Article Text

Abstract
Objective Between 2009 and 2013, the National Heart Foundation of Australia ran mass media campaigns to improve Australian’s awareness of acute coronary syndrome (ACS) symptoms and the need to call emergency medical services (EMS). This study examined the impact of this campaign on emergency department (ED) presentations and EMS use in Victoria, Australia.
Methods The Victorian Department of Health and Human Services provided data for adult Victorian patients presenting to public hospitals with an ED diagnosis of ACS or unspecified chest pain (U-CP). We modelled changes in the incidence of ED presentations, and the association between the campaign period and (1) EMS arrival and (2) referred to ED by a general practitioner (GP). Models were adjusted for increasing population size, ACS subtype and demographics.
Results Between 2003 and 2015, there were 124 632 eligible ED presentations with ACS and 536 148 with U-CP. In patients with ACS, the campaign period was associated with an increase in ED presentations (incidence rate ratio: 1.11; 95% CI 1.07 to 1.15), a decrease in presentations via a GP (adjusted OR (AOR): 0.77; 95% CI 0.70 to 0.86) and an increase in EMS use (AOR: 1.10; 95% CI 1.05 to 1.17). Similar, but smaller associations were seen in U-CP.
Conclusions The Warning Signs Campaign was associated with improvements in treatment seeking in patients with ACS—including increased EMS use. The increase in ACS ED presentations corresponds with a decrease in out-of-hospital cardiac arrest over this time. Future education needs to focus on improving EMS use in ACS patient groups where use remains low.
- acute coronary syndrome
- chest pain
- delivery of health care
- outcome assessment
- health care
Data availability statement
No data are available. Data are not available from the authors due to contractual arrangements. Data are available on request from the Victorian Department of Health and Human Services.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known about this subject?
Only 40%–60% of patients with acute coronary syndrome (ACS) present to the hospital by ambulance. Many attend their local doctor before presenting, and delays in presenting to the hospital are common and place patients at risk of out-of-hospital cardiac arrest.
The impact of public mass media campaigns on treatment seeking for ACS to date has varied.
What does this study add?
This population-based study used data from 33 emergency departments (EDs) to examine the effect of a large mass media campaign by the National Heart Foundation of Australia which addressed the known barriers to patient delay and ambulance use.
We found that campaign period was associated with an 11% increase in ED for ACS, and a 10% increase in emergency medical services (EMS) use by patients with ACS. Presentations via local doctors decreased.
We also studied the knock-on effect on patients diagnosed with unspecified chest pain, and found a smaller increase (8%) in presentations and EMS use (3%).
How might this impact on clinical practice?
Our study provides evidence that education targeting the barriers known to influence patient’s prehospital decision-making is effective. Targeting regions and populations at high risk may be a better use of resources.
The increase in ACS presentations in our study suggests such education may even save lives by preventing out-of-hospital cardiac arrest.
Introduction
Improving patient recognition and response to acute coronary syndrome (ACS) symptoms is key to optimising outcomes through early reperfusion.1 A particularly important public response is the use of emergency medical services (EMS) which ensures early diagnosis, treatment and transport to a hospital with cardiac capabilities.2 However, only 40%–60% of patients with ACS arrive to the hospital by EMS.3–5
In the mid-2000s, the National Heart Foundation of Australia (NHFA) recognised the need to improve EMS use for ACS in Australia.6 At that time, the barriers to EMS use were ignoring/denying symptoms, embarrassment and preference to see a local doctor before presenting to the hospital.6 The NHFA designed a large mass media campaign to improve Australian’s ACS symptom knowledge and address barriers to EMS use.7 The campaign ran intermittently across the country between 2009 and 2013, and had significant reach with approximately 66% of patients with ACS reporting having seen the campaign.8 Despite this, single centre studies have shown no impact of this campaign on EMS use in patients presenting with chest pain or those diagnosed with ACS.9–11 However, statistical power may be an issue in these studies. A recent population-based study of calls to EMS for chest pain reported an increased effect during the campaign,12 which highlights the need for larger multi-centre studies to address this question.
This study aimed to examine the impact of the NHFA Warning Signs Campaign on ACS EMS use and emergency department (ED) presentations in the Australian state of Victoria. Secondary aims were to (1) examine the impact of the campaign on ED presentations via general practitioners (GPs—ie, local doctors) and (2) to examine EMS use and ED presentation numbers in patients presenting to ED with chest pain but given an unspecified diagnosis to examine potential changes in the ‘worried well’.
Methods
Study design and setting
This retrospective, observational study used data between 2003 and 2015 from the Victorian Emergency Minimum Dataset (VEMD) provided by the Victorian Department of Health and Human Services.
Over the study period, the population of Victoria increased from 4.9 million to 5.9 million. At the time of this study, EMS services were provided by a single ambulance service, Ambulance Victoria, in a user pays system for those not covered by a government pension, health insurance or EMS subscription (over half of the population). Public hospital healthcare, including ED visits, is free to all Australian citizens and most permanent residents of Australia. Private healthcare is on a user pays system. In 2015, there were 50 EDs (34 public, 5 public specialties and 11 private) within Victoria—however, the majority (~93%) of emergency presentations are made to public EDs.
Data source and inclusion criteria
The Victorian Department of Health and Human Services maintains administrative data on all emergency presentations to Victoria’s public hospitals in the VEMD. This dataset includes patient demographics, mode of arrival (eg, self or EMS), patient referral source (eg, self, GP, another hospital) and ED diagnosis in ICD-10-AM (International Classification of Diseases) format.
Deidentified data were extracted from the VEMD for cases aged ≥20 years presenting to 33 EDs (one ED with partial data for the study period and five specialty EDs were excluded). Inclusion criteria for this study were an ED ICD-10 code of ACS (I200, I213, I214, I219) or unspecified chest pain (U-CP, R074); residence in a private home (in order to specifically gauge the public impact of the campaign); and Victorian residency (determined from residential postcode). Non-Victorian Australian residents were excluded due to a lack of consistency in campaign exposure across the nation; international visitors were also excluded. Validations of VEMD ACS data at one hospital showed high accuracy for key variables and diagnosis.13
National Heart Foundation’s Warning Sign Campaign
The NHFA intermittently ran a paid mass media Warning Signs Campaign in Victoria between 2009 and 2013 to increase awareness of ACS symptoms among residents and to encourage them to call EMS on experiencing these symptoms. Media included two television advertisements, radio and print.8 14
Outcomes measures
The primary outcomes were ACS EMS arrivals and ED presentations. EMS arrivals occurred when patients self-presented to an ED via EMS transport (ie, were not referred by a GP). ED presentations were the number of patients with ACS presenting to ED. Secondary outcomes were ED presentations via a GP referral (patients who were referred to the ED via a GP), and U-CP EMS use and ED presentations.
Statistical analysis
Monthly ED data for the period July 2003 to December 2015 were included in this study. Campaign activity commenced in October 2009 and concluded in August 2013.
Baseline characteristics of ED patients are summarised as counts and percentages with stratification by arrival mode (self, EMS or via a GP). The association between campaign activity and mode of presentation was assessed by piecewise logistic regression with separate models for direct EMS arrival and GP referral. A linear spline was created from month with knots at the month in which the campaign started (October 2009) and at the month that the postcampaign period began (September 2013). Models were adjusted for the increase in population size over the study period, winter (June–August) presentation and patient factors including age, sex, ethnicity (Australian born vs other), preferred language (English vs other), interpreter requirements (yes vs no), residential details (lives alone vs lives with others, metropolitan vs regional/rural location) and ED sub-ACS diagnosis6 (unstable angina vs acute myocardial infarction (AMI)).
Negative binomial models were applied to monthly count data to describe any increase in the incidence of ED presentations that was associated with the campaign activity. Separate models were estimated for ACS and U-CP presentations. Estimated residential population was used as an offset.
The analyses were completed using Stata V.16.0 for Windows (StataCorp). All statistical tests were two-tailed and significance was assessed at the 5% alpha level.
Patient involvement
This study used routinely collected hospital data, service providers (ambulance and ED providers) were involved in the design and study objectives. Patients and the public were not involved at any stage. Data were provided in a deidentified format, therefore dissemination of the results to study participants was not possible.
Results
ED presentations
Over the study period, there were 14 997 732 ED presentations, including 149 374 for ACS and 612 758 for U-CP. Of these, 124 632 (83%) patients with ACS and 536 148 (87%) patients with U-CP were eligible for inclusion. The majority of exclusions were due to residing in a non-private residence (59%), age <20 years (17%) or interstate/international visitor (15%).
Following adjustment, there was an 11% increase in ED presentations for ACS (incidence rate ratio (IRR): 1.11; 95% CI 1.07 to 1.15) and an 8% increase for U-CP (IRR: 1.08; 95% CI 1.05 to 1.12) during the campaign period when compared with the precampaign and postcampaign periods. When compared with patients with U-CP, those with ACS were more likely to be men, older in age, born overseas and have a language other than English as their preferred language (table 1).
A comparison of patient characteristics by mode of arrival for patients with an emergency diagnosis of acute coronary syndrome and unspecified chest pain
Patients with ACS
Of the 124 632 patients with ACS (48% with AMI), the majority (72 818, 58%) arrived by EMS without first attending a GP. The remainder self-presented (n=41 483, 33%) or presented via a GP referral (n=10 331, 8%). Of those referred by a GP, 42% (n=4325) arrived by EMS and 58% (n=6006) self-presented. When compared with EMS arrivals, GP referred patients were more likely to be men, come from the younger age groups (20–44 years, 45–64 years) and reside outside of a major city (table 1). Patients who self-presented were similarly more likely to be men and younger, but less likely to live alone.
When compared with the precampaign period, there was a significant increase in the adjusted odds of direct arrival by EMS (adjusted OR: 1.10; 95% CI 1.05 to 1.17) and a significant decrease in the adjusted odds of GP referral (OR: 0.77; 95% CI 0.70 to 0.86) during the campaign period (table 2). There were no significant changes in the adjusted odds of EMS arrival or GP referral postcampaign when compared with the campaign period (figure 1).
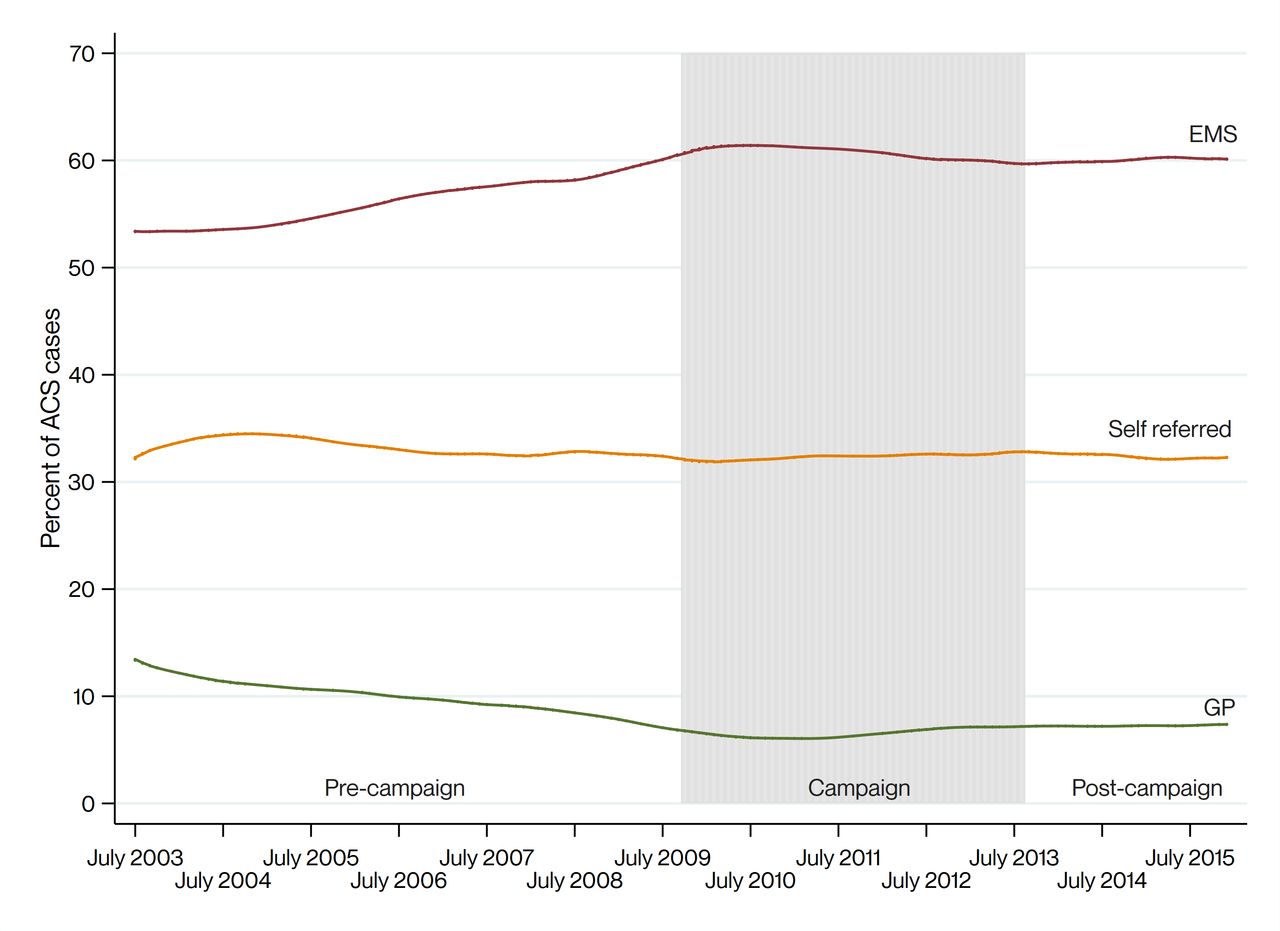
{kind=link}
Acute coronary syndrome (ACS) treatment seeking behaviour over time. EMS, emergency medical services; GP, general practitioner.
Factors associated with arrival by EMS or via local doctor in patients with ED diagnosis of acute coronary syndrome and unspecified chest pain
Adults in the younger age groups (20–44 years and 45–64 years) were significantly less likely to arrive directly by EMS and more likely to present via GP referral (table 2), as were overseas-born residents, residents who required an interpreter and residents who live outside of a major city. Men were significantly less likely to arrive directly by EMS compared with women, but GP referrals did not differ with respect to sex. Living alone was associated with an increased odds of EMS arrival.
Patients with U-CP
Of the 536 148 patients presenting with U-CP, half self-presented (n=279, 078, 52%), over one-third (212 214, 40%) arrived directly by EMS, and a smaller proportion (44 856, 8%) presented via GP referral. EMS arrivals tended to be older, be Australian-born and live alone when compared with GP referrals (table 1).
Among U-CP presentations, there were no clear trends in direct EMS arrivals or GP referrals during the precampaign, campaign or postcampaign periods (table 2). There was a modest increase in the adjusted odds of EMS arrivals during the campaign when compared with the precampaign period (OR: 1.03; 95% CI 1.00 to 1.06) and a further increase during the postcampaign period (OR: 1.04; 95% CI 1.01 to 1.08). There was a more prominent decrease in the adjusted odds of GP referral during the campaign period when compared with the precampaign period (OR: 0.79; 95% CI 0.75 to 0.82), however, this eased postcampaign when compared with the campaign period (OR: 0.93; 95% CI 0.88 to 0.98).
The trends associated with U-CP patient characteristics were similar to those reported for patients with ACS: adults in the younger age groups (20–44 years and 45–64 years) were significantly less likely to arrive directly by EMS and more likely to present via GP referral, as were overseas-born residents and people who lived outside of a major city. Men were significantly less likely than women to arrive directly by EMS and to present via GP referral. Individuals who required an interpreter were significantly more likely to be GP-referred; living alone was associated with an increased odds of EMS arrival and a significantly lower odds of being referred by a GP.
Discussion
The 5 years in which the NHFA’s mass media Warning Signs Campaign ran was associated with a 11% increase in ED presentations for ACS and a 10% increase in EMS use by patients with ACS—which was sustained in the following 2 years. We also found a smaller increase (8%) in presentations and EMS use (3%) for U-CP. Of note, was a ~22% drop in ACS presenting to ED via GP referrals during the campaign.
Our study is the largest multi-centre study in Australia to examine the impact of EMS use for the Warning Signs campaign to date. Our findings concur with two of our previous population-based studies in Victoria which found a 10.7% increase in calls to EMS for chest pain12 and a decrease in out-of-hospital cardiac arrests during the campaign period.14 The latter may explain the 11% increase in ACS presentations that our present study observed during the campaign (ie, potentially patients who averted a cardiac arrest). Findings from single-centre before-and-after studies have shown no impact of this campaign on EMS use in different regions of Australia.9–11 Statistical power is likely to be an issue in these studies, as is the varying campaign exposure across the country and the ongoing public perception that self-transport is faster.9 11
Internationally, the effect of mass media campaigns on EMS use in ACS is conflicting. A recent systematic review reported only three of five studies conducted outside Australia found an increase in EMS use following mass media campaigns.15 On closer examination, the studies that showed an effect tended to address the barriers to ambulance use16 and were adequately powered for this outcome.17 Studies reporting no change in EMS simply told the public to call EMS or had very high rates of EMS use precampaign.18 19 Our data suggest there is great value in addressing the barriers to EMS use in public education, such as not being sure about the seriousness of symptoms and embarrassment to call EMS.
Our study also demonstrated some unwanted effects on the healthcare system. While effective at increasing EMS use in ACS, the campaign period was also associated with an 8% increase in ED presentations for non-specified chest pain and a ~3% increase in EMS use in these patients. However, this only corresponds to an additional 275 ED presentations per campaign month, or an average of 8 patients per ED/month.
Given the large expense associated with mass media campaigns (~$16 million nationally20), the NHFA are unlikely to run such a large national campaign in the near future. The regional variation in EMS use for ACS, as reported in the seminal REACT (Rapid Early Action for Coronary Treatment) trial,17 is an important finding for future interventions aiming to improve EMS use for ACS. Focusing public education on regions at high-risk of ACS21 and with low EMS use may be a better use of funding and resources. As a result, we are currently conducting a step-wedge randomised controlled study focusing on educating the public in such high-risk regions (Heart Matters RCT, NCT04995900). By using a focused approach, we hope to overcome some of the issues identified in the REACT trial (eg, REACT targeted some communities with high baseline EMS use and low prehospital delay times),17 as well as minimising some of the additional burden on EMS and ED seen with a wide-spread population-wide campaign.
Limitations
The limitations of the study include the study design, which cannot show causation, and the use of administrative data. First, it is possible that other factors or small scale interventions may have contributed to findings. Second, we were unable to examine the clinical impact of increased EMS use with the available data in this study. However, previous research has found EMS use is associated with shorter times to reperfusion,4 22 and our previous research found an association between the campaign period and (1) shorter prehospital delay times8 and (2) a decrease in the incidence of out-of-hospital cardiac arrest in Victoria.14 Finally, our study used an ED administrative dataset not designed for research, which may be subject to coding errors. However, a validation study that we conducted in one centre showed high accuracy in the data used in this study, particularly demographics, ACS diagnosis and EMS use.13
Conclusion
Our findings suggest the NHFA’s Warning Signs Campaign was associated with an increase in ACS ED presentations and EMS use, and a decrease in ED presentations via GPs. Our study supports the use of public campaigns to change health seeking-behaviour for ACS. Future interventions need to focus on improving EMS use in patient groups where use remains low.
Data availability statement
No data are available. Data are not available from the authors due to contractual arrangements. Data are available on request from the Victorian Department of Health and Human Services.
Ethics statements
Patient consent for publication
Ethics approval
The Monash Human Research Ethics Committee approved this study, consent was not required as the VEMD data provided was deidentified.
Acknowledgments
We would like to acknowledge current and former NHFA staff who provided campaign information, particularly Harry Pastramis and Kelly Donnelly.
References
Footnotes
Contributors JEB and ZN conceived the study. JEB, ZN, JF, KS, PC and DS were involved in planning and funding applications. SH and JEB conducted the analysis. All authors contributed to the interpretation of findings and drafting of the manuscript.
Funding This study was supported by a Stroke Foundation Grant. KE and SH are funded by the National Health and Medical Research Council (NHMRC) Prehospital Emergency Care (PEC-ANZ) Centre of Research Excellence. ZN, JF and PC are funded by NHMRC Research Fellowships. JEB and DS are funded by Heart Foundation Fellowships.
Competing interests JEB and JF have provided unpaid consultancy assistance to the NHFA. The NHFA was not involved in this study beyond providing campaign information.
Provenance and peer review Not commissioned; externally peer reviewed.