Article Text

Statistics from Altmetric.com
Transcatheter aortic valve replacement (TAVR) was born as a last resort for otherwise inoperable patients with symptomatic severe aortic stenosis (AS).1 Initially, the procedure was invasive, associated with serious complications and expensive, but if successful, offered patients with few treatment options the opportunity for improved survival and enhanced quality of life (QoL). Among elderly TAVR candidates, improvement in functional class is often the more relevant benefit of a successful TAVR while younger patients may be more concerned with the longer survival associated with the procedure.
A poor outcome after a specific intervention can be defined as the intervention failing to achieve the expected treatment goals. With TAVR, the treatment goals are improved survival and reduced symptoms and hence, a poor outcome would include death and reduced QoL post procedure.2 The cornerstone randomised controlled trials of TAVR carefully evaluated objective QoL measures prior to and after TAVR using the Kansas City Cardiomyopathy Questionnaire (KCCQ), a standard measure of symptoms, physical and social limitations, and QoL in patients with heart failure. In the Placement of Aortic Transcatheter Valve (PARTNER) 1 Trial—Cohort B, compared with medical therapy alone, TAVR conferred a 25-point improvement (five points usually considered clinically relevant) in the KCCQ overall summary (KCCQ-OS) Score still lasting after 1 year.3 Similarly, in high-risk operable patients (PARTNER Cohort A and CoreValve US Pivotal Trial), TAVR was associated with a highly significant and clinically meaningful improvement in the KCCQ-OS Score (increase of 20–30 points) at 1 month, 6 months and 1 year compared with the baseline,4 5 with a more rapid improvement in TAVR arm compared with surgery (1-month scores greater after TAVR). Interestingly, the lower the estimated surgical risk the greater the improvement in QoL: in low-risk patients (PARTNER 3 trial), TAVR was associated not only with KCCQ-OS Score increase compared with baseline (19 points at 1 year) but also with greater improvement compared with surgery beyond 1 month: 6 months (p=0.04) and 12 months (p=0.04).6 7
The reported improvement in QoL among the major TAVR trials obviously represents the average treatment effect among the treated patients. With any medical intervention, the magnitude of benefit varies from patient to patient and can be impacted by a number of patient-specific and treatment-specific variables. This is especially true when the population in question present numerous comorbid illnesses, as with TAVR recipients. Both cardiac and extra-cardiac conditions can impact outcome after TAVR. It is therefore not surprising that in among the elderly and frail TAVR patients included in the PARTNER 1 trial, more than one-third (35%) of TAVR recipients had a poor outcome at 6 months (death or a KCCQ-OS Score<45 (equivalent to New York Heart Association (NYHA) Class IV)).2 Observational data of real world clinical practice support the randomised trial observation of a substantial proportion of patients failing to achieve treatment goals after TAVR: among more than 13 000 patients included in the US Society of Thoracic Surgeons/American College of Cardiology/Transcatheter Valve Therapy (STS/ACC/TVT) Registry with STS scores well distributed among risk classes (47% high risk; 39% medium risk; 14% low risk, mean STS Score 7.7%), 39% of patients presented poor outcomes at 1 year (death, or 10-point decline in KCCQ-OS or KCCQ-OS<60 (equivalent to NYHA III–IV)).8 Poor QoL accounted for half of these substandard clinical outcomes.
It is therefore imperative to identify TAVR candidates with an expected poor functional outcome and to integrate this information into clinical decision-making. To date, several studies have identified predictors of poor outcomes, defined as death or absence of QoL improvement, but few have focused only on the patient’s symptomatic status. Symptom status alone is highly relevant for elderly patients with poor QoL and is a key component of patient-reported outcomes. Yoshijima et al9 report important information on the role of specific baseline characteristics in anticipating poor symptomatic improvement (SI) after TAVR and how poor SI impacts prognosis.
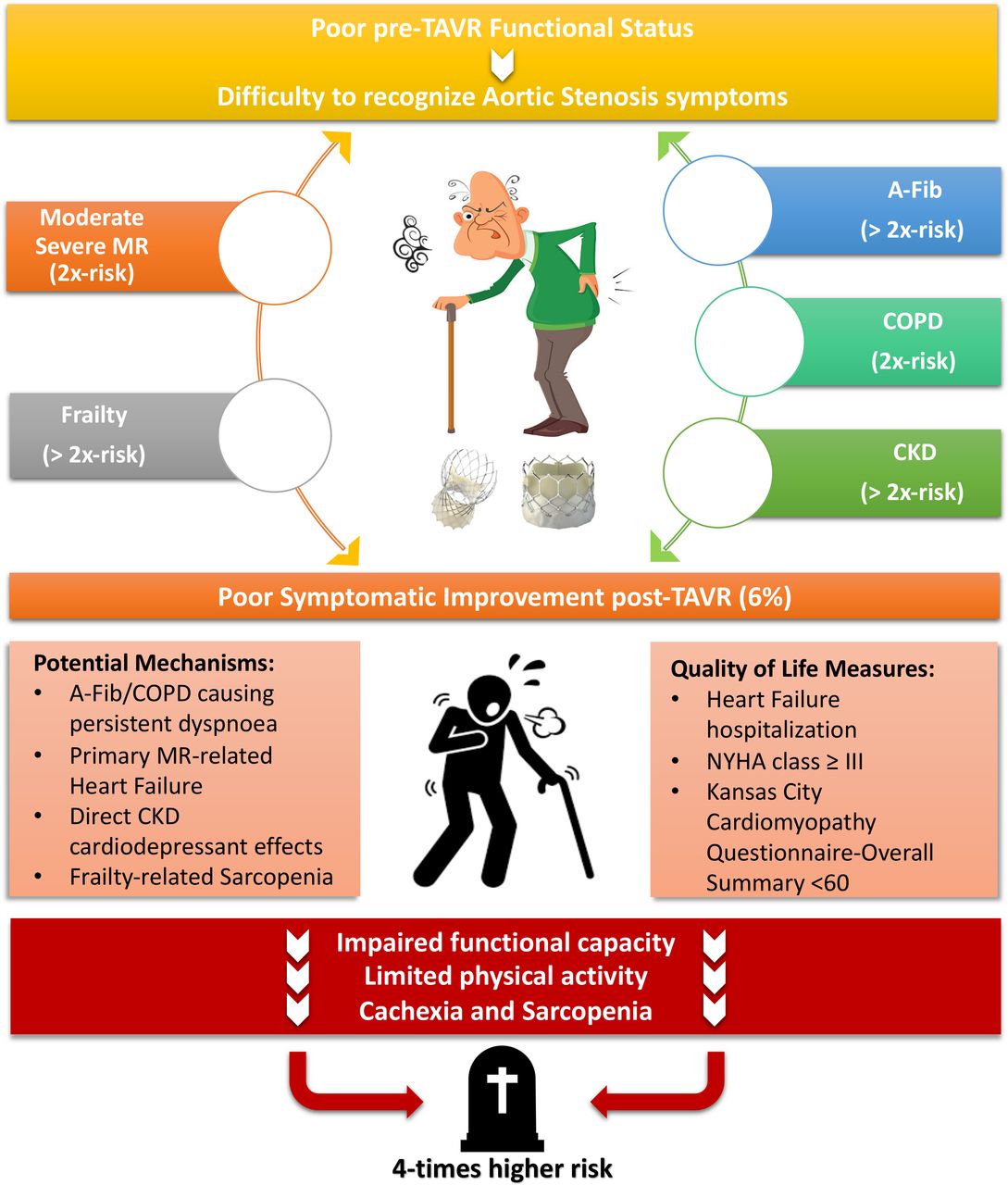
Poor SI was defined as readmission for heart failure or NYHA≥3 at 1 year after TAVR. The choice of NYHA class instead of QoL scores can be justified as it represents both the exercise capacity and symptomatic status of the patient. Poor SI was reported in 6.6% of the study population (1749 patients; mean STS Predicted Risk of Mortality (PROM) Score 6.3%) and was associated with baseline atrial fibrillation (AF) (HR 2.20, 95% CI 1.44 to 3.36, p<0.001), chronic obstructive pulmonary disease (COPD) (HR 1.68, 95% CI 1.01 to 2.78, p=0.045), Clinical Frailty Scale≥4 (HR 2.17, 95% CI 1.36 to 3.43, p=0.001), chronic kidney disease (CKD) (HR 2.30, 95% CI 1.28 to 4.14, p=0.005) and preprocedural moderate-to-severe mitral regurgitation (MR) (HR 1.90, 95% CI 1.14 to 3.15, p=0.013).
The prevalence of poor SI in this series (6.6%) is low when compared with previous data. In the PARTNER 1A trial, poor SI based on KCCQ-OS Score alone amounted to one in five patients (20%); in the STS/ACC/TVT registry it was 18.2% of cases. The reported low incidence of poor SI may be related to several factors: the use of NYHA class as a QoL parameter may reflect the physician’s subjective perspective than that of the patient and could underestimate the patient’s perception.10 Also, the exclusion patients who died within 1 year of TAVR from this analysis likely impacted the low rate of poor SI. Moreover, the inclusion of first-generation TAVR systems and the analysis being limited to Asian patients could limit the generalisation of such finding to broader populations.
The current study also identifies predictors of poor SI that are almost identical to predictors of adverse clinical outcome (death/impaired QoL) reported in prior analyses. Indeed, it is hardly surprising that AF, COPD and CKD (per creatine increase 1 mg/dL) have been associated with limited improvement in 6-minute walking test and in KCCQ-OS after TAVR.11 12 AF, COPD and pulmonary hypertension often present dyspnoea which, on one hand, can confound the symptomatic assessment of AS prior to TAVR, and on the other hand, can impair the functional capacity of patients after TAVR. Patients with these comorbid conditions often limit their activity to avoid experiencing uncomfortable symptoms and hence, symptom improvement after TAVR is less likely, irrespective of the outcome of the procedure and associated the impact on cardiac function.13 14 Similarly, among patients with CKD, an overactive renin–angiotensin–aldosterone axis can exacerbate adverse haemodynamic status and be directly cardiodepressant.15
The association of baseline moderate-severe MR with poor SI is a novel, but rational, finding. The aetiology of the MR was not reported in this study, however, and is a key issue when considering the outcome of patients with coexistent MR undergoing TAVR since the severity of MR has been shown to improve in two-thirds of patients (60%) of cases, mostly attributed to reverse left ventricular remodelling and improved left ventricular function,16 suggesting functional MR aetiology in these patients. In contrast, structural mitral valve disease (primary MR) is likely to persist after TAVR and could explain the absence of symptom improvement. It is therefore imperative to evaluate the cause of MR before considering its ability to predict future events.
The current study also adds to the available literature supporting the association of frailty with poor SI after TAVR. Despite the considerable body of evidence on this issue,17 18 objective measures of frailty are unfortunately often overlooked in the work-up for TAVR and have also been omitted from prior analyses used to develop QoL prediction models.8 Not surprisingly, patients with poor SI also had a higher incidence of all-cause death and readmission for HF (p<0.001), likely reflecting the increased burden of comorbid illnesses. The inevitable sarcopenia and cachexia that ensue from limited physical activity and advanced frailty have previously been associated with a four-time increased risk of death (figure 1).19 20
{kind=link}
Graphic explanation of the complex relationship between medical comorbid illnesses and severe aortic stenosis and their impact on a patient’s symptoms, before and after TAVR. A-Fib, atrial fibrillation; CKD, chronic kidney disease; COPD, chronic obstructive pulmonary disease; MR, mitral regurgitation; NYHA, New York Heart Association; TAVR, transcatheter aortic valve replacement.
The present study reminds us that a considerable proportion of TAVR patients do not derive a symptomatic benefit from TAVR. This underscores the importance of assessing all TAVR candidates for the known predictors of poor outcome and to document objective measures of frailty. These data inform the shared-decision-making process with patients and their families and provide an opportunity to avoid complex, expensive and ultimately futile procedures.
Ethics statements
Patient consent for publication
Ethics approval
This study does not involve human participants.
References
Footnotes
Contributors ML and DM drafted and revised the final manuscript. CK and AP did literature revision.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests DM: Consultant for Medtronic, Boston Scientific and Microport.
Provenance and peer review Commissioned; internally peer reviewed.