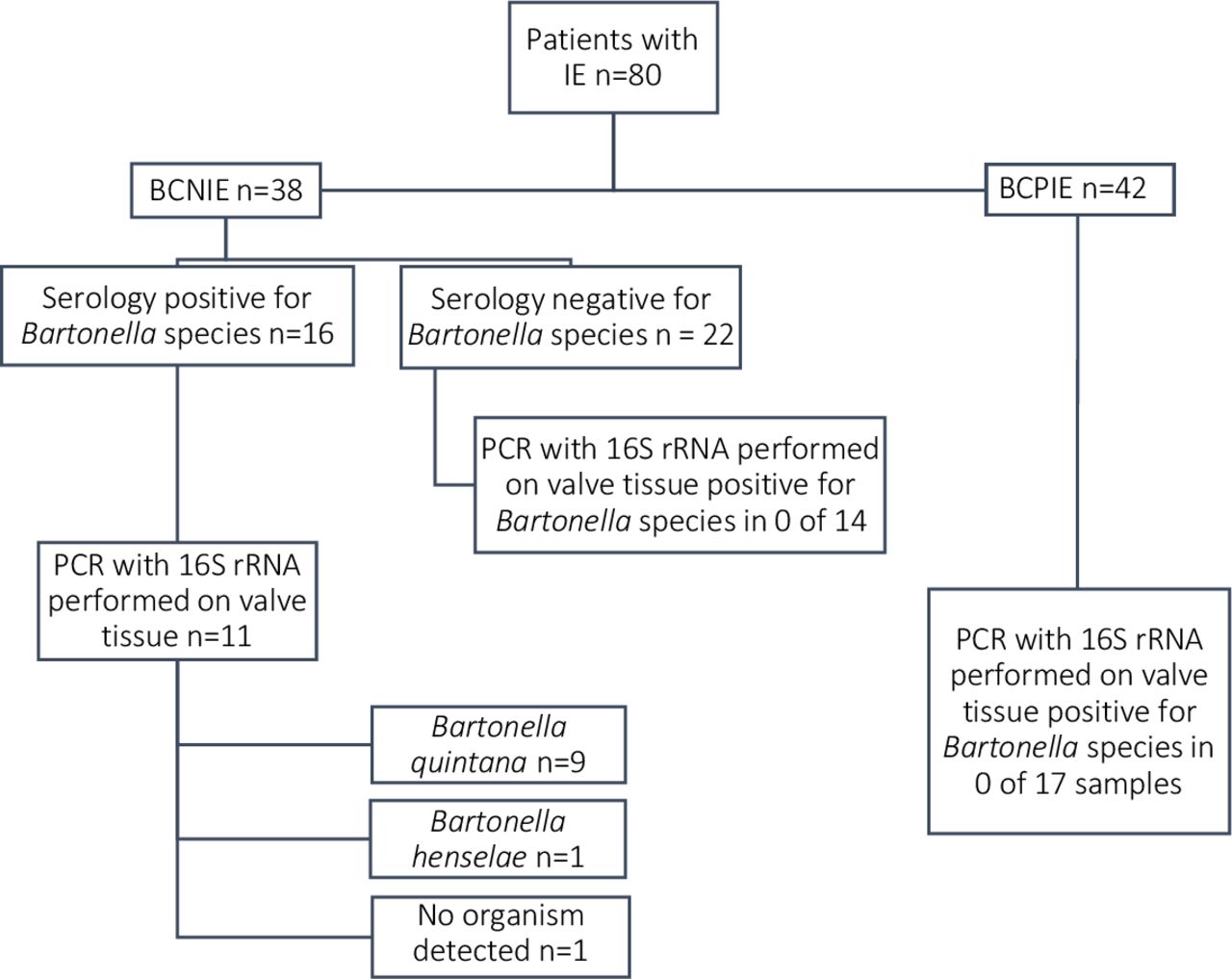
Bartonella serology was positive in 16/38 (42.1%) of patients with BCNIE in our cohort (figure 2). Eleven of the 16 patients underwent surgery with definite IE confirmed by pathological criteria in all 11 (100%) patients. PCR performed on valve tissue identified the causative organism as Bartonella quintana in nine patients and Bartonella henselae in one patient. None of the patients with BCPIE who had PCR performed on their valve tissue, returned positive PCR for Bartonella species. Similarly, only patients with BCNIE and positive serology returned positive PCR for the Bartonella species (figure 2).

{kind=link}
{kind=link}
Analysis of patients with Bartonella serology suggesting active infection. BCNIE, blood culturenegative infective endocarditis; BCPIE, blood culture positive infective endocarditis; IE, infective endocarditis.
Discussion
We have observed a lower than expected sensitivity (57.8%) of the modified Duke/ESC 2015 clinical criteria2 to classify patients with definite IE by pathological criteria, as such.2 28 The sensitivity in our cohort is lower than reported in first-world cohorts where sensitivities of up to 80% are frequently reported.2 4 29 Although no previous study has evaluated the sensitivity of either the original Duke criteria or subsequent modifications in a South African cohort, a recent retrospective cohort of patients treated for IE have reported rates of definite IE of 59%–64%.9
The likely causes of the clinical misclassification of patients with definite IE by pathological criteria as possible IE in our cohort, are the high rate of BCNIE (55.6%) with no cases of Coxiella burnetii (absence of a major criteria), coupled with a low prevalence of the minor criteria. In this group of patients with only a single major criteria, three or more minor clinical criteria must be present to fulfil the criteria for definite IE.2 Three or more minor clinical criteria were present in only 24.4% of our cohort with definite IE by pathological criteria (table 2). The minor clinical criteria comprise a number of clinical features that have decreased in prevalence in the developed world since the original publication of the Duke criteria.1 5 7 We have observed a similar trend with the majority of patients (75.6%) with definite IE by pathological criteria having less than three of the minor criteria present (table 2).
The high rate of BCNIE was predominantly caused by non-culturable organisms, specifically Bartonella species, rather than antibiotic use prior to blood culture sampling (tables 1 and 3). The detection of active Bartonella infection with serology in patients with BCNIE2 12 15 is currently regarded as a minor criterion in contrast to serology for Coxiella burnetii which is part of the major criteria.2 The addition of Coxiella burnetii serology to the current guidelines was motivated on the basis that Coxiella burnetii is a common cause of BCNIE in European cohorts, specifically in France, and upgrading serological detection from a minor to a major criterion increased the sensitivity of the guideline criteria.2 4 We have previously reported the emergence of Bartonella species as a cause of BCNIE12 13 and the elevation of positive Bartonella serology to the major criteria could be motivated on a similar basis as the elevation of serology for Coxiella burnetii to the major criteria. In this cohort of patients with definite IE by pathological criteria, the elevation of Bartonella serology to a major microbiological criteria would increase the sensitivity of the clinical criteria to 77.8% (figure 1), which is similar to the reported sensitivities of the current modified Duke/ESC 2015 clinical criteria in developed-world cohorts.2 6 Serology for Bartonella species was positive in 11 of the patients with BCNIE who underwent surgery, with 16S rRNA PCR performed on valve tissue confirming Bartonella quintana in nine patients and Bartonella henselae in one patient (figure 2). This also suggests a low false-positive rate for the serological test when used in patients with a high pre-test probability for IE. One patient with active systemic lupus erythematosus (SLE) returned positive serology for Bartonella species, Brucella, Mycoplasma and Coxiella burnetii; this was likely due to cross-reactivity of the antibodies associated with SLE.12 Serology for Bartonella after treatment of SLE was negative and PCR performed on the surgical specimen was negative for all these organisms. Importantly, none of the patients with BCPIE or BCNIE with negative serology for Bartonella species returned positive 16 rRNA PCR for Bartonella species (figure 2).
The frequency of occurrence of some of the clinical features incorporated in the minor criteria of the modified Duke/ESC 2015 clinical criteria was low in this study (table 2) and contributed to the lower than expected sensitivity of these criteria. This is particularly evident in this cohort because of the high prevalence of Bartonella-associated IE. Immunological features such as Roth spots, Janeway lesions and Osler nodules were rarely detected, similar to previous reports from South Africa.8 The most commonly observed clinical features were new-onset dyspnoea, clubbing, anaemia, haematuria and evidence of embolic events. When comparing our cohort to previous cohorts of IE in South Africa, the presence of fever and a predisposing endocardial abnormality was lower8 9 while the proportion of patients with intravenous drug use remained low (table 1). A possible explanation for the higher than expected rate of clubbing and lower rate of documented fever may be the proportion of patients with Bartonella-associated IE in our cohort. The majority of our patients with Bartonella-associated IE had clubbing (15/16; 93.8%). In contrast, fever was only documented in one patient (6.3%) with Bartonella-associated IE.
A significant number of patients presented with clinical features of acute or acute on chronic severe valvular regurgitation, with the majority confirmed to be either acute or acute on chronic severe by echocardiographic criteria.21 This suggests that a significant number of patients present early with acute IE and may offer a partial explanation for the decrease in clinical features listed in the minor criteria when compared with the era when viridans streptococci was the predominant organism.
Conclusion
We have observed a lower than expected sensitivity (57.8%) of the modified Duke/ESC 2015 clinical criteria to diagnose definite IE utilising the pathological criteria as the gold standard. This lower sensitivity appears to be driven primarily by the high rate of Bartonella-associated BCNIE, coupled with a low prevalence of the clinical features incorporated into the minor criteria. Elevation of positive serology for Bartonella to a major criterion, similar to the previous modification of the criteria for Coxiella burnetii, will increase the sensitivity of the modified Duke/ESC 2015 clinical criteria in regions with a high prevalence of Bartonella-associated IE.
Limitations
Although Bartonella species are a frequent cause of BCNIE in the Western Cape region of South Africa and many other countries,12 13 30 the elevation of serology for Bartonella to a major criteria is unlikely to affect the sensitivity in countries with a low prevalence of this organism. The validity of this new criteria must be confirmed in different prospective cohorts of patients and should include the analysis of specificity and accuracy. We only performed serology for Bartonella species in patients with BCNIE and thus could not evaluate the specificity of the serological criteria utilised. Patients with known or newly diagnosed malignancy were excluded from this study.
Data availability statement
Data are available on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study was approved by the Health Research Ethics Committee of Stellenbosch University (Project number S19/08/162) and performed in accordance with the Declaration of Helsinki (2013 version). All patients signed written informed consent. Waiver of consent was approved for patients that demised before consent.
Acknowledgments
Dr E Ngarande, Research coordinator, Division of Cardiology, Department of Medicine, Stellenbosch University and Tygerberg Hospital, Cape Town, South Africa. Dr A Ismail, Division of Cardiology, Department of Medicine, Stellenbosch University and Tygerberg Hospital, Cape Town, South Africa. Dr D Zaharie, Department of Anatomical Pathology, Stellenbosch University and Tygerberg Hospital, Cape Town, South Africa.
References
Footnotes
Contributors All persons who meet authorship criteria are listed as authors, and all authors certify that they have participated sufficiently in the work to take public responsibility for the content, including participation in the concept, design, analysis, writing or revision of the manuscript. AJKP as the primary investigator and guarantor was responsible for the conception and design of the study, acquisition of data, analysis and interpretation as well as drafting of the manuscript. CP, PGH and AFD contributed to the conception and design of the study, acquisition of data, analysis and interpretation as well as revising the manuscript critically for important intellectual content. HP, JT and JJ contributed to the acquisition, analysis and interpretation of data as well as revising the manuscript critically for important intellectual content.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.