Article Text

Abstract
Objectives Diastolic dysfunction (DD) has been reported to be highly prevalent in people living with HIV (PLWH) on antiretroviral therapy (ART) leading to the hypothesis that it may be an early marker of myocardial disease. Our objective was to evaluate the prevalence of DD in people living with human immunodeficiency virus without known history of diabetes or hypertension in Western Kenya.
Methods In this cross-sectional study in western Kenya, 110 PLWH on ART and without known diabetes or hypertension were matched for age ±5 years and sex to HIV-uninfected controls. Study participants underwent a comprehensive two-dimensional echocardiogram and laboratory testing.
Results The mean (SD) age in the HIV-positive group was 42.9 (8.6) years compared with 42.1 (12.9) years in the HIV-uninfected group. Mean (SD) CD4 +T cell count for the HIV-positive group was 557 (220) cells/ml. Mean systolic and diastolic blood pressures were within the normal range and comparable between the two groups. Mean body mass index was 25.2 (5.4) kg/m2 and 26.3 (5.4) kg/m2 in HIV-positive and uninfected participants, respectively. There was only 1 (0.9 %) case of DD in each group. Despite low prevalence of DD, PLWH had 5.76 g/m2 higher left ventricular mass index (p=0.01) and 2.77 mL/m2 larger left atrial volume (p=0.02) compared with the HIV-negative group after adjusting for risk factors associated with DD.
Conclusion Contrary to prior reports, DD in PLWH was low. Environmental and cardiovascular disease risk factors such as diabetes and hypertension may be significant modifiers for development and progression of DD in PLWH.
- echocardiography
- epidemiology
- global health
Data availability statement
Data are available on reasonable request. The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known about this subject?
People living with HIV (PLWH) are at increased risk of heart failure.
Diastolic dysfunction has been reported to be highly prevalent in PLWH and proposed that it may be an early marker of heart failure in PLWH.
What does this study add?
Contrary to prior reports, in this contemporary population of PLWH on antiretroviral therapy in Western Kenya without history of hypertension and diabetes, the prevalence of diastolic dysfunction was very low.
However, after multivariable adjustments including age, sex, body mass index and systolic blood pressure, PLWH had increased left ventricular mass and left atrial size.
How might this impact on clinical practice?
Additional studies are needed to elucidate the environmental and cardiovascular risk factors that may predispose PLWH to myocardial structural changes and increased risk for heart failure.
Introduction
The advent of antiretroviral therapy (ART) has changed the course of HIV from an acute infection with high mortality to a chronic disease with many ageing-associated comorbidities.1 As the successes of ART coverage expands and people living with HIV (PLWH) are living well past the age of 50,2 cardiovascular diseases are now the leading cause of morbidity and mortality in this population.3 4
Cardiac involvement in HIV infection has long been described with an AIDS defining phenotype of dilated left ventricular (LV) systolic dysfunction in the pre-ART era.5 Despite optimal ART however, PLWH remain at a significantly increased risk of heart failure even after adjusting for the prevalent traditional cardiovascular risk factors.6 There are very limited data on the natural history of heart failure in the current era of ART and the mechanism for this increased risk is not fully understood.7
Despite the disproportionate burden of the HIV epidemic concentrated in sub-Saharan Africa, accounting for more than 70% of PLWH,8 there is paucity of data from this region on cardiovascular disease burden and prevalence of heart failure in PLWH in the ART era.7 9 In the South African Heart of Soweto Study,10 9.7% of newly diagnosed heart disease patients were HIV-infected with 29% with LV systolic dysfunction and 38% with HIV-associated cardiomyopathy. On the other hand, in a multicentre study of patients presenting with acute heart failure in nine African countries, only 2.6% of heart failure were attributed to HIV cardiomyopathy.11
It has been well-established diastolic dysfunction (DD)12–14 is highly prevalent in PLWH without symptoms of heart failure, leading to the hypothesis that it may be an early marker of myocardial dysfunction in this population.15 Studies in the USA have also shed light on the unique mechanisms and consequences of DD in PLWH, highlighting fibrosis and left atrial abnormalities that are associated with risk of clinical heart failure.16 17 Given the link between DD and its association with overall increased mortality and heart failure with preserved ejection fraction,18 19 more studies are needed to effectively characterise the epidemiology of DD in PLWH in endemic regions.
Prior studies linking HIV to DD have focused on PLWH with greater burden of comorbid conditions12 such as diabetes and hypertension,12 13 20 21 hepatitis C infection13 22 23 that confound the true association of DD with HIV infection. Similarly, the limited studies from Africa evaluating asymptomatic PLWH have included untreated cohorts24 25 or PLWH with high prevalence of cardiac comorbidities20 24 strongly associated with DD. The objective of this study was to characterise the prevalence of DD in ART treated PLWH in Kenya and a matched HIV-uninfected (HIVneg) group, without known risk factors of diabetes and hypertension.
Methods
Study setting
The study was a cross-sectional study; participants were recruited from the Moi Teaching and Referral Hospital (MTRH) in Eldoret, Kenya, within the Academic Model Providing Access to Healthcare (AMPATH) programme. The AMPATH programme is a partnership between Moi University School of Medicine, Moi Teaching and Referral Hospital (Kenya’s second national referral hospital), and a consortium of US medical schools that promotes a comprehensive approach to providing care in Western Kenya.26 The Moi Teaching and Referral Hospital is an 800-bed capacity, university affiliated hospital, serving a broad mix of rural, urban poor and urban middle-class population in Western Kenya. The AMPATH Centre at MTRH serves over 50 000 patients with HIV.
Power analysis estimates
To estimate the required sample size, we reviewed the literature on the prevalence of DD in PLWH and non-infected individuals.12 13 27–31 Major findings were that in PLWH, the prevalence of DD was 26%–67%.29 Most of these studies included individuals 30–50 years of age, and 4%–30% had either diabetes or hypertension.13 32 33 Notably Schuster31 et al study in PLWH, age 42.1±4.7 years without metabolic syndrome and hypertension had reported prevalence of DD of 67%, and when restricted to abnormal transmitral flow, DD was present in 27% compared with 12% in matched healthy controls. DD prevalence in large unselected population studies ranged from 11% to 27%34 35 with age ranges between 25 and 75 years. In the younger age groups of 25–45 years, DD was estimated at 2.834–8.835%.
Using lower DD prevalence to account for absence of comorbidities in PLWH and overestimating prevalence in the HIV uninfected controls, we performed a power calculation assuming the prevalence of DD of 14% in PLWH and 3% in HIV-uninfected. An estimated 100 participants in each group to obtain statistical power at 0.80 level at the 0.05 alpha level.31 To eliminate the effect of potential dropouts and increase further the power of the study, 110 individuals per group were recruited.
Study participants
Adult men and women living with HIV and treated with long-term ART (>1 year) were recruited from a convenience sample of an existing cohort of 300 PLWH actively enrolled into care in the AMPATH clinic centre.
Participants were contacted by phone and invited to participate in the study. Interested participants completed a structured questionnaire, physical exam, venous blood sampling, echocardiography and ECG after their routine clinic appointment. PLWH were matched to HIVneg participants based on age (±5 years) and sex. Inclusion criteria were age 18 years or older treated with ART for at least a year. Pregnant women, patients who reported prior diagnosis of hypertension or diabetes or were on medications for high blood pressure or diabetes were ineligible to participate. HIVneg participants were recruited from different outpatient clinic centres within MTRH where they were either voluntarily seeking HIV testing or were referred by providers for testing. Participants who matched for age and sex to the PLWH cohort and tested negative for HIV were approached to participate in the study. Exclusion criteria for controls were identical to those described for cases, with the additional criterion that controls had tested negative for HIV. All study participants signed a written informed consent and were enrolled between February 2016 to May 2016.
Patient and public involvement
This research was done without patients and public involvement. Patients were not invited to comment on the study design and were not consulted to develop patient relevant outcomes or interpret the results. Patients were not invited to writing or editing this manuscript for readability or accuracy.
Clinical assessment
Clinical history for PLWH was obtained from review of both electronic medical records and paper-based charts. All participants completed a questionnaire including personal and family medical history, socioeconomic status indicators, smoking and alcohol intake, physical activity level and basic nutritional survey. Blood samples were collected for non-fasting lipid panel, glycosylated haemoglobin A1C level, in addition to CD4 +T cell count levels in PLWH. Viral loads were obtained from review of the electronic medical records and were included in the analysis if they were performed within a year from the participant enrolment date in the study. All participants had their weight, height, waist and hip circumference measured in addition to heart rate and blood pressure measurements after at least 5 min of rest.
Echocardiogram
All participants underwent comprehensive echocardiograms performed by a single experienced sonographer with a Philips CX50 (Philips Healthcare, Boethel, Washington, USA). We used two-dimensional (2D), colour Doppler, tissue Doppler and spectral Doppler imaging using a standardised protocol of image acquisition for chamber sizes, LV size and systolic and diastolic function according to the American Society of Echocardiography (ASE) guidelines.36 Echocardiogram images were securely stored and transferred to the Duke Cardiac Diagnostic Unit core laboratory. Echocardiogram measurement and interpretation followed a protocol developed specifically for this study with two primary readers (BW and BC) and one over-reader (GSB). All LV structure and function-related measurements were averaged from three separate measurements of 2–3 different cardiac cycles. The LV mass was determined by aligned linear measurements of LV cavity dimension and wall thickness from the 2D parasternal long axis view and was calculated using the Devereux standard validated formula.36 Left atrial (LA) volume was derived using the apical four-chamber and two-chamber views.36 LV mass index (LVMI), left atrial volume index (LAVI) were calculated and indexed to body surface area. Biplane measurements were used to calculate EF and were compared with visual EF assessment. Abnormal LV systolic function was defined as biplane EF less than 50%, or visual EF less than 50% when biplane measurements were not available. Tricuspid regurgitant systolic jet velocity (TRV) was measured in the apical four-chamber view. TRV was assumed to be normal in subjects who had no tricuspid regurgitant jet or a weak unmeasurable peak TRV. RAP is the estimated right atrial pressure based on calibre and respirophasic variation of the inferior vena cava. Diastolic parameters and function were assessed using the 2016 ASE guidelines37 with the following criteria for assessing components of DD: average E/e′ ratio >14, septal é velocity <7 cm/s or lateral velocity <10 cm/s, tricuspid regurgitation velocity >2.8 m/s, and LA volume index >34 mL/m2. Forty-six (42%) participants in each group had unmeasurable TRV that were assumed to be normal. E/e′ ratio was missing in five participants (2.3%), LAVI in two per each group (1.8%) and average e’ was missing in 1.
Data analysis
All data are expressed as mean±SD or median (range) for continuous variables and percentages for discrete variables, stratified by HIV status. Continuous variables were analysed by Wilcoxon signed rank test and categorical variables by Fisher exact or χ2 as appropriate to compare covariates between those with and those without HIV infection. A significance level was set at p<0.05, and all probability values reported were two sided.
The effect sizes of HIV status on diastolic function parameters, LVMI and LAVI were assessed using unadjusted and adjusted linear and logistic regression models. Covariates in adjusted models included age, sex, systolic blood pressure, glycated haemoglobin A1C, smoking history (never/ever) and body mass index (BMI). Additional individual multivariable linear regression models were fitted in the PLWH with HIV immune parameters (nadir CD4 +T cell count, recent CD4 +T cell count and detectable viral load (HIV RNA >20 copies/mL), years since HIV diagnosis) after adjusting for other covariates. Interaction effects between HIV status and sex were also analysed in additional adjusted models. Analysis was performed using Statasoftware (StataCorp. 2015. Stata Statistical Software: Release 14.2: StataCorp).
Results
Baseline subject characteristics
We screened 188 PLWH and 146 HIVneg individuals and enrolled 110 participants in each group (figure 1). Participants’ characteristics are described in table 1. The mean age of the cohort was 42.9±9 years in PLWH and 42.1±13 in HIVneg and about 60% were female. The mean systolic blood pressure was comparable between the two groups and in the normal range. BMI was slightly higher in HIVneg but the difference was not statistically significant. The prevalence of smoking history (current or prior history) was higher in PLWH compared with HIVneg (20% vs 6.4%, p=0.003). PLWH had higher serum total and high-density lipoproteins (HDL) cholesterol compared with the HIVneg group, whereas triglycerides and calculated low-density lipoproteins (LDL) -cholesterol were similar between the two groups. Mean glycosylated haemoglobin A1C levels were within normal limits but higher in HIVneg (5.5±0.49 vs 5.8±0.47, p<0.001). Six (5%) HIVneg and one HIVpos (0.9%) had previously undiagnosed diabetes with A1C levels greater 6.5%. The mean duration of HIV infection was 7.2±3.3 years. All PLWH were on ART with a mean duration of 5.3±3.1 years and 75% had undetectable viral load. Of those who had detectable viral low, the median number of copies/mL was <150.

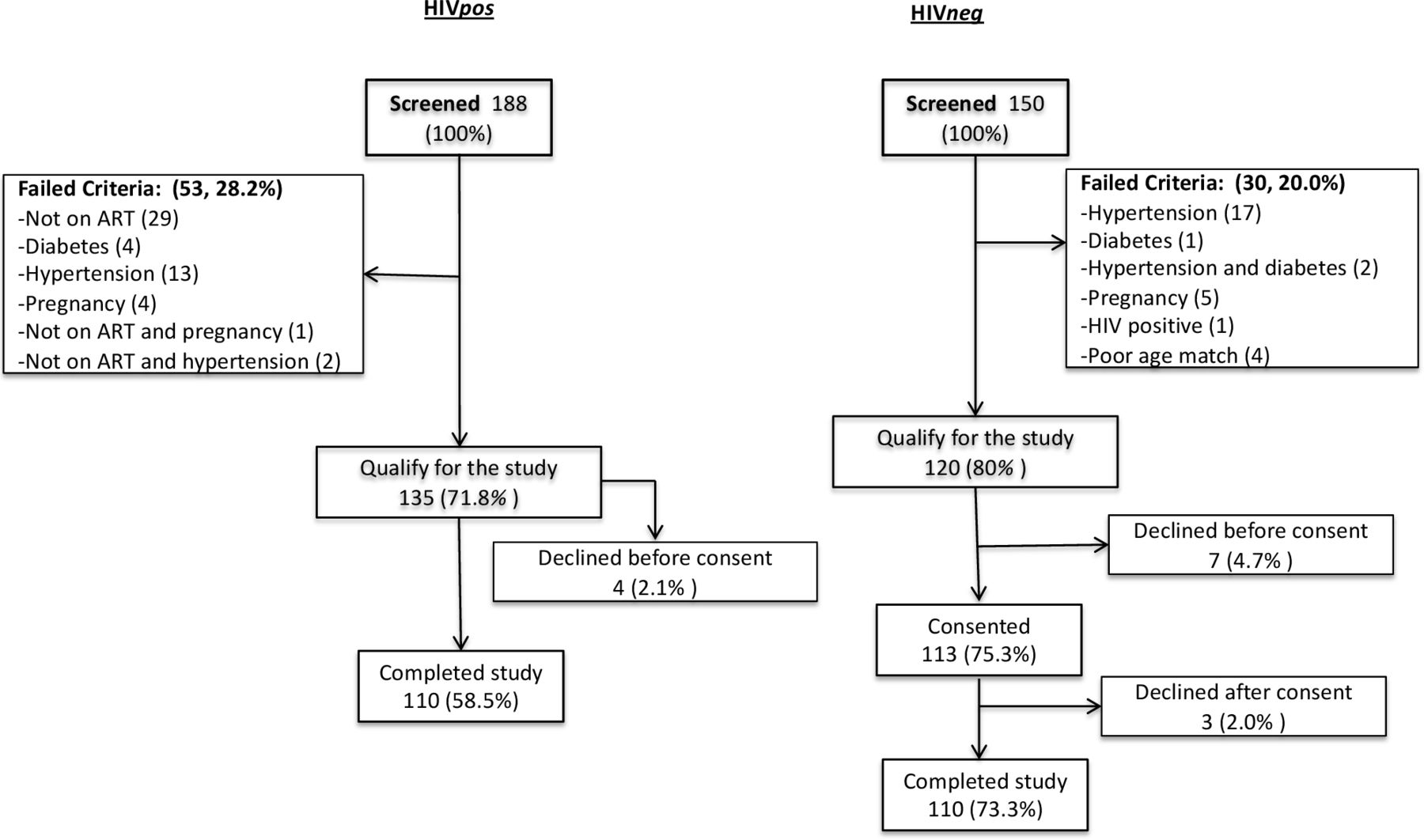{kind=link}
Enrolment of study participants. ART, antiretroviral therapy.
Characteristics of study participants
Echocardiographic parameters
Table 2 describes echocardiogram parameters between PLWH and HIVneg. Mean LVEF was 59% and the lowest EF was 45%, seen in only one participant. PLWH had a higher LV mass and LVMI to body surface area compared with HIVneg. LAVI was slightly larger in PLWH but the difference was not statistically significant. Diastolic function parameters were comparable between the two groups except for septal mitral annular tissue Doppler velocity which was slightly lower in PLWH compared with HIVneg (11.2±2.2 vs 11.8±2.5, p=0.04, respectively). There were 46 subjects (41.2%) in each group with trace or no tricuspid regurgitation. DD was rare in this group with 98.2% of the study participants with normal diastolic function. Only 1 PLWH (0.01%) participant had grade 1 DD in the setting of slightly depressed EF. Similarly, in the HIVneg group only 1 (0.01%) had abnormal diastolic function, at grade II. There were two participants (0.02%) in each group with indeterminate diastolic function.
Echocardiogram parameters by HIV status
Table 3 describes the relationship between HIV status and echocardiogram parameters in unadjusted and adjusted models. After adjusting for systolic, diastolic blood pressures, BMI, smoking history, haemoglobin A1C, LDL and HDL cholesterol levels, LVMI was 5.76 g/m2 higher in PLWH (p=0.01) compared with HIVneg. LAVI was also larger by 2.77 mL/m2 (p=0.02) in the PLWH (p=0.02) compared with HIVneg. Mitral annular septal e’ velocity was lower but no longer significant in comparison to the unadjusted model. There were no interaction effects between HIV status and sex on any of the echocardiographic parameters.
Relationship between HIV status and echocardiogram parameters in unadjusted and adjusted models
Effect of HIV disease characteristics on parameters of diastolic function
Among HIV-infected group, nadir CD4 +T cell count, current CD4 +T cell count, years on ART, years since HIV diagnosis were not associated with diastolic function parameters after adjusting for the cardiovascular risk factors in the adjusted models. Similarly, LVMI and LAVI were not associated to nadir or current CD4 count. LVEF was 0.73% lower per year since HIV diagnosis (p=0.018).
Discussion
With emerging data suggesting HIV as a risk factor for heart failure,6 studies evaluating early manifestation of cardiac dysfunction could help elucidate factors associated with increased risk and unique mechanisms of how HIV leads to clinical heart failure. In this study, we aim to evaluate the burden of DD in a contemporary, ART-treated and well characterised group of individuals with HIV infection without significant comorbidities. We found that in PLWH with limited confounding factors of hypertension and diabetes, the prevalence of DD to be very low with only 2.7% of PLWH with either grade I or indeterminate diastolic function. The prevalence of diastolic function was similar to the HIVneg group. Despite the low prevalence of DD however, PLWH had higher LVMI and LAVI.
The majority of studies evaluating the prevalence of DD have been reported from developed countries where the prevalence of cardiovascular risk factors such as diabetes, hypertension, metabolic syndrome, IV drug use and mode of HIV infection are different.7 13 Studies in sub-Saharan Africa on the other hand have included symptomatic,38 hospitalised or untreated PLWH with advanced immune dysfunction.24 25 In our study of ART-treated PLWH with relatively normal CD4 +T cell counts, we specifically sought to enrol participants without known cardiovascular risk factors of diabetes or hypertension which promote DD. As such, our findings are in contrast to a systematic review and meta-analysis that showed pooled prevalence of 29.3%7 where studies included individuals with and without known cardiovascular risk factors. Buggey39 et al have previously reported the prevalence of DD in older (mean age 52 years), ART-treated PLWH in Uganda to be 45.5% (compared with 36.8% in HIVneg controls) which was similar to reported prevalence in Western countries ranging from 26% to 50%.13 40 Notably their cohort had a high prevalence of hypertension (89%) and diabetes (26%) which may have significantly confounded the prevalence of DD attributable to HIV infection. Our findings are unique in that we are among the first to report the prevalence of DD and its parameters in an African cohort relatively free of diabetes or hypertension.
We applied the 2016 ASE guidelines to determine the presence of DD. These criteria rely on discrete echocardiographic variables (LVEF, average E/e′ ratio, septal or lateral e’ velocity, tricuspid regurgitation velocity, E/A ratio and LA volume index) and are known to be more stringent and have greater specificity than prior guidelines.37 Comparing prevalence estimates using the 2009 vs the 2016 ASE guidelines in the Women’s Interagency HIV Study, 18% of subjects with grade I DD were reclassified as normal and the prevalence of DD decreased from 41% to 19%.41 The presence of DD with the 2016 criteria also correlated better with heart failure biomarkers and clinical symptoms.41 42 Interestingly, however, the study by Buggey et al in Uganda also used 2016 ASE criteria for diastolic function assessment and reported a significantly higher prevalence of DD what was mostly grade I. It is possible that traditional cardiovascular risk factors may be strong effect modifiers in the presence of HIV infection for the development of DD.
Despite the low prevalence of DD, PLWH in this study had higher LV mass consistent with previous echocardiogram13 21 and CT43 44 studies. In a relatively young cohort (mean age of 43 years) without history of hypertension, it is interesting to note early development of increases in LV mass potentially suggesting the role of HIV infection in the pathogenesis of these early subclinical changes. Increase in LV mass in Multi-Ethnic Study of Atherosclerosis, a large ethnically diverse cohort, was associated with increased inflammatory markers and a 7.5-fold increased risk of cardiovascular death and 5.4-fold increase in developing heart failure.45–47 Individuals with other inflammatory conditions such as rheumatoid arthritis48 and ankylosing spondylitis49 have also been shown to have increased LV mass, and LV hypertrophy correlating with disease activity and higher inflammatory markers. In our cohort, there was no association of LV mass with nadir CD4 or current CD4 +T cell counts as reported in some studies.13The long-term clinical progression and relevance of increased LVMI in this relatively young cohort warrants further investigation.
Despite the low prevalence of DD in this group, left atrial size was greater in PLWH compared with the HIVneg individuals. Left atrial size reflects severity and chronicity of DD better than other parameters of diastolic function and dilation predicts future risk of atrial arrhythmias and stroke.36 Whether elevated systemic inflammation mediates increased atrial arrhythmic risk among PLWH warrants further study.
Study limitations
Although the study presents a contemporary group of PLWH in sub-Saharan Africa with few traditional cardiovascular risk factors and access to ART, the mean age of the cohort was relatively young. Therefore, the generalisability of our findings is limited to similar groups. For the purposes of this study, we targeted PLWH without known risk factors of hypertension or diabetes. In doing so, we may have excluded people who are at higher risk of developing subclinical changes either due to the inflammatory milieu that occurs as a result of the HIV infection itself, the ART or the combined effects of traditional cardiovascular risk factors with HIV infection. Our sample size was relatively modest and although we powered the study by lowering prior estimates of DD to account for exclusion of participants with traditional cardiovascular risk factors, we identified a prevalence much lower than anticipated which is likely due to the unique design of our study and more stringent DD criteria. Thus, our study may have been underpowered to detect true differences in the prevalence between each group. These novel prevalence estimates, however, can be of use to the scientific community to guide future study in this area. Our study is a cross-sectional study, and we are limited in our ability to make any causal inferences. It is likely that myocardial dysfunction in this population is a continuum of structural and functional alterations which need to be evaluated prospectively. We were unable to investigate relationships between circulating inflammatory markers and echocardiographic abnormalities and are thus unable to infer mechanistic pathways.
Conclusion
Contrary to prior reports, we demonstrate a very low prevalence of DD in a group of ART treated PLWH using contemporary professional guidelines to detect DD. Despite the low prevalence of frank DD, however, we identified a tendency of LV mass increase, enlargement of left atria in PLWH which are not explained by traditional risk factors. Environmental and cardiovascular disease risk factors such as diabetes, hypertension may be significant modifiers for development and progression of DD in HIV-positive population.
Data availability statement
Data are available on reasonable request. The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by Moi University Institutional Research and Ethics Committee (IREC) Approval # 0001536, Duke University Institutional Review Board #Pro00068891, the Vanderbilt Institutional Review Board #160181.
Acknowledgments
The investigators gratefully acknowledge the participants who donated their time and energy toward this study and the advancement of scientific knowledge.
References
Footnotes
Twitter @BethelWolduMD
Contributors BW and GSB conceived the study, analysed the data, and drafted the manuscript. All authors reviewed manuscript critically for important intellectual content and all authors have read and approved the manuscript submitted. GSB accepts full responsibility for the finished work and/or the conduct of the study, had access to the data, and controlled the decision to publish.
Funding This project was supported by National Institutes of Health (NIH) Research Training Grant R25 TW009337, funded by the Fogarty International Centre, the NIH Office of the Director, the National Institute of Mental Health, and the National Heart, Lung and Blood Institute. BW was supported by the NIH Research Training grant T32 HL007227-41/T32 HL007227-42 grant.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.