Article Text

Abstract
Background The Toronto Aortic Stenosis Quality of Life Questionnaire (TASQ) is a validated instrument for assessing quality of life (QoL) in patients with severe aortic stenosis (AS). In this study, we evaluated health status outcomes, based on the TASQ, in patients with severe AS undergoing transcatheter aortic valve replacement (TAVR) or surgical aortic valve replacement (SAVR).
Methods The TASQ registry was a prospective observational registry. Patients with severe AS from nine centres in Europe and one in Canada underwent either SAVR or transfemoral TAVR. Patients completed the TASQ, Kansas City Cardiomyopathy Questionnaire and Short Form-12 V.2 prior to the intervention, predischarge, and at 30-day and 3-month follow-ups. Primary end point was the TASQ score.
Results In both the TAVR (n=137) and SAVR (n=137) cohorts, significant increases were observed in all three scores. The overall TASQ score improved as did all but one of the individual domains at 3 months after the intervention (p<0.001). TASQ health expectations were the only domain which worsened (p<0.001). Across TASQ subscores, significant changes were evident from the time of discharge in the TAVR and 30-day follow-up in the SAVR cohort. In a categorical analysis of the TASQ, 39.7% of the TAVR group and 35.0% of the SAVR group had a substantially improved health status at 3 months compared with baseline.
Conclusions The TASQ captured changes in QoL among patients with severe AS who were treated with TAVR or SAVR. QoL improved substantially after either intervention, as indicated by changes in the TASQ overall score at 3 months.
Trial registration number NCT03186339.
- aortic diseases
- heart valve prosthesis implantation
- quality of healthcare
- outcome assessment
- healthcare
- aortic valve stenosis
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- aortic diseases
- heart valve prosthesis implantation
- quality of healthcare
- outcome assessment
- healthcare
- aortic valve stenosis
Key questions
What is already known about this subject?
The Toronto Aortic Stenosis Quality of Life Questionnaire (TASQ) is a validated instrument for assessing quality of life (QoL) in patients with severe aortic stenosis (AS).
What does this study add?
We evaluated health status outcomes, based on the TASQ, in patients with severe AS undergoing transcatheter aortic valve replacement (TAVR) or surgical aortic valve replacement.
QoL improved substantially after either intervention, as indicated by changes in the TASQ overall score at 3 months.
How might this impact on clinical practice?
With the TASQ, a validated tool for QoL assessments of patients undergoing surgical or TAVR is available.
Introduction
Patients with severe aortic stenosis (AS) are often elderly with multiple comorbidities.1 The symptom burden from severe AS can disrupt their ability to participate in daily activities and adversely affect their quality of life (QoL).2 The primary aim of treating AS is to prolong survival while considering the effect of interventions on QoL when assessing the risks and benefits of treatment.3 Aortic valve (AV) replacement using either surgical aortic valve replacement (SAVR) or transcatheter aortic valve replacement (TAVR) improves survival in patients with severe symptomatic AS,4 and evidence suggests these procedures also improve QoL.5–9
The Toronto Aortic Stenosis Quality of Life Questionnaire (TASQ) is a validated QoL instrument for patients undergoing TAVR or SAVR.10 11 This questionnaire reflects AS-specific symptoms and how they affect a patient’s physical and mental well-being, as well as evaluates patients’ assessment of their general health. It is short, convenient to use and specific to patients with AS, providing an accurate picture of QoL in patients with severe AS, before and after treatment.11
We performed a multinational prospective study to evaluate health status outcomes, based on the TASQ, in patients with severe symptomatic AS treated with either TAVR or SAVR. The study’s principal results have been reported previously.11 TAVR and SAVR may be used in different patient populations and can be associated with different procedure-related complications, which may result in differences in health status. Therefore, separate analyses of patients who had TAVR and SAVR may provide additional relevant information on QoL outcomes in patients with AS undergoing different interventions. TASQ-based health status outcomes for study patients with severe AS are now reported separately for patients who underwent TAVR and SAVR.
Methods
The TASQ registry was a prospective observational registry with a follow-up period of 3 months.10 12 Patients with severe symptomatic AS were recruited from nine European centres (Austria/Germany,2 France,2 Italy,2 Spain2 and the UK1) and one centre in Canada, with the intention of having at least two sites per language. Patients underwent either transfemoral (TF) TAVR using the balloon expandable SAPIEN three valve (Edwards Lifesciences), or SAVR using any commercially available surgical valve. Treatment decisions were made by the local heart team, based on standard in-house protocols, and were independent of the study. Recruitment was intentionally not limited to comparable cases as this would have excluded surgery in young patients with low surgical risk and TAVR in older patients with high or prohibitive surgical risk. Patients were excluded from the study if they were unable to complete the questionnaire due to cognitive impairment.
The principal objective of the registry was to validate the TASQ questionnaire in patients with severe symptomatic AS undergoing TAVR or SAVR.
TASQ, Kansas City Cardiomyopathy Questionnaire (KCCQ) and Short Form-12 V.2 (SF-12v2) questionnaires
For this registry, the TASQ was produced in English (available open access10 12) and validated translations were produced in French, German, Italian and Spanish. Patients were required to complete the TASQ prior to the intervention (baseline), pre-discharge, and at 30-day and 3 months follow-up. The scoring of the TASQ10 is based on a consistent 7-point scale for each of the 16 questions, covering response options from “not very much” to “very much”. The TASQ consists of five domains: physical symptoms (questions 1 and 14), physical limitations (questions 3, 6, 7 and 15), emotional impact (questions 2 and 8–13), social limitations (questions 4 and 5) and health expectations (question 16). Each question has a maximum score of 7, giving the complete questionnaire a maximum total score of 112, with a higher score indicating improved QoL. The full questionnaire is available online (wwwtasq-qcom.
Patients also completed the KCCQ. The KCCQ13 is a 23-item self-administered questionnaire that addresses specific health domains, including physical limitation, symptom frequency and burden, QoL, social limitation, symptom stability and self-efficacy—the first four are combined into an overall summary scale. Values for the domains range from 0 to 100, with higher scores indicating lower symptom burden and better QoL. The self-efficacy domain is designed to assess whether or not patients feel they have the knowledge and skills to manage their heart failure as an outpatient. The KCCQ has been used in several AS-related analyses.7 8 14
Generic health status was assessed with the SF-12v2. The Short Form-12 (SF-12) is a reliable and valid measure of generic health status that provides overall physical and mental component summary scores.15 Scores are standardised using norm-based methods around a mean of 50, with higher scores indicating better health status.16 The maximum score for both physical and mental component summary scores is 100.
Statistical analysis
The primary endpoint was the TASQ score. The primary analysis evaluated patients’ health status in the TAVR and SAVR cohorts separately. Missing health status (TASQ) values were replaced by the mean score, provided that the patient had responded to ≥50% of the questions for that subscale. Mean changes in health status scores at all time points were compared with baseline within each treatment group using paired t-tests.
Categorical analyses incorporating both health status (TASQ) and survival were performed to provide further perspective on the effect of these interventions over time. For these analyses, ordinal categories were defined as death, worse (decrease of >5% vs baseline), no change (change of between –5% and 5%), slightly improved (increase of >5%–10% vs baseline), moderately improved (increase of 10%–20%) and substantially improved (increase of >20%).
Baseline characteristics were compared between the cohorts using two-tailed t-tests for continuous variables and χ2 test or Fisher’s exact test for categorical variables (p values <0.05 were regarded as statistically significant). The comparison provided proof for the assumption that the two patient populations were quite different. While we provide statistical measures for a comparison of patients who underwent TAVR and SAVR, we dismissed any further attempt to adjust or match the two groups.
Statistical analysis was performed using SPSS V.24.0.
Results
Overall, 274 patients were included in the analysis, of which 137 underwent TAVR and SAVR, respectively (table 1).
Patient characteristics
TASQ in patients undergoing TAVR
The mean age of patients in the TAVR cohort was 82.7 years, and 43.1% were female. Coronary artery disease (CAD, 47.4%), previous hospital admission for congestive heart failure (CHF, 37.2%) and a history of atrial fibrillation (AF, 36.4%) were common in this group. The mean Society of Thoracic Surgeons (STS) risk score among patients undergoing TAVR was 5.22. At baseline, the mean TASQ score among patients undergoing TAVR was 67.1, while the mean KCCQ score was 52.4 and the mean SF-12v2 score was 36.9 (table 1).
Among patients undergoing TAVR, considerable and statistically significant increases were observed in the overall TASQ score, and in all but one of the single-domain TASQ scores, at 3 months after the intervention (p<0.001) (table 2), health expectations worsened (p<0.001). Corresponding changes were observed with the KCCQ and SF-12v2 questionnaires at all time points (online supplemental figures 1 and 2).
Supplemental material
Supplemental material
Within-group change in TASQ after TAVR or SAVR
Significant improvements in the overall TASQ score and in the physical symptoms, physical limitations and emotional impact TASQ domains were observed at hospital discharge (p<0.001) and remained significant thereafter (figure 1). Significant changes in the social limitations domain (improvement) and health expectations domain (worsening) were only seen from 30 days onwards (p<0.001). When the baseline score for the overall TASQ was set to 100%, the absolute increase in the overall TASQ score was approximately 12% at discharge, 26% at 30 days and 30% at 3 months (figure 2).
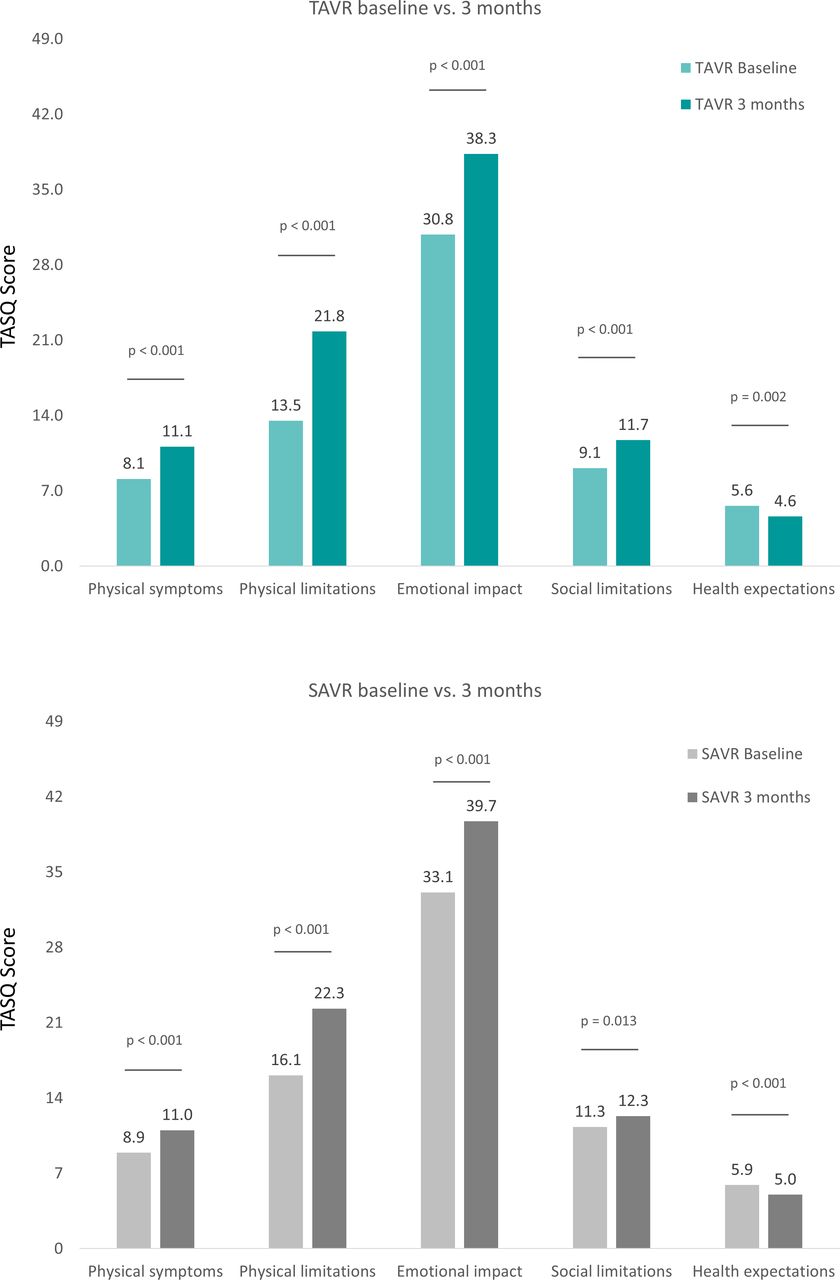
Absolute TASQ score at baseline and 3-month follow-up. Bars between columns represent the maximum achievable score per domain. SAVR, surgical aortic valve replacement; TASQ, Toronto Aortic Stenosis Quality of Life Questionnaire; TAVR, transcatheter aortic valve replacement.

TAVR vs SAVR at baseline, discharge, 30 days and 3 months after the intervention, adjusted for differences in baseline TASQ score. SAVR, surgical aortic valve replacement; TASQ, Toronto Aortic Stenosis Quality of Life Questionnaire; TAVR, transcatheter aortic valve replacement. *P<0.05, ***P<0.001 vs baseline.
At 3 months, two patients (1.7%) in the TAVR group had died and 5.8% had a worse health status compared with the baseline situation. However, the proportion of patients categorised as ‘worsened’ declined continuously from discharge through the 30-day follow-up and up to 3 months (figure 3). At 3 months, 39.7% of the TAVR group had a ‘substantially improved’ health status compared with baseline.

{kind=link}
{kind=link}
{kind=link}
Proportion of patients who underwent TAVR and SAVR achieving specific levels of clinically relevant change in health status (TASQ score and survival status). P values are derived from the Mann-Whitney U test for these categorical analyses, ordinal categories for clinically relevant changes in the TASQ (plus survival status) were defined as death, worse (decrease of >5% vs baseline), no change (change of between –5% and <5%), slightly improved (increase of 5% to <10% vs baseline), moderately improved (increase of 10% to <20%), substantially improved (increase of ≥20%). SAVR, surgical aortic valve replacement; TASQ, Toronto Aortic Stenosis Quality of Life Questionnaire; TAVR, transcatheter aortic valve replacement.
TASQ in patients undergoing SAVR
The mean age of patients in the SAVR cohort was 72.5 years and 31.4% were female. The most common concurrent cardiac diseases were AF (14.9%) and CAD (10.2%). Mean STS risk score was 2.45. At baseline, the mean TASQ score was 75.3; the mean KCCQ score was 68.1; and the mean SF-12v2 score was 42.4 (table 1).
Among patients who underwent SAVR, considerable and statistically significant increases were observed in the overall TASQ score, and in all but one of the single-domain TASQ scores, at 3 months after the intervention (p<0.001) (table 2). Again, the health expectations domain worsened at 3 months (p<0.001). Corresponding changes were observed with the KCCQ and SF-12v2 questionnaires at all time points (online supplemental figures 1 and 2).
Significant improvements were not observed for any TASQ (and KCCQ and SF-12v2) scores at the time of discharge but were seen from 30 days onwards for the overall TASQ score, and the physical symptoms, physical limitations and emotional impact TASQ domains (p<0.001). The social limitations domain had worsened at discharge (p<0.001), but by 3 months, a significant improvement from baseline was seen (p=0.013). The health expectations domain did not differ significantly from baseline at discharge or 30 days. When the baseline score for the overall TASQ was set to 100%, the absolute change in the overall TASQ score was approximately –3% at discharge, +12% at 30 days and +20% at 3 months (figure 2).
At 3 months, two patients (1.7%) in the SAVR group had died and 13.0% had a worse health status compared with the baseline. However, the proportion of patients categorised as worsened declined continuously from discharge through the 30-day follow-up and up to 3 months (figure 3). At 3 months, 35% of the SAVR group had a substantially improved health status compared with baseline.
TASQ–TAVR versus SAVR
Recruitment was intentionally not limited to comparable cases as this would have excluded surgery in young patients with low surgical risk and TAVR in older patients with high/prohibitive surgical risk. Compared with SAVR, patients undergoing TAVR were older (p<0.001), more often female (p=0.046) and more often had CAD (47.4% vs 10.2%, p<0.001) or previous hospital admission for CHF (37.2% vs 9.8%, p<0.001). The STS risk score was higher in patients undergoing TAVR (5.22 vs 2.45). QoL at baseline was lower in the TAVR cohort, as indicated by the mean overall TASQ score (67.1 vs 75.3, p<0.001), KCCQ score (52.4 vs 68.1, p<0.001) and SF-12v2 score (36.9 vs 42.4, p<0.001) (table 1). On a descriptive basis, TAVR had a relatively higher improvement of the patients who had TASQ than those who had SAVR, which was particularly evident at discharge and 30 days. Despite these differences and the ones at baseline, the difference in the TASQ between patients who underwent TAVR and SAVR was small at 3 months.
Discussion
This study demonstrated that the TASQ captured changes in QoL among patients with severe symptomatic AS who were treated with TAVR or SAVR. Changes were detected soon after intervention—from the time of hospital discharge in patients undergoing TAVR and from 30 days postintervention in patients who underwent SAVR. QoL improved substantially after TAVR and SAVR, as indicated by changes in the TASQ overall score at 3 months. Significant improvements were also seen in four of the five individual TASQ domains (physical symptoms, physical limitations, emotional impact and social limitations) at this time point.
The potential benefits of AV interventions on QoL for patients with AS have been demonstrated in previous studies, using a variety of QoL tools.5–9 14 17–19 The TASQ is the first AS-specific QoL instrument to be developed12 and has been validated for use in patients undergoing TAVR and SAVR.10 11 The results of the current study add to the body of evidence about the TASQ. The main analysis of the study, which combined the TAVR and SAVR cohorts, found that the TASQ was a responsive measure of QoL in patients with severe AS and was sensitive to changes from discharge up to 3 months after AV interventions.11 The overall TASQ score increased significantly, with improvements seen in the domains of physical symptoms, physical limitations, emotional impact and social limitations at 3 months.11 The results of the current analyses of the separate TAVR and SAVR cohorts are generally consistent with the principal analysis. The overall TASQ score improved significantly in both cohorts at 3 months, as did scores for the physical symptoms, physical limitations, emotional impact, and social limitations domains. The health expectations domain worsened in both cohorts in the current analysis. A slight decrease in this domain was also seen in the combined analysis.11
In the current study, a QoL benefit was seen as early as discharge in the TAVR cohort, but not the SAVR cohort, which may be related to the type of intervention. All patients undergoing TAVR underwent TF-TAVR. Comparative studies and a meta-analysis have reported a short-term QoL advantage with TF-TAVR (but not with other TAVR routes) compared with SAVR.5 8 9 17 20 Various QoL instruments were used in these studies, such as the KCCQ, the generic SF-12 or SF-36, and EuroQol 5 Dimension. Studies comparing TF-TAVR and SAVR in patients at high or intermediate surgical risk found that the advantage did not persist in the long term; after 6–12 months, there was no significant difference in QoL benefit between TAVR and SAVR.5 8 9 17 However, a study involving patients with severe AS at low surgical risk found that TF-TAVR was associated with better health status (assessed using the KCCQ) compared with SAVR at 1, 6 and 12 months postintervention.20
The significant differences in baseline characteristics between the TAVR and SAVR cohorts precluded formal statistical comparison of changes in TASQ scores between these groups in the current analysis because adequate adjustment/propensity score matching was not feasible. Patients undergoing TAVR were older, predominantly female, and had a higher prevalence of CAD and rhythm disturbances. Carotid artery stenosis, cerebrovascular disease and peripheral vascular disease were also more common in patients undergoing TAVR, and surgical risk scores were higher. These differences likely accounted for the lower overall QoL seen in patients undergoing TAVR at baseline (as indicated by TASQ, KCCQ and SF-12v2 scores). Despite a formal comparison not being possible, a few points of potential interest were noted. Although the TASQ overall score was substantially lower at baseline in the TAVR group, only a small difference in scores was seen between the TAVR and SAVR groups at 3 months. A significant improvement versus baseline was seen at discharge in the TAVR cohort, but only from 30 days in the SAVR cohort. The magnitude of the improvement in overall TASQ score during the 3 months postintervention also appeared to be greater in the TAVR cohort. Taken together, these findings suggest that patients undergoing TAVR gained on patients who had SAVR in terms of their QoL during the first 3 months post-intervention.
Strengths and limitations
Recruitment was aimed at facilitating equal distribution of patient numbers across different languages. Patients were evaluated to make sure they had the cognitive ability to complete the questionnaires. The TAVR group only included patients who underwent TF-TAVR as this was the standard procedure used at participating centres. Comparison of changes in TASQ between TAVR and SAVR recipients was attempted, as recruitment was intentionally not limited to comparable cases as this would have excluded surgery in young patients with low surgical risk and TAVR in older patients with high or prohibitive surgical risk.
Conclusions
The TASQ captured changes in QoL among patients with severe symptomatic AS who were treated with TAVR or SAVR. Furthermore, the results suggest that the TASQ reflects changes earlier after an intervention, particularly after TAVR. QoL improved substantially after both TAVR and SAVR, as indicated by changes in the TASQ overall score at 3 months.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
The study protocol was approved by the independent ethics committee or the institutional review board at each centre. The registry was conducted in accordance with the Declaration of Helsinki and its amendments, as well as country-specific laws and regulations. Patients provided written informed consent.
Acknowledgments
Data were captured using the s4trials Software provided by Software for Trials Europe GmbH, Berlin, Germany.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors SK, RS, LSt, CL, LSy, JK, MT, PB and DF were involved in the conception and design of the registry. The remaining authors gave feedback on the final protocol and included patients. SK, CL and PB drafted the manuscript and all the other authors revised the article for important intellectual content. All authors gave final approval of the version to be published and are fully accountable for the content of the manuscript. PB accepts full responsibility for the work and/or conduct of the study, had access to the data and controlled the decision to publish. Study coordinators: Michelle Dimas, Mamta Kapoor, Jermel Pierre (Toronto, Canada); Mervyn Andiapen, Rita Adrego, Adedolapo Adeleke (London, UK); Mathilde Le Marchand, Genevieve Mottin, Sharanya Logeswaran (Massy, France); Reza Farnoud (Bichat, France); Florian Fulisch, Nathalie Guessefeld, Renate Kahl (Kiel, Germany); Mattia Lunardi, Ilaria Franzese (Verona, Italy); Mira Stolcova (Florence, Italy); Maria Angeles Carmona, Teresa Hemodinamica (Barcelona, Spain); Elena Paz, Maria Rita Soler Martin (Coruna, Spain).
Funding This work was supported by a research grant provided by Edwards Lifesciences (Nyon, Switzerland) to the Institute for Pharmacology and Preventive Medicine (Cloppenburg, Germany).
Competing interests PB is the representative of the Institute for Pharmacology and Preventive Medicine, Cloppenburg, Germany. LS, JK and MT are employees of the funder. All centres were paid by IPPMed for the enrolment and documentation of patients.
Provenance and peer review Not commissioned; internally peer reviewed.