Article Text

Abstract
Multiple publications have addressed the under-representation of women in the cardiology workforce, and indeed in leadership positions and procedural subspecialities, despite gender parity among medical school graduates. The work–life balance does not appear to be the only determining factor since other specialties such as obstetrics have a adequate representation of women. Vlachadis Castles et al report the results from their online survey of 452 female doctors (both trainees and specialists) from Australia and New Zealand, 13% of whom were women in cardiology. Female cardiologists reported working longer hours and more on-call commitments; significantly fewer women in cardiology reported a balanced life, or that cardiology was family friendly or female friendly, despite a greater earning capacity and an overwhelming majority agreeing that they were professionally challenged whilst intellectually stimulated in their jobs. Our editorial addresses the deterrents to women in cardiology seeking leadership opportunities in all areas including academic, administrative and research positions.
- ethics
- medical
- delivery of health care
- health care economics and organizations
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Much has been discussed about the ‘leaky pipeline’ of women in cardiology globally. There is significant under-representation of women in the cardiology workforce, and indeed in leadership positions and procedural subspecialities, despite gender parity among medical graduates.1 2 A number of diverse challenges in attracting and indeed retaining women in cardiology have been identified (Box 1), not the least of which is the lack of work–life balance in what is often perceived a male-dominated specialty.2–5
Challenges to recruiting and retaining women in cardiology
Perceived work–life imbalance (WLI).
Discrimination.
Radiation concerns.
Opportunities for career progression.
Family planning.
Lack of mentorship.
Unequal financial compensation.
Workplace culture.
The paper by Vlachadis Castles et al report data from an online survey of 452 female doctors (both trainees and specialists) from Australia and New Zealand, 13% of whom were women in cardiology.6 Female cardiologists reported working longer hours and more on-call commitments; significantly fewer women in cardiology reported a balanced life, or that cardiology was family friendly or female friendly, despite a greater earning capacity and an overwhelming majority agreeing that they were professionally challenged while intellectually stimulated in their jobs.6
Poor work–life balance or perceptions thereof, have been a significant deterrent to women choosing cardiology as a subspeciality.2–5 Indeed, worldwide, gender disparity is even greater in procedure-based subspecialities of cardiology, with women comprising only between 4.5% and 7.5% of the interventional cardiology workforce.4 7 However, it is interesting that subspecialities with as demanding on call-hours, such as obstetrics and gynaecology do not have similar issues of recruitment and retention of women; this is testament to the fact that a lack of work–life balance is perhaps not the only deterrent to female uptake of cardiology as a career choice.
A lack of flexibility in working hours, particularly for women with young children has been previously reported,2 4 and could be what deters women from pursuing leadership roles, and opting to completely change specialty or leave academia in favour of private practice, which potentially offers greater flexibility in working hours. Indeed, more recently, there has been a shift towards reframing the issue of work–life balance as ‘work-life integration (WLI)
where the goal is to create synergy between work, home, community, and the private self.8 To this end, a solution might be the introduction of flexible training programmes for trainees and indeed flexible working hours, job sharing and shift work for consultants.1 2
In the UK, where a relatively well-structured less than full-time (LTFT) training programme exists, cardiology LTFT trainees constitute only 4% (compared with 24.2% in paediatrics and 20.3% in obstetrics and gynaecology),9 10 and predominantly (69%) comprise of women.10 However, almost a third of LTFT trainees have perceived that they do not get the same training opportunities as full-time colleagues.10 Additionally, within interventional cardiology some perceive that LTFT is taken less seriously. Perceptions are important, as this may be why far fewer LTFT trainees specify electrophysiology (EP) and interventional cardiology as a career choice. This may remain the status quo until more of the cardiology consultant workforce, male and female have experienced working LTFT to appreciate how valuable it is to enable meeting family commitments and for achieving the work–life integration. Recent real-life examples of female cardiologists in procedure-based specialties have shown that working LTFT is possible and demonstrates no lesser commitment to the specialty.7
This aspect is so important because traditionally, women have tended to bear the brunt of domestic responsibilities, and have reported that these competing demands may have hindered their professional development, pursuit of leadership positions and ability to travel for professional advancement,3 4 thus limiting networking opportunities that are invaluable for career progression and seeking mentorship. It is however encouraging that more recently, significantly more men have also cited family responsibilities affecting their ability to travel for meetings and committee work.4 The contemporary climate of a shift in major meetings to a virtual/ hybrid platform resulting from travel restrictions due to the pandemic. Along with a shift in attitude towards gender disparity, virtual meetings have increased opportunities for female participation in meetings, on panels and as speakers and in the audience.
Workplace culture has been commented on within cardiology internationally.3–5 9 11 Female trainees and consultants have noticed more sexism and discrimination, particularly relating to parenting and domestic responsibilities.4 11 Sexism has detrimental downstream effects often resulting in a lack of professional confidence when working with patients and colleagues, limiting career aspirations, and potentially leading to fewer leadership and professional pursuits.11 Women are also frequently at the receiving end of ‘benevolent sexism’, manifest as being asked about plans for pregnancy during fellowship interviews and also, being cautioned against difficult paths ahead.
Furthermore, gross inaccuracies around radiation, especially misconceptions of potential harms of radiation during pregnancy continue to derail female recruitment into interventional cardiology and EP, many of which are largely unfounded.1 3 These need to be debunked as they deter a talent pool away from a rewarding subspeciality.
So why is there such a push to improve the gender balance in cardiology? A more diverse and better gender-balanced workforce provides more optimal care for patients.12 This is why we need robust methods of enhancing recruitment and retention of women in cardiology, and tangible solutions to tackle the leaky pipeline at varying stages of careers. Attracting the best talent pool to our specialty, irrespective of gender, is certainly in its best interests. As shown in this paper by Vlachadis Castles, and others, younger people—both men and women—increasingly value work–life balance, stable hours and family friendliness in their career choices.3–6 A lack of female mentors and role models in cardiology, has been repeatedly cited as a potential disincentive for the recruitment and retention of women in cardiology,3 7 9 but with the decline of all male panels (manels) this is being addressed.
Perceptions are important, and cardiology needs to better demonstrate that, despite the many challenges, it is certainly possible to combine family life and a rewarding career, inclusive of research, fellowship and high profile, even within procedural-based subspecialities.7 ‘You can’t be what you can’t see’ has been oft-quoted in the realms of academic cardiology. Notably, since the issues of gender disparity were first discussed,1 the workforce gender balance has been improving, but there is still some way to go.
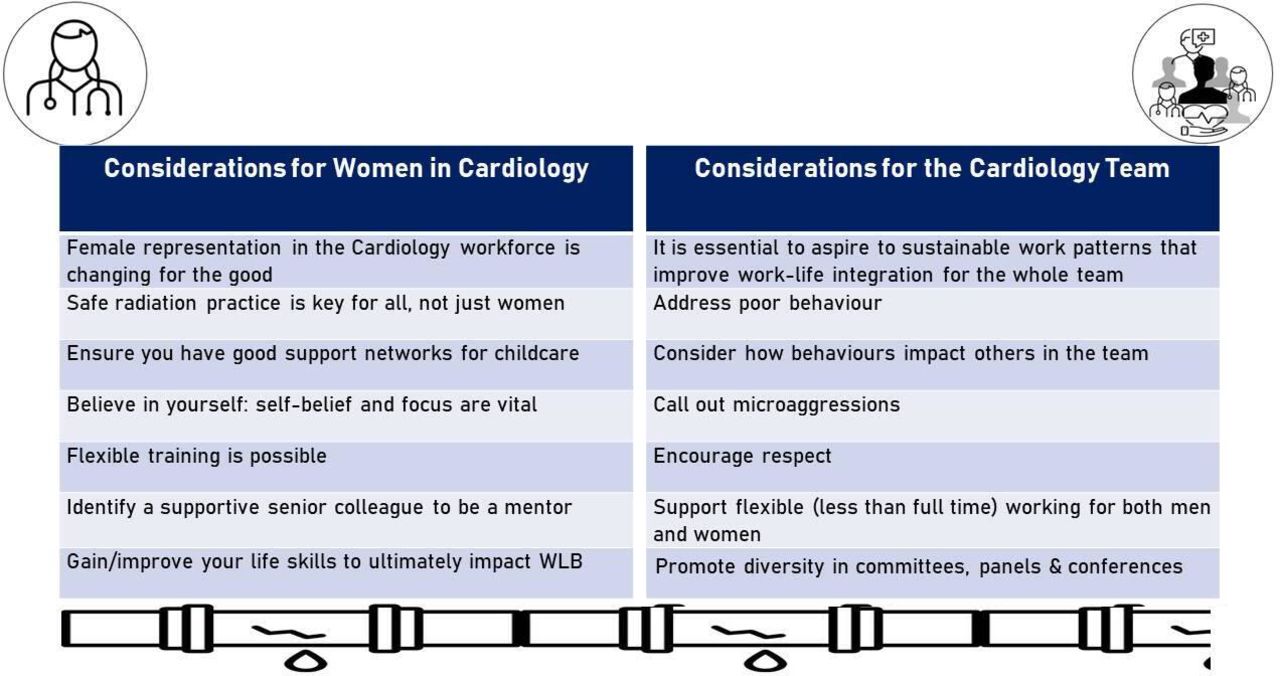
Globally, an active effort is increasingly being made by cardiovascular professional societies and independent organisations such as Women as One, to address the female under-representation within the specialty.2 These include the formation of women in cardiology working groups, networking events, mentorship programmes and awards schemes. But perhaps the most effective interventions come in the form of a collaborative effort by the entire cardiology team to promote diversity in the workforce (figure 1). An active commitment by both male, female and gender-neutral colleagues to support one another, discuss and understand experiences, provide mentorship and promote a more inclusive culture in the workplace will certainly go a long way towards achieving gender parity in cardiology.

{kind=link}
Strategies to enhance recruitment and retention of women in cardiology
Indeed, the issues identified for women in cardiology are relevant for all in cardiology. Ultimately addressing these issues will improve the gender imbalance in our fascinating specialty and help to create a more diverse workforce, resulting in optimal patient care. For all of us, optimal patient care is the common goal. As a biproduct of the process, all working lives will improve. We can see that we are on our way to achieving this change. We just need to accelerate the pace of change.
Ethics statements
Footnotes
Twitter @aayshacader, @mirvatalasnag, @ShrillaB
Contributors All authors contributed equally to this manuscript and reviewed the final submission.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Commissioned; internally peer reviewed.
Linked Articles
- Health care delivery, economics and global health care