Article Text

Abstract
Objective Mild aortic valve stenosis (AS) and aortic valve (AV) sclerosis are associated with diastolic dysfunction and increased mortality in the general population. This study specifically investigated the impact of mild AV disease in heart failure with preserved ejection fraction (HFpEF).
Methods Consecutive patients hospitalised with HFpEF (n=370) underwent assessment of cardiac structure and function and long-term clinical follow-up.
Results In the study cohort, 111 had mild AS (30%), 104 AV sclerosis (28%) and 155 a non-calcified AV (42%). Mild-to-moderate AV regurgitation (AR) was present in 64 (17%). Compared with patients with a normal AV, those with AV disease were older, with worse renal function and more atrial fibrillation. E/e′ increased from non-calcified AV to AV sclerosis to mild AS (13.8 (10.8–16.8) vs 15.0 (10.9–20.0) vs 18.0 (12.7–23.3), respectively; p<0.001)). Left ventricular diastolic pressure–volume relationships were shifted leftwards in patients with AS and AV sclerosis, but not influenced by AR. The left ventricular end-diastolic volume normalised at 20 mm Hg was 117±34 mL, 106±30 mL and 112±30 mL in non-calcified AV, AV sclerosis and mild AS, respectively (p=0.023), while 112±32 mL in mild-to-moderate AR. Over 30 months (IQR, 8–61 months), 247 patients died (67%). The presence of mild AV disease was associated with increased mortality, but this was no longer significant after adjusting for age and sex.
Conclusions Low-grade AV disease is common among patients hospitalised for HFpEF and is associated with older age, atrial arrhythmia, renal dysfunction, higher left heart filling pressures and increased left ventricular chamber stiffness.
- echocardiography
- aortic valve stenosis
- aortic valve insufficiency
- heart failure
- diastolic
Data availability statement
Data are available upon reasonable request. All data relevant to the study are included in the article or uploaded as supplementary information. The data underlying this article will be shared on reasonable request to the corresponding author.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known about this subject?
Mild aortic valve disease is associated with increased cardiovascular risk.
This might be explained by its association with inflammation and obesity.
Both the latter are risk factors to develop heart failure with preserved ejection fraction.
What does this study add?
This study provides a real-world estimate of the prevalence of mild aortic valve disease in heart failure with preserved ejection fraction, showing its presence in the majority of hospitalised patients.
Mild aortic valve stenosis and aortic valve sclerosis, but not mild aortic valve regurgitation, are associated with a leftwards shift in the diastolic left ventricular pressure–volume relationship.
How might this impact on clinical practice?
Mild aortic valve stenosis and aortic valve sclerosis in heart failure with preserved ejection fraction might be interpreted as surrogate markers for more advanced left ventricular stiffening.
Further study is required to clarify the natural history and treatment of aortic valve disease in patients with heart failure and preserved ejection fraction.
Introduction
The prevalence of aortic valve stenosis (AS) is growing as the population grows older, representing the most common primary valve disease leading to intervention.1 Although the aetiology of AS is degenerative in the majority of cases (~80%), recent evidence suggests that aortic calcification results from a complex process that is related to chronic inflammation, lipoprotein deposition, renin-angiotensin system activation and osteoblastic transformation of valvular interstitial cells.1–6 Aortic valve sclerosis is associated with higher C-reactive peptide levels and more advanced coronary artery disease, illuminating one mechanistic link with increased cardiovascular risk, even in the absence of significant haemodynamic obstruction.7 8 Inflammatory biomarkers and a higher genetic risk for obesity are associated with faster progression towards more severe AS.9 10
Both inflammation and obesity also play a central role in the pathophysiology of heart failure with preserved ejection fraction (HFpEF).11 12 Mild aortic valve disease is relatively common in HFpEF, but estimates are based on clinical trial cohorts rather than consecutive samples from the community. Patients with HFpEF characteristically display increased diastolic chamber stiffness and high filling pressures, and these changes may be augmented with even low-grade aortic valve disease, since the latter is also associated with systemic vascular stiffening.13 The present study was undertaken to describe the prevalence, cardiac structural and functional changes associated with low-grade aortic valve disease in HFpEF, including aortic valve sclerosis, mild AS, and mild aortic valve regurgitation (AR) in a well-characterised group of consecutive patients that were hospitalised for decompensated heart failure.
Methods
Study design
This retrospective cohort study includes consecutive patients with HFpEF, who were hospitalised because of signs or symptoms of congestion and treated with intravenous loop diuretics within 24 hours and for a duration of >48 hour at a single tertiary care facility (Mayo Clinic, Rochester, Minnesota, USA) between January 2010 and December 2015. All charts were manually reviewed by a board-certified cardiologist to confirm acute heart failure as the primary diagnosis of admission. Patients with more than mild AS, defined as either a peak aortic jet velocity ≥3 m/s, mean gradient ≥25 mm Hg, or valve area <1.2 cm², were excluded. Furthermore, mitral valve stenosis that was more than mild, defined as either a mean gradient >5 mm Hg or valve area <1.5 cm², was also an exclusion criterion. There was no need for written informed consent as the study was purely observational and retrospective.
Cardiac structure and function
Comprehensive transthoracic echocardiography examinations were performed in agreement with contemporary guidelines and carried out by experienced sonographers.14 The upper limit of normal for peak aortic jet velocity in the Mayo Clinic echo lab is 1.8 m/s. Patients above this threshold were classified as having mild AS. Patients who displayed qualitatively substantial valvular leaflet thickening and/or calcification with a peak aortic jet velocity <1.8 m/s were classified as having aortic valve sclerosis. AR was reported on a semiquantitative scale as normal, trivial, mild, mild–moderate, or moderate after integration of a visual estimate by colour Doppler imaging with available quantitative measurements according to contemporary guidelines.14
Stroke volume was assessed from the LV outflow tract diameter and pulsed-wave Doppler signal. Preload recruitable stroke work (PRSW) was calculated as a load-insensitive parameter of contractility according to the single-beat method described by Lee et al.15 Therefore, stroke work was estimated as the product of stroke volume and mean arterial blood pressure. Next, the left ventricular end-diastolic volume (LVEDV)–stroke work relationship was characterised as the ratio of stroke work over (LVEDV−k LVEDV + (1−k) LVwall) with LVwall=LV mass/1.05 and k=0.0004 LV mass +0.6408. Effective arterial elastance (Ea) was calculated as 0.9 times arterial systolic blood pressure (mm Hg) over stroke volume (mL) and total arterial compliance as stroke volume (mL) divided by arterial pulse pressure (mm Hg).
LV septal and lateral early diastolic tissue velocities (e′) were taken as measures of diastolic function. The time constant of isovolumetric relaxation (τ) was calculated according to the formula τ = (14.7–100 e′)/0.15 by using the septal e′ value.16 17 LV end-diastolic pressure (LVEDP) was estimated by 11.96+0.596 E/e′ (mm Hg) as previously validated against invasive measurements.17 The diastolic stiffness constant (β) was calculated according to the single-beat approach proposed by Klotz et al.18 On the premise that volume-normalised curves of the end-diastolic pressure–volume relationships (EDPVR) share a common shape, this method allows estimation of a curve-fitting constant α in addition to β, hence enabling characterisation of the entire EDPVR from a single set of pressure–volume coordinates. A modified method was used when LVEDP was 27–36 mm Hg to address recognised mathematical limitations of the original equations.19 Because different values of α and β can be associated with similar EDPVRs, groups were compared by use of the LVEDV at a common LVEDP of 20 mm Hg, as in prior studies.19
Outcome assessment
Patient follow-up was initiated on the day of admission and censored at the last follow-up contact that the patient was confirmed to be alive, or 28 August 2019, whatever came first. Vital status was determined from the Mayo Clinic registration database (Accurint) and the Rochester Epidemiology Project death database, which ascertains mortality data from medical records, death certificates, obituaries and notices of death in the local newspapers. Data on all Minnesota deaths are obtained from the State of Minnesota annually.
Statistical analysis
Continuous variables are expressed as mean±SD if normally distributed, or otherwise as median (IQR). The analysis of variance or Kruskal-Wallis H test was used for comparison among groups as indicated, with the independent-samples Student’s t-test or Mann-Whitney U test used for comparison of individual subgroups. Categorical data are expressed as percentages and compared with Pearson’s χ²-test. Generalised linear and nominal logistic regression models were used to provide age-adjusted p values. Correlations were assessed with Spearman’s ρ. The Kaplan-Meier method was employed to construct survival curves with the log-rank test used for comparison between groups. The Cox-proportional hazards model was used to calculate the HR for all-cause mortality with 95% CI and adjust for age and sex. Statistical significance was always set at a two-tailed probability level of <0.05. All statistics were performed using JMP V.14.1.0. (SAS Institute, Cary, North Carolina, USA).
Patient and public involvement
Patients were not involved in the study design as this was a retrospective study.
Results
Study population
A total of 3823 patients with preserved LV ejection fraction (≥50%) were hospitalised for Heart Failure meeting criteria between January 2010 and December 2015 at Mayo Clinic. From this group, 443 were definitely confirmed with a primary diagnosis of decompensated HFpEF, of whom 370 met all inclusion criteria for the study (figure 1). The average age of the population was 77±13 years with 58% women. N-terminal pro-hormone B-type natriuretic peptide (NT-proBNP) levels were available in 345 cases (93%) and were severely elevated (median 2679 ng/L, IQR 1195–5538 ng/L) (table 1). The average H2FPEF score was 6.5±2.0 corresponding to a median HFpEF probability of 98% (IQR, 93%–99%). The median time from meeting inclusion criteria to the echocardiography results was 1 day (IQR, 1–2) and was within 1 week in 312 patients (84%).
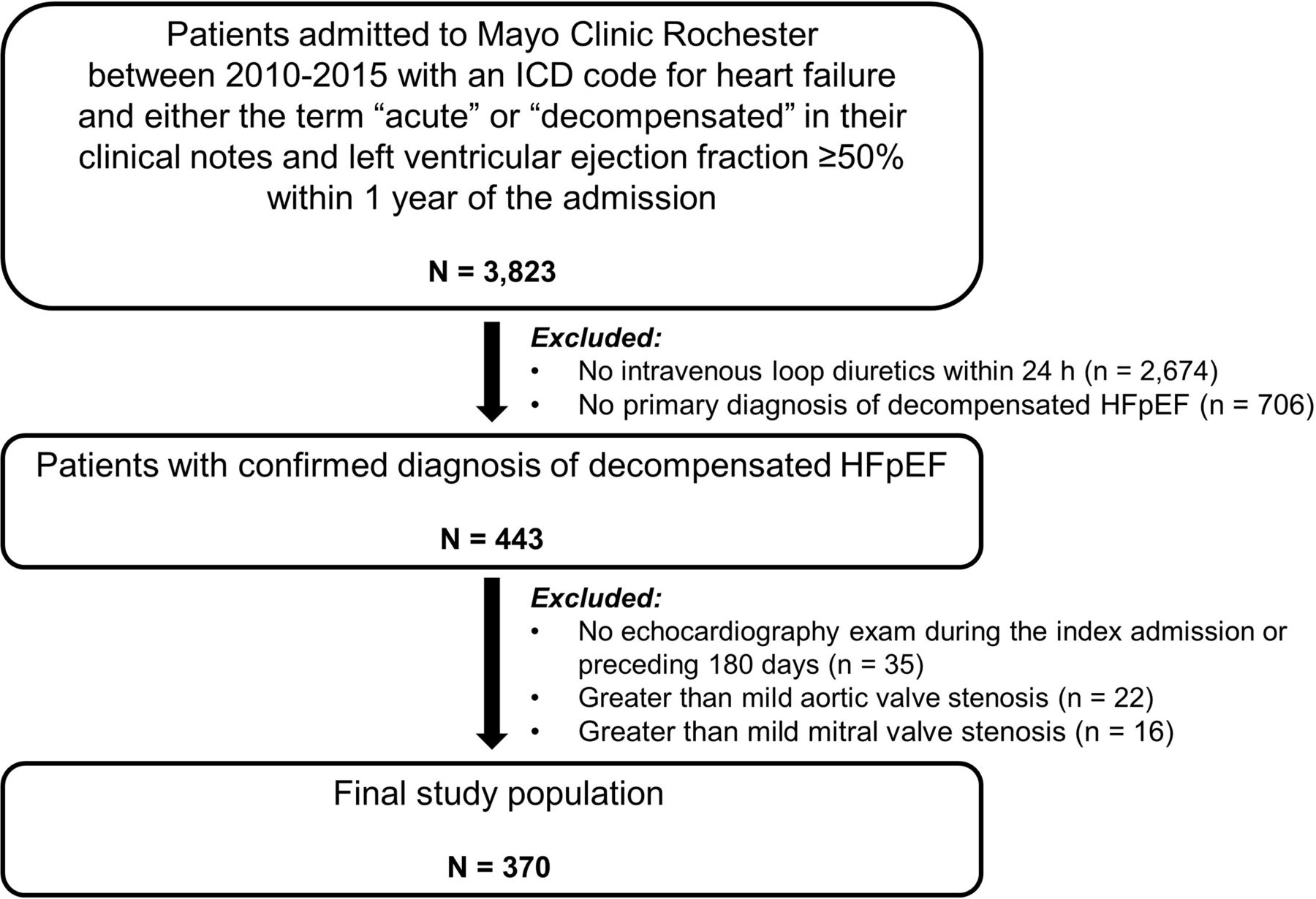
Study flowchart. HFpEF, heart failure with preserved ejection fraction; ICD, international classification of diseases.
Baseline characteristics of the study population
Prevalence of aortic valve disease
Mild AS was present in 111 patients (30%), 104 patients were found to display aortic valve sclerosis but normal peak aortic jet velocity (28%), and 155 (42%) had a grossly normal, non-calcified aortic valve (figure 2). Using a stricter cut-off for mild AS at peak aortic jet velocity ≥2 m/s, 24 patients were reclassified from mild AS to aortic valve sclerosis, leading to an overall prevalence of 24% for mild AS. As compared with patients with a non-calcified aortic valve, those with aortic valve sclerosis and mild AS were significantly older and had worse renal function. Atrial fibrillation was more prevalent among patients with aortic valve sclerosis, while baseline heart rate was lower in those with mild AS.
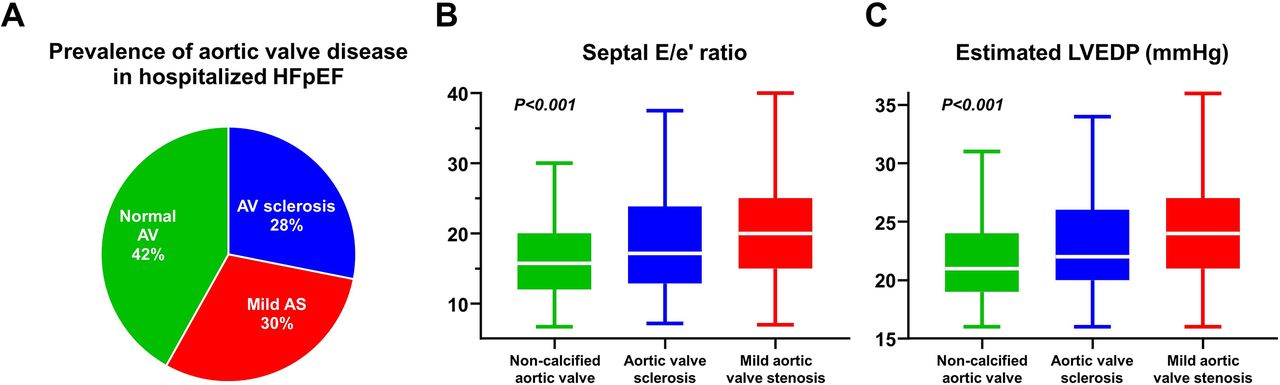
(A) Prevalence of normal aortic valve (AV) (green), AV sclerosis (blue) and mild aortic stenosis (red). Left heart filling pressures as (A) septal E/e′ ratio and (B) estimated left ventricular end-diastolic pressure (LVEDP) according to AV status. HFpEF, heart failure with preserved ejection fraction.
None or trivial AR was present in 306 (82.7%), while 57 had mild AR (15.4%), 5 mild–moderate AR (1.4%) and 2 moderate AR (0.5%) (online supplemental table S1). The presence of mild-to-moderate AR was associated with older age, lower body mass index and body size, more atrial fibrillation and higher NT-proBNP levels.
Supplemental material
Cardiac structure and function
As compared with patients with a non-calcified aortic valve, those with aortic valve sclerosis had smaller ventricular chambers, lower LV mass, larger left atria, lower cardiac output and more tricuspid valve regurgitation (table 2). However, none of these findings remained significant after adjusting for age.
Cardiac structure and function
As compared with patients with a normal aortic valve, those with mild AS displayed slightly higher LV ejection fraction and significantly higher stroke volume (table 2). Peak aortic jet velocity corrected for stroke volume index was similar in patients with aortic valve sclerosis versus a non-calcified aortic valve (3.72±0.98 cm/s/mL/m² vs 3.58±0.91 cm/s/mL/m²; p=0.244) but was significantly elevated in patients with mild AS (5.02±1.22 cm/s/mL/m2; p<0.001). There was extraordinarily little overlap between the patients with mild AS and mild-to-moderate AR (table 2), arguing against a substantial impact of AR on the peak jet velocity measurement.
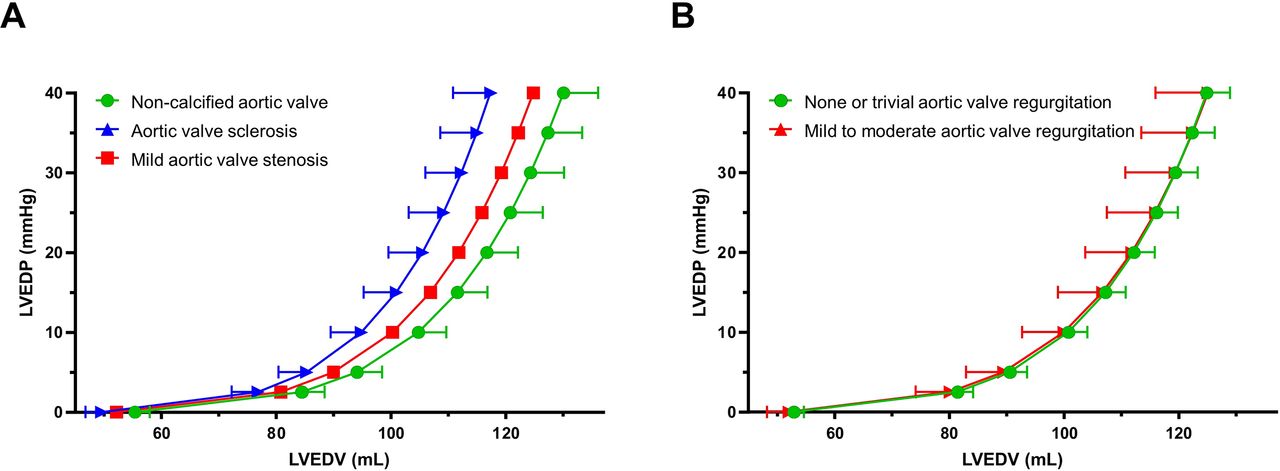
Left heart filling pressures, reflected by the E/e′ ratio and estimated LVEDP, increased in a graded fashion from patients with a non-calcified aortic valve over those with aortic valve sclerosis to mild AS (table 2; figure 2). There was a modest but significant correlation between septal E/e′ ratio and peak aortic jet velocity (Spearman’s ρ=0.25; p<0.001). The EDPVR was shifted leftward in patients with aortic valve disease, to the greatest extent in patients with aortic sclerosis and to lesser extent in patients with mild AS (figure 3). The LVEDV normalised at an LVEDP of 20 mm Hg was 117±34 mL, 106±30 mL and 112±30 mL in non-calcified aortic valve, aortic valve sclerosis and mild AS, respectively (p=0.023).

Mean left ventricular end-diastolic pressure–volume relationships for patients with aortic valve sclerosis and mild stenosis (A) and aortic regurgitation (B). LVEDP, left ventricular end-diastolic pressure; LVEDV, left ventricular end-diastolic volume.
Patients with mild to moderate versus none or trivial AR had a larger LV end-diastolic volume index, larger left atria, a slightly lower ejection fraction, and higher left heart filling pressures, reflected by the E/e′ ratio and estimated LVEDP (online supplemental table S2). The EDPVR was virtually superimposable in patients with or without AR (figure 3). The LVEDV normalised at LVEDP 20 mm Hg was 112±32 mL in mild-to-moderate AR (p=0.937 vs no AR).
All-cause mortality and aortic valve disease
Over 30 months (IQR, 8–61 months), 247 patients died (67%), corresponding to 21.3 deaths per 100 patient years of follow-up. Aortic valve sclerosis (25.8 deaths per 100 patient years; p=0.008), mild AS (26.8 deaths per 100 patient years; p=0.003), and mild-to-moderate AR (28.7 deaths per 100 patients years; p<0.001) were each associated with increased risk for all-cause mortality in univariate analyses when compared with patients with a normal aortic valve (15.0 deaths per 100 patient years). Median survival (95% CI) was 59 months (51–79 months) in patients with a normal aortic valve, 26 months (19–36 months) in patients with aortic valve sclerosis, 29 months (16–37 months) in patients with mild AS; and 25 months (19–39 months) in patients with mild-to-moderate AR (figure 4).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Time to all-cause mortality according to aortic valve status: (A) aortic valve sclerosis and mild aortic valve stenosis; and (B) mild-to-moderate aortic valve regurgitation.
The HR (95% CI) for all-cause mortality was 1.60 (1.16–2.21) in patients with aortic valve sclerosis, 1.68 (1.23–2.30) in patients with mild AS, and 1.86 (1.29–2.69) in patients with mild-to-moderate AR (table 3). However, after adjusting for age and sex, these results were no longer significant.
All-cause mortality risk according to aortic valve status
The cause of death could be ascertained in 205/247 cases (83%). There were no significant differences in cause of death between patients with a non-calcified aortic valve and patients with aortic valve sclerosis (online supplemental table S3). Patients with mild AS tended to have higher mortality due to comorbid conditions (p=0.048), but a similar risk for heart failure related death (p=0.910).
Discussion
The current study reports the prevalence, pathophysiological implications and the association with outcomes of mild aortic valve disease in a contemporary population of well-characterised patients with HFpEF who were hospitalised for volume overload. The major findings are that (1) low-grade aortic valve disease is very common, present in over half of hospitalised patients with HFpEF; (2) the presence of progressive aortic valve disease, even in the mild range, was associated with greater elevations in left heart filling pressures; (3) aortic valve sclerosis/calcification was associated with a smaller and stiffer left ventricle, while mild AR coincided with a more dilated left ventricle but similar compliance; and (4) low-grade aortic valve disease is not independently associated with risk of death after accounting for age and sex. The present study suggests a novel link between valvular sclerosis/calcification and ventricular stiffening in HFpEF.
The prevalence of AS identified in the present study is greater than the value reported in an analysis from the Prospective Comparison of ARNI with ARB Global Outcomes in HF with Preserved Ejection Fraction (PARAGON-HF) trial. In the latter analysis, mild AS was found in only 10% of patients, although with a slightly more conservative cut-off defining AS (peak aortic jet velocity ≥2 m/s).20 Using the latter definition, the prevalence of mild AS would still have been over two-fold higher (24%) in the present study. The reasons for these discrepant findings likely relate to the facts that patients were younger in PARAGON-HF, with less comorbidity in order to meet the eligibility criteria, whereas patients in this less selected cohort of patients were a decade older, with greater comorbidity burden, and had all been hospitalised. As the present study includes consecutive real-world patients hospitalised because of decompensated HFpEF, it probably offers the best estimate of the true prevalence of aortic valve disease in hospitalised HFpEF.
Patients with mild AS in the present study had a lower heart rate and increased stroke volume when compared with patients with a normal aortic valve. However, the ratio of peak aortic jet velocity to stroke volume was elevated, indicating that the increased valvular gradient was not merely the consequence of increased flow, but rather due to a more rigid valve. It is possible that a larger stroke volume with greater time varying changes in shear stress might contribute to more rapid degeneration and loss of tissue elastance. This would also explain why patients with obesity, who are known to have a higher stroke volume, display accelerated progression of AS.10 11
To maintain this higher stroke volume, prior studies have shown that the myocardium of obese patients consumes more ATP, straining myocardial energy reserves, contributing to exertional impairments.21 Over time, this detrimental energetic impairment may contribute to the progression of HFpEF and its related comorbid conditions. This is consistent with data from the present study, in which patients with aortic valve sclerosis without stenosis had similar stroke volume and heart rate when compared with patients with a normal aortic valve. Apart from being older, with more permanent atrial fibrillation, baseline characteristics were comparable in this former versus latter group. Therefore, patients with aortic sclerosis provide a useful control group to help discern the effects of ageing from those associated with an elevated aortic gradient.
The increased stroke volume in the mild AS group could be explained by a higher contractile state, which is supported by a trend towards higher PRSW, as well lower prevalence of comorbidities including atrial fibrillation and tricuspid regurgitation. The EDPVR suggested increased LV stiffness in patients with aortic valve sclerosis, which was less dramatic in patients with mild AS. We therefore speculate that valvular sclerosis and calcification reflect the effects of ageing and comorbidities on the heart, while the peak jet velocity in mild AS is more related to pressure overload itself. Notably, both conditions were quite common, and both were associated with greater elevations in cardiac filling pressures, estimated by the E/e′ ratio. Given the increased chamber stiffness in these patients, it is possible that they ‘require’ a higher LVEDP to achieve adequate chamber preload, which may complicate attempts to aggressively decongest in the inpatient or outpatient setting.22
Kidney disease was notably more advanced in patients with mild AS or aortic valve sclerosis. Chronic kidney disease has been associated with incident AS and may be an important mechanistic link with HFpEF.23 This may also contribute to the increase in LV diastolic chamber stiffness and estimated LV filling pressures noted among patients with aortic valve disease. Chronic kidney disease could be impugned as either the cause or consequence of a systemic calcific process affecting the aortic valve and potentially the myocardium at the same time, via increased fibroblast growth factor-23, secondary and tertiary hyperparathyroidism, and effects on the calcium-phosphate metabolism.24
Importantly, this study shows that HFpEF is often present even at an early stage of AS, where valve interventions are not performed. This reinforces the point that HFpEF and AS are two common age-related disorders that frequently coexist in the same patient. This coexistence may explain the persistent heightened risk of heart failure readmissions and abnormal exercise haemodynamics after aortic valve intervention in many patients.25 26
Limitations
The HFpEF cohort was restricted to patients who were hospitalised for decompensated heart failure, and results may differ if a broader cohort including more stable, ambulatory patients would be included. The cross-sectional nature of the data limits the ability to make causal inferences in the relationships between aortic valve disease, haemodynamics, and cardiac structure. LV pressures were not directly measured but rather estimated from the E/e′ ratio. While this introduces greater variability compared with invasive measures, this approach has been successfully applied at the population level in multiple prior studies.19 27 Importantly, the same methods were applied to measure LV pressure in all patient groups, so these limitations only affect the precision of our estimates and not the veracity of the conclusions, since the same methods were applied to all patients, eliminating any bias.
Conclusions
Low grade aortic valve disease is quite common among patients hospitalised with HFpEF. The presence of aortic valve sclerosis and mild stenosis identifies groups of patients with HFpEF with greater elevation in filling pressures and increased chamber stiffness. Further study is required to clarify the natural history and treatment of aortic valve disease in patients with HFpEF.
Data availability statement
Data are available upon reasonable request. All data relevant to the study are included in the article or uploaded as supplementary information. The data underlying this article will be shared on reasonable request to the corresponding author.
Ethics statements
Patient consent for publication
Ethics approval
The study complies with the Declaration of Helsinki and the study protocol was approved by the locally appointed ethics committee.
Acknowledgments
The authors thank the staff of the Earl Wood Catheterization Laboratory and the patients who agreed to participate in research, allowing for this study to be completed
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors FHV and BAB designed the study. FHV and YNVR collected the data. FHV wrote the first draft of the manuscript that was subsequently edited and revised by all authors. BAB is responsible for the overall content as a guarantor.
Funding BAB is supported by RO1 HL128526 from the National Institutes of Health. FHV is supported by a Fellowship of the Belgian American Educational Foundation (BAEF) and by the Special Research Fund (BOF) of Hasselt University (BOF19PD04).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.