Article Text

Abstract
Objective To identify the most common transthoracic echocardiogram (TTE) parameters in patients hospitalised with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2/COVID-19) and their association with myocardial injury and outcomes.
Methods A retrospective, single-centre, observational, exploratory cohort study was performed at the height of the COVID-19 pandemic. All SARS-CoV-2 polymerase chain reaction (PCR) positive patients who underwent a TTE during their inpatient admission between 1 March 2020 and 31 October 2020 were analysed. The most frequent cardiovascular risk factor profile and echocardiographic features were investigated.
Results A total of 87 patients met the eligibility criteria. A salient 41.4% (n=36) of our cohort succumbed to this devastating virus. More than half of our hospital population (58.6%) were admitted to the intensive care unit (ITU) and this was significantly associated with inpatient mortality (OR: 7.14, CI 2.53 to 20.19, p<0.001). Hypertension was the most common cardiovascular risk factor (51.7%) with no additional prominence in non-survivors (OR: 2.33, CI 0.97 to 5.61, p=0.059). Remarkably, 90.8% of our cohort demonstrated a preserved left ventricular ejection fraction, although 69.1% had elevated troponin levels. Only 1 patient (1.1%) was given a diagnostic label of myocarditis. A raised pulmonary artery systolic pressure (36.8%) andright ventricle (RV) dysfunction (26.4%) were the most common echocardiographic features. In particular, the presence of RV dysfunction was significantly related to adverse outcomes (OR: 2.97, CI 1.11 to 7.94, p<0.03).
Conclusions In this cohort of extremely unwell patients hospitalised with COVID-19 pneumonitis, the presence of RV dysfunction or admission to ITU was significantly associated with inpatient case fatality ratio. Moreover, COVID-19-induced myocarditis remains extremely rare.
- COVID-19
- Echocardiography
- Hypertension
- Diagnostic Imaging
Data availability statement
Data are available upon reasonable request. All data pertinent to the study are presented in the research article.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known about this subject?
The SARS-CoV-2 pandemic presents one of the greatest medical challenges of our generation. While commonly causing a viral pneumonitis, it has significant and profound effects on the cardiovascular system. Myocardial damage in this cohort of patients is well recognised and is highlighted by the notable rise in troponin. However, the mechanism of myocardial injury remains convoluted.
What does this study add?
In this retrospective, observational survey, 69.1% of patients had elevated troponin levels but over 90% of patients had a preserved left ventricular function. Both elevated pulmonary artery systolic pressure (PASP) and right ventricle(RV) dysfunction were the most common echocardiographic features with RV dysfunction significantly associated with inpatient mortality. There was no significant relationship between inpatient death and prominent cardiovascular risk factors.
How might this impact on clinical practice?
Characterising the presence of RV dysfunction is a valuable tool in the risk stratification of patients hospitalised with COVID-19. Additionally, COVID-19-induced myocarditis is rare and troponin elevation is likely to represent the phenotype of a severe respiratory illness.
Introduction
The severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), otherwise known as the coronavirus (COVID-19) pandemic presents one of the greatest medical challenges of our generation. While commonly causing a viral pneumonitis, COVID-19 can trigger widespread and systematic insults largely precipitated through a cytokine storm.1 This can have profound and disastrous effects on the cardiovascular (CV) system.
Both the lungs and the heart express the angiotensin-converting enzyme 2 (ACE-2) protein, which has been acknowledged as the port of entry for SARS-CoV-2.1 With respect to the myocardium, cardiac myocytes and fibroblasts both express the ACE-2 receptor abundantly and studies have demonstrated that ACE-2 levels correlate with the extent of pathological left ventricular remodelling.1–3
Myocardial injury in COVID-19 is well recognised and is characterised by a significant elevation in troponin levels, especially in individuals with severe infection which necessitated hospitalisation.4 5 However, the exact mechanisms of this elevation remain uncertain. Yet, the value of this biochemical marker is critical in prognosticating patients infected with COVID-19, given the correlation between elevated levels and adverse outcomes.5–7 Although troponin is classically used to identify a type 1 myocardial infarction, multiple non-ischaemic processes such as hypoxaemia, venous thromboembolism, systemic inflammatory response, tachyarrhythmias and myocarditis contribute to this biochemical phenomenon in COVID-19.4–7
Transthoracic echocardiogram (TTE) has been widely utilised in patients hospitalised with COVID-19 to elucidate the aetiology of myocardial damage. Given its extensive availability, cost effectiveness and non-invasive approach, it is universally recommended as the first-line imaging modality to assess the structure and the function of the heart.8 9 However, due to the transmissibility and fatality rate of the SARS-CoV-2, leading societies only recommend the use of echocardiography if it is deemed to alter the management trajectory.10 As data regarding echocardiographic findings in COVID-19 remains sparse and inconclusive, we aim to add to the growing body of literature to identify the most frequent TTE parameters in patients hospitalised with COVID-19 and its association with myocardial injury and outcomes.
Methods
Study design
A retrospective review of all patients admitted with a COVID-19 polymerase chain reaction (PCR) positive swab who underwent a TTE between 1 March 2020 and 31 October 2020 at our institution was performed. All patients were greater than 18 years of age and only the index echocardiogram was included in the analyses. Patients with a previous echo indicative of heart failure with reduced ejection fraction were excluded. The study was conducted without any patient or public involvement.
Data collection
Pertinent demographic variables such as age, gender, ethnicity, height (cm) and weight (kg) were collected using the electronic healthcare records (Cerner, Missouri, USA). The presence of other diagnostic labels such as hypertension, diabetes, chronic obstructive pulmonary disease (COPD), chronic kidney disease (CKD), coronary artery disease (CAD), stroke and atrial fibrillation (AF) were also obtained. Peak high sensitivity troponin I (hs-cTnI) (ng/L) levels and the diagnosis of a new pulmonary embolus (PE) made during the inpatient admission was also noted. At our institution, hs-cTnI was considered elevated if it was ≥16 ng/L in females or >30 ng/L in males. Other variables such as admission to intensive care unit (ITU), the presence of a cardiovasular (CV) diagnosis on discharge and inpatient death were retrieved.
Echocardiogram
Scans were performed by British Society of Echocardiography (BSE) accredited sonographers in accordance with the BSE COVID-19 protocol.11 A level 1 BSE scan was performed in all patients with no ECG gating. Images were acquired by a GE Vivid Q ultrasound machine (GE Healthcare, Horten, Norway). At our institution, the GE EchoPAC PC V204 software was used to obtain measurements in accordance with the joint American Society of Echocardiography (ASE) and European Association of Cardiovascular Imaging (EACVI) guidelines .8 9
Echocardiographic variables such as left ventricular end diastolic dimension (LVIDd) (cm), left ventricular ejection fraction (LVEF) (%), left atrial size (cm), right atrial area (cm2), right ventricle (RV) size (cm), tricuspid annular plane systolic excursion (TAPSE) (cm) and pulmonary artery systolic pressure (PASP) (mm Hg) were collected. Left ventricular impairment was defined as an LVEF ≤50%. LVEF was calculated by the Simpson’s biplane method:
((End diastolic volume−end systolic volume)/end diastolic volume)×100.
In addition, the presence of left ventricular dilatation was determined by an LVIDd >5.2 cm in females and a LVIDd >5.8 cm in males. Furthermore, RV dysfunction was defined as either a dilated RV, reduced TAPSE or an impaired RV radial function either objectively or visually at the discretion of the echocardiographer. A dilated left atrium was identified either as an antero-posterior dimension of ≥4 cm; an indexed volume of ≥34 mL/m2 or a volume of ≥54 mL when BSA was not available for indexing. Right atrial dilatation was identified as an area ≥18 cm2. A TAPSE of <1.7 cm was defined as abnormal and a PASP of ≥35 mm Hg was suggestive of raised pulmonary artery pressures.
Statistical analyses
All the variables have been graphically inspected and summarise according to their statistical nature. This includes means, standard deviation, medians, interquartile values and ranges for continuous variables and proportions for categorical data with marginal percentages by hospital outcome. Logarithmic transform was considered where appropriate.
Exact logistic regression on a binary response defined by the hospital outcome to assess its associations with the available variables in the data was measured by odds ratio (OR). An OR greater than 1 indicates a harmful effect while an OR smaller than 1 indicates a protective effect. The level of significance was deemed as 0.05 and the uncertainties were expressed as 95% CIs. The relatively small dataset prevented a reliable multivariable model and the exploratory aspect of the analyses did not require adjustments for the alpha level of significance.
All analyses have been conducted in STATA (StataCorporation 2021, Stata Statistical Software: release 17, College Station, Texas, USA).
Results
During this 8-month period, a total of 90 patients with COVID-19 pneumonia underwent an echocardiogram. Out of these, 87 met the eligibility criteria (figure 1). Baseline characteristics, including demographics, comorbidities, biomarkers and relevant echocardiographic findings are illustrated in table 1. Majority of the referrals for echocardiography were primarily due to elevated troponin levels (n=53, 60.9%), followed by assessment of baseline left ventricular function (n=8, 9.2%). An abnormal ECG in isolation accounted for only one referral; however, an abnormal ECG together with a raised troponin level resulted in 7 (8%) echocardiograms being performed. Furthermore, a clinical suspicion of acute coronary syndrome (ACS) alongside an abnormal troponin led to 5 (5.7%) echocardiograms being completed.

Flowchart demonstrating the most pertinent features of our COVID-19 cohort. BAME, Black and minority ethnic; HFrEF, heart failure with reduced ejection fraction; LVEF, left ventricular ejection fraction; PASP, pulmonary artery systolic pressure; RV, right ventricle.
Baseline demographics, risk factors, biochemical and echocardiographic parameters
Patient characteristics
A salient 41.4% (n=36) of the study population succumbed to this devastating virus. The mean age of the cohort was 62±14.8 years of age and there was no significant difference observed between those who died and those who survived (64±13.7 vs 61.5±15.6, OR: 1.01, CI 0.98 to 1.04, p=0.43). Males comprised 55.2% (n=48) of the cohort. Our population demographics represents a high proportion of patients of black and minority ethnic origin (BAME) (60.9%, n=53). Notably, they were not at a higher risk of mortality from COVID-19 when compared with Caucasians (OR: 0.97, CI 0.37 to 2.50, p=0.95).
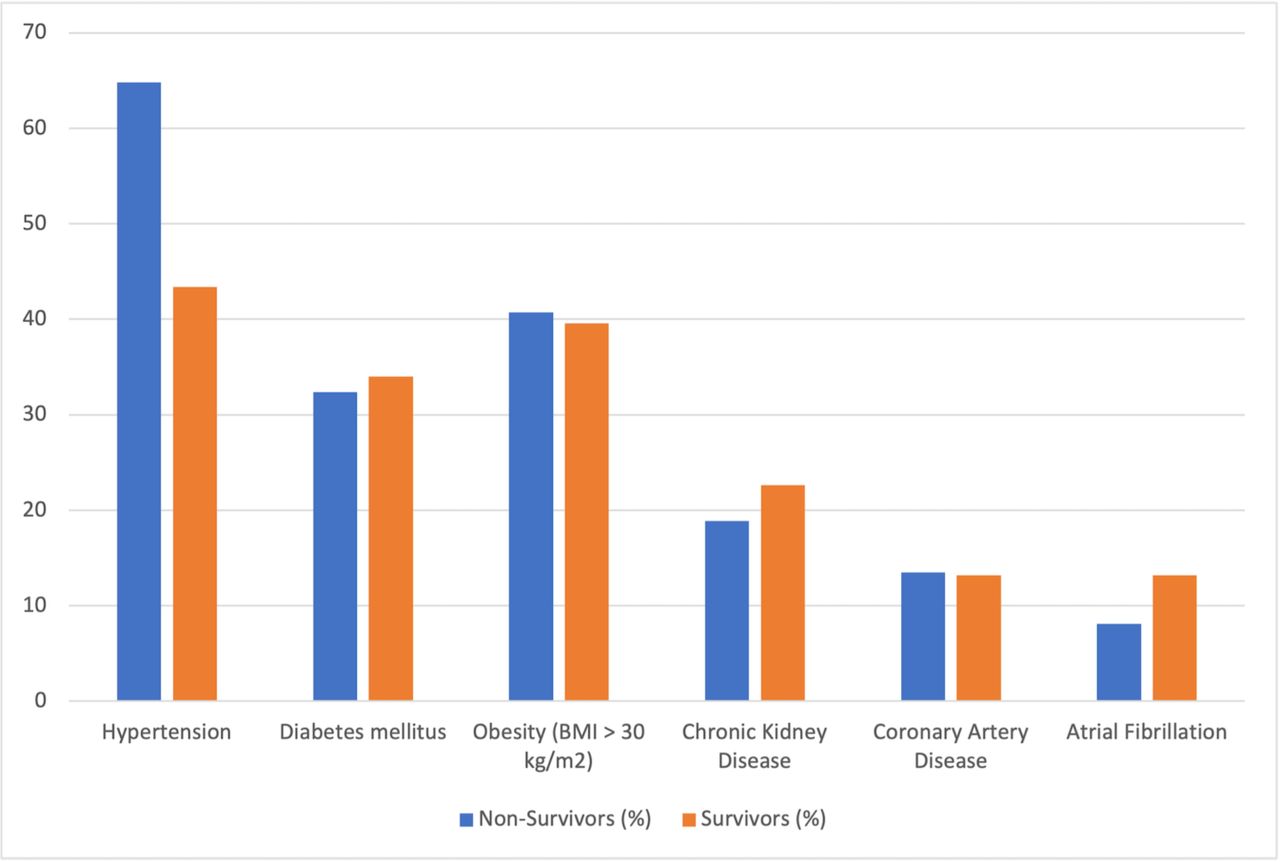
An overwhelming majority of the cohort were overweight with 65.5% (n=57) exhibiting a body mass index (BMI) of ≥25 kg/m2. The mean BMI of the cohort was elevated at 29.8±6.9 kg/m2, but there was no statistical significance demonstrated between obesity (BMI: >30 kg/m2) and inpatient mortality (OR: 1.14, CI 0.43 to 3.0, p<0.79). Other notable CV risk factors included hypertension (51.7%) and diabetes (33.3%) (figure 2). There was no significant link observed between the presence of CV risk factors and inpatient death, although a diagnostic label of hypertension was close to achieving statistical significance (OR: 2.33, CI 0.97 to 5.61, p=0.059). More than half of the cohort (58.6%) was admitted to ITU and out of the 36 patients who died, 30 (83.3%) passed away in the ITU setting. Intuitively, admission to ITU was associated with an increased risk in mortality (OR: 7.14, CI 2.53 to 20.19, p<0.001).
{kind=link}
{kind=link}
Bar chart demonstrating the distribution of comorbdities in both survivors and non-survivors. BMI, body mass index.
Transthoracic echocardiogram
Overall, 90.8% (n=79) of the cohort had a preserved LVEF. The mean LVEF of our population was 60.7%±10% and there were no significant differences between survivors and non-survivors (59.8% vs 62.1%, p=0.30). Markedly, 91.7% (n=33) of the non-survivors cohort had a preserved LVEF. A raised PASP (36.8%) was the most common echocardiographic feature exemplified in our cohort, although this was not related to mortality (OR: 1.84, CI 0.56 to 6.05, p<0.32). Numerically, the mean PASP was considerably higher in those who died (44.5±14.2) when compared with those who survived (38.5±11.1). Importantly, RV dysfunction was demonstrated in 26.4% of patients and this was associated with a 3-fold increase in death (OR: 2.97, CI 1.11 to 7.94, p<0.03). Both the left (22.2%, n=18) and right (21.3%, n=16) atria were dilated in less than a quarter of patients with no relation to fatality (p=0.08 and p=0.36, respectively). With regards to LV remodelling, the mean LV size was significantly higher in those who survived (4.6±0.5 cm vs 4.2±0.7 cm). Nonetheless, it is critical to recognise that the mean LV size for both subgroups was well within normal limits with only 4.9% (n=4) of the overall cohort having a dilated LV.
Eighteen (20.7%) patients subsequently underwent a repeat TTE during their inpatient admission. Sixteen (88.8%) out of the 18 repeat TTE’s were performed in ITU patients. From the 13 patients with a raised PASP on the initial echocardiogram (all ITU patients), 7 (53.8%) improved their right-sided pressures with 4 (30.8%) normalising their pulmonary artery pressures. Yet, 7 (53.8%) individuals still had persistently elevated PASP on repeat imaging. Only one out of the four patients with normalised PASP eventually expired. However, 85.7% (n=6) of the patients with persistently raised PASPs died.
Troponin
Troponin levels were performed in 81 (93.1%) patients. Elevated levels were observed in 69.1% (n=56) of our cohort with raised levels occurring more frequently in women (71.8%) compared with men (58.3%). The median peak troponin was numerically higher in the patients who died when rivalled to those who survived (71.2 ng/L vs 45.3 ng/L, OR: 1.14, 95% CI 0.88 to 1.47, p<0.32).
CV outcomes
Fifteen patients (18.4%) had a concomitant CV diagnosis during their admission with 8 (9.2%) patients diagnosed with AF or a supraventricular tachycardia. Five patients (5.7%) were diagnosed with a Non-ST elevation myocardial infarction (NSTEMI). However, it is important to note that out of these patients, only one underwent coronary angiography and subsequent percutaneous coronary intervention. Two patients were admitted to ITU for concomitant severe COVID-19 pneumonitis and were too unstable to undergo coronary angiography and were treated medically. Moreover, one patient had a poor functional status and his frailty precluded him from undergoing coronary angiography. The remaining one patient was planned to undergo an outpatient CT coronary angiogram. Additionally, 1 patient (1.1%) was given a diagnostic label of myocarditis after a coronary angiogram revealed a non-ischaemic cause of chest pain and troponin rise. Finally, one patient was newly diagnosed with LV non-compaction cardiomyopathy.
Discussion
Our study represents an extremely sick cohort of patients with an ITU admission rate of 58.6% and an inpatient mortality rate of 41.4% at a busy East London district general hospital. Remarkably, over 90% of the cohort demonstrated a preserved LVEF. Both a raised PASP and RV dysfunction were markedly prevalent with RV dysfunction in particular exhibiting a significant link with inpatient mortality. This corroborates with data from Europe and the USA.12–15 In particular, Wats et al established that poorer the RV function, the higher the risk of death from COVID-19.13 Furthermore, sequalae of RV dysfunction such as tricuspid regurgitation (TR), specifically moderate to severe TR, also displayed an increased association with adverse outcomes. Studies have also demonstrated a relationship between elevated PASP and an increased risk in mortality; however, we did not ascertain a correlation between these two variables.12 13 It is perceptive that both RV dysfunction and raised PASP are likely to represent a phenotype of the severe respiratory illness from COVID-19 pneumonitis rather than direct, isolated RV damage from the virus. As such, our dataset demonstrated that 53.8% (n=7) of the ITU cohort with raised PASPs who underwent serial echocardiography improved their pulmonary pressures likely as a result of the superior ventilation provided by mechanical respiratory support. This once again offers evidence for the role of respiratory pathology as the main contributor to the elevated right heart pressures and dysfunction in COVID-19. In fact, a literature review of cardiac autopsies from patients with COVID-19 revealed myocarditis in only 20 out of 277 (7.2%) patients.16 Moreover, this was likely to be an overestimate given the lack of standardisation and rigour in recognising myocarditis in postmortem studies. From a CV point of view, this is reassuring and recent cardiac MRI analysis of 149 healthcare workers with mild COVID-19 infection demonstrated a late gadolinium enhancement pattern consistent with myocarditis in only 4% of individuals after 6 months from the initial incubation.17 Our echocardiographic data reiterates these findings with only 1.1% of our cohort having a diagnostic label of myocarditis. While COVID-19 primarily insults the lung parenchyma through direct invasion via the ACE-2 receptors, PE has also been widely reported as a consequence of the systemic and vascular inflammation.1 18 A combination of both viral pneumonitis and thrombosis of the pulmonary arteries is postulated to play a critical role in the development of RV dysfunction.
In a subset of patients who underwent repeat echocardiography, there was a signal towards the utility of PASP as a prognostic marker, as those with persistently raised pulmonary pressures were more likely to succumb to SARS-CoV-2. In line with this, retrospective observational data from New York, USA (n=214), identified the important association between elevated pulmonary pressures and death in the hospital population (OR: 5.39, CI 1.96 to 14.86, p<0.001).13 Additionally, elevated PASP was also linked to a need for vasopressor support and mechanical ventilation, which is instinctive given that elevated right-sided pressures are a direct result of severe COVID-19 pneumonitis and/or PE.13 Furthermore, a raised PASP with simultaneous reduction in TAPSE (TAPSE/PASP ratio) has also been demonstrated to be an independent marker of poor outcomes in COVID-19 Acute Respiratory Distress Syndrome and adds additional value to the traditionally used Berlin Criteria in prognostication.19 However, given the variability in accurately measuring PASP through echocardiography and particularly in patients on respiratory support, this will need to be studied in a prospective, rigorous and standardised manner before being used for prognostication purposes in patients with COVID-19.
Cardiac troponin was notably elevated in the majority of our study population (69.1%). However, this elevation was not characterised by an increase in mortality in contrast to contemporary data.4 5 20 When rivalled to other biomarkers, troponin has been shown to be superior for prognostication purposes. Zhou et al elucidated that in 191 hospitalised patients with COVID-19, troponin I had an OR of 80.1 (CI 10.34 to 620.36, p<0.0001) in predicting mortality, a figure significantly more prominent when compared with D-Dimer, lactate dehydrogenase, creatine kinase and white cell count. Although troponin I elevation is classically interconnected with ACS, case series have shown that in those infected with COVID-19 who present with ST segment elevation on ECG, a substantial percentage have unobstructed coronary arteries.21 22 In addition, postmortem analyses have also highlighted the infrequency of acute myocardial infarctions in the COVID-19 cohort.16 Therefore, the mechanisms of troponin leak in these patients remain multifactorial and predominantly non-ischaemic. These include indirect myocardial injury secondary to severe hypoxia, sepsis, systemic inflammation, PE and rarely from direct myocardial injury from stress cardiomyopathy or myocarditis. Another proposed mechanism for this phenomenon can be related to the degree of RV dysfunction and our data underscores this association with 78.2% of patients with RV dysfunction expressing elevated troponin levels. Out of the 7 patients with troponin values >900 ng/L, 5 (71.4%) conveyed RV dysfunction on their echocardiogram.
We did not establish a significant relationship between the presence of hypertension and inpatient mortality. However, this was perishingly close to statistical significance and the overwhelming majority of current literature provide striking evidence for this connection.5 6 23 24 Furthermore, this link was echoed during the Middle East respiratory syndrome coronavirus (MERS-CoV) outbreak in 2012, which shares analogous pathogenesis to SARS-CoV-2.25 26 The co-existence of hypertension along with other CV risk factors such as diabetes, CKD and CAD predisposed patients to MERS-CoV as well as considerably increasing their risk of death. Data from Wuhan, the epicentre of SARS-CoV-2, additionally demonstrated a preponderance of COVID-19 to individuals with underlying hypertension and its significant relation to mortality (OR: 3.05, CI 1.57 to 5.92, p<0.0010).6 Intriguingly, a meta-analysis of 48 317 patients infected with COVID-19 exhibited that younger patients (<50 years) with hypertension had a higher fatality rate than older patients (>60 years) with the same comorbidity.23 In addition, numerous studies have also shown diabetes, obesity and underlying coronary artery disease to also be a poor prognostic sign.27 However, we were again unable to reverberate these findings. Overall, the reason for increased prevalence of hypertension in the COVID-19 cohort remain unclear and convoluted. A plausible explanation is that hypertension predisposes COVID-19 individuals to myocardial injury, which perpetuates poorer blood pressure control and thus leading to adverse outcomes.28 29 The initial theories suggesting the role of upregulation of ACE-2 receptors in those with underlying hypertension have been widely disproved.24 28 In the non-COVID-19 cohort, plasma ACE-2 levels have shown to be notably elevated as well as associated with adverse outcomes in those with AF, obstructive CAD and aortic stenosis.2 3 30 Recent COVID-19 literature have similarly demonstrated prominent levels of plasma ACE-2 in those infected with SARS-CoV-2 in addition to being a prognostic compass.30 Therefore, this novel biomarker is an exciting area which requires more detailed characterisation to fully recognise its value in improving outcomes from this destructive virus.
Limitations
Numerous limitations exist within our study. First, as a retrospective, observational study there is an inherent selection bias and inability to control confounding variables. Second, only patients who the parent team viewed as appropriate for an echocardiogram were examined and hence there was a large cohort of patients hospitalised with COVID-19 we did not capture. In addition, only patients with a positive PCR result were included and there is probably a proportion of patients with false negative PCR results who were not studied. Furthermore, our data are only applicable to the hospital population and does not apply to the large majority of patients with mild COVID-19 infection. In accordance with the BSE COVID-19 protocol, level 1 scans were performed, and thus valvular pathology was not expertly analysed. Finally, death from an alternative aetiology other than COVID-19 cannot be fully excluded but given that the hospital admissions during our study period were virtually all COVID-19 presentations, it is extremely likely that all inpatient mortality was directly attributable to SARS-CoV-2.
Conclusions
Our single-centre, retrospective cohort study exhibits a critical contribution to the COVID-19 literature. Remarkably, in this extremely ill cohort of patients who died, over 90% of patients had a preserved LVEF. Moreover, admission to ITU or echocardiographic evidence of RV dysfunction in the hospitalised COVID-19 population signifies a trend toward poorer outcomes, thus, indicating that the echocardiographic phenotype associated with adverse events is more consistent with a severe respiratory illness rather than direct myocardial injury from SARS-CoV-2.
Data availability statement
Data are available upon reasonable request. All data pertinent to the study are presented in the research article.
Ethics statements
Patient consent for publication
Ethics approval
Ethical approval was granted by the Health Research Authority and Health and Care Research Wales. The integrated research application system identification number is 286 146.
Acknowledgments
We are extremely grateful to the cardiac physiology department at Homerton University Hospital for performing high-quality echocardiograms in challenging situations.
References
Footnotes
Contributors The corresponding author, AB, attests that all listed authors meet authorship criteria and that no others meeting the criteria have been omitted, and is the recognised guarantor for this piece of original research. All authors (AB, ZM, NE, DL, JN, RB, ICS, JB and VV) contributed to the proposal of the research project, data analysis and interpretation as well as the writing and revision of the manuscript. Statistical analyses were performed by ICS.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.